To follow.
Was this helpful?
Thanks for your feedback!
To follow.
RELATED CHAPTERS
RELATED GUIDANCE
Working Together to Safeguard Children, Chapter 3 (Department for Education)
Under section 17 Children Act 1989, local authorities are under a general duty to provide services for children in need for the purposes of safeguarding and promoting their welfare. A child in need is defined under section 17 as:
a child who is unlikely to achieve or maintain a reasonable level of health or development, or whose health and development is likely to be significantly or further impaired without the provision of services, or a child who is disabled.
Local authorities can also ask other agencies to assist in the delivery of support and services under section 17 of the Children Act 1989, but those agencies are under no legal obligation to do so. However, whilst the duty to deliver support and services under section 17 of the Children Act 1989 is with the local authority, other safeguarding partners may play a critical role in the delivery of services for children and their families. Local safeguarding partners are responsible for setting the strategic direction, vision, and culture of the local multi-agency safeguarding arrangements, including agreeing and reviewing shared priorities, and the resources required to deliver services effectively.
Some children in need may require accommodation because there is no one who has parental responsibility for them, they are lost or abandoned, or the person who has been caring for them is prevented from providing them with suitable accommodation or care. Under section 20 of the Children Act 1989, the local authority has a duty to accommodate such children in need in their area.
Where a child in need is approaching 18 years of age, this transition point should be planned for in advance. This includes where children are likely to transition between child and adult services.
To fulfil this duty, practitioners undertake assessments of the needs of individual children, giving due regard to a child’s age and understanding when determining what, if any, services to provide. Following acceptance of a referral by local authority children’s social care, a social work qualified practice supervisor or manager should initiate a multi-agency assessment under section 17 of the Children Act 1989. The assessment should be led by a lead practitioner and approved by a social work qualified practice supervisor or manager. Local authorities have a duty to ascertain the child’s wishes and feelings and take account of them when planning the provision of services.
For the assessment process, see the Assessments chapter.
Every assessment must be informed by the views of the child as well as the family, and a child’s wishes and feelings must be sought regarding the provision of services to be delivered. Where possible, children should be seen alone. Where a child requests to be seen with a trusted adult, this should be supported. A child’s communication needs should be taken into account.
When assessing children in need and providing services, specialist assessments may be required and, where possible, should be co-ordinated so that the child and family experience a coherent process and a single plan of action.
Assessments should be carried out in a timely manner reflecting the needs of the individual child.
Assessments should determine whether the child is in need, the nature of any services required and whether any specialist assessments should be undertaken to assist the local authority in its decision-making.
Where information gathered during an assessment result in the lead practitioner and social work qualified practice supervisor or manager suspecting that the child is suffering or likely to suffer significant harm, the local authority should hold a strategy discussion to enable it to decide, with other agencies, whether it must initiate enquiries under section 47 of the Children Act 1989 (see Strategy Discussions chapter).
Where the local authority children’s social care decides to provide services, a multi-agency child in need plan should be developed which sets out which organisations and agencies will provide which services to the child and family.
The plan should set clear measurable outcomes for the child and expectations for the parents. The plan should reflect the positive aspects of the family situation as well as the weaknesses, acknowledging any factors beyond the family that may be undermining their capacity to parent or keep their child safe.
Where a child in need has moved permanently to another local authority area, the original local authority should ensure that all relevant information (including the child in need plan) is shared with the receiving local authority as soon as possible. The receiving local authority should consider whether support services are still required and discuss with the child and family what might be needed, based on a timely reassessment of the child’s needs. Support should continue to be provided by the original local authority in the intervening period. The receiving local authority should work with the original local authority to ensure that any changes to the services and support provided are managed carefully.
RELEVANT INFORMATION
Working Together to Safeguard Children (Department for Education)
Guidance – Supporting Families: Early Help System Guide (gov.uk)
See also Early Help Partnership Strategy (opens in Buckinghamshire Safeguarding Children Partnership website)
Early help is support for children of all ages that improves a family’s resilience and outcomes or reduces the chance of a problem getting worse. It is not an individual service, but a system of support delivered by local authorities and their partners working together and taking collective responsibility to provide the right provision in their area. Some early help is provided through ‘universal services’ such as education, family centres and health services. They are universal services because they are available to all families, regardless of their needs. Other early help services are coordinated by a local authority and / or their partners to address specific concerns within a family and can be described as targeted early help. Examples of these include parenting support, mental health support, youth services, youth offending teams and housing and employment services. Early help may be appropriate for children and families who have several needs, or whose circumstances might make them more vulnerable. It is a voluntary approach, requiring the family’s consent to receive support and services offered. These may be provided before and/or after statutory intervention.
Effective provision relies upon local organisations and agencies working together, and may include:
Where appropriate, a lead practitioner should co-ordinate the activity around the family, ensure the assessment and the family plan responds to all needs identified, and lead on ensuring the family co-produce the plan.
Local organisations and agencies should have in place effective ways to identify emerging problems and potential unmet needs of individual children and families. Local authorities should work with organisations and agencies to develop joined-up early help services. In Buckinghamshire, the Family Hub Network brings together early help providers. to support communities, based on a clear understanding of local needs supported by the Joint Strategic Needs Assessment (JSNA) and Early Help Partnership to inform their partnership early help offer.
Multi-agency and multi-disciplinary training will be important in supporting this collective understanding of the demographics and needs of the local community, the local practice framework, and the services available to support children. All practitioners working with children and families, including those in universal services and those providing services to adults with children, need to understand their role in identifying emerging problems and work together to prevent things from getting worse. They need appropriate training so that they:
Practitioners should be alert to the potential need for early help for a child who:
The Early Help Partnership promotes a shared approach to practitioner training and development, through shared access to a wide range of early help training.
All children aged 5 to 16 are legally entitled to a full-time education, suitable to any special educational need. Education is essential for children’s progress, wellbeing and wider development and being in school is a protective factor against wider harms, including exploitation. Where children are not receiving education, either because they are persistently missing school, or are not registered at a school and not receiving a suitable education otherwise, this could be a possible indicator of neglect, abuse or exploitation or could in itself constitute neglect in severe and sustained cases.
Young people aged 16 and 17, including those with special and educational needs and disabilities, are required to participate in education or training until they reach their 18th birthday. They are entitled to an offer of a suitable place in education or training under the September Guarantee. Local authorities are therefore expected to identify and pay particular attention to young people who are not in education, employment or training or whose current activity is not known.
Local authorities also have a statutory duty to secure sufficient suitable education and training provision for all young people aged 16 to 19 and for those up to age 25 with a learning difficulty assessment or, EHC plan, in their area. They should make available to young people aged 13 to 19 and to those up to the age of 25 with a learning difficulty assessment or EHC plan, support that will encourage, enable or assist them to participate in education or training.
As education and childcare settings have daily contact with most children and families, they are uniquely placed to identify concerns and, with partners as appropriate, address them early. Safeguarding professionals, including safeguarding partners and their delegates, should work closely with education and childcare settings to ensure information about children is shared effectively, risks of harm are correctly identified and understood, and children and families receive the services they need. This includes, but is not limited to, information, such as increased absence or mental health problems, which may be indicators that a child has suffered or is at risk of suffering neglect, abuse, and exploitation.
Those working in education and childcare settings need to be aware of how children’s experiences can impact on their mental health, behaviour, attendance and progress at nursery, school, or college. Where children have suffered abuse, neglect and exploitation, or other potentially traumatic adverse childhood experiences, this can have a lasting impact throughout childhood, adolescence and into adulthood.
It is important where children are home educated that relevant information is shared between local authorities, schools, colleges, and other relevant partners. Parents have a right to educate their children at home providing the education is suitable. When a child of school age is not a registered pupil at a school and is not receiving suitable education at home, this could be an indicator of neglect, abuse, or exploitation. Schools must notify the local authority of a child’s removal from the school roll at a non-standard transition point, and they should also share information on a child’s circumstances, especially if already known to children’s social care or if they have an EHC plan.
Where a child and family would benefit from co-ordinated support from more than one organisation or agency (for example, education, health, housing) there should be a multi-agency assessment. These assessments should:
Practitioners should have consideration for specific needs, including, but not exclusive to, family members who may have learning difficulties / disabilities or those whose first language is not English, are care experienced, young parents, fathers or male carers, and parents who identify as LGBT.
If a family does not consent to an early help assessment, practitioners should seek to understand why this is the case, so that they can provide reassurance to the family about their concerns. They should ensure the family has understood the consensual nature of support, and range of services available to meet their needs. The practitioner should consider how the needs of the child could otherwise be met, for example, through provision by universal services that the family already engages with. Practitioners should still inform individuals that their data will be recorded and shared, and the purpose of this explained to them. If a family has chosen not to engage with support in the past, this should not act as a barrier to them accessing support in the future. If at any time it is considered that the child may be a child in need, as defined in the Children Act 1989, a referral should be made to children’s social care. Practitioners should ensure that the family has understood that the support and services provided under section 17 of the Children Act 1989 and are consensual. If there are concerns that the child has suffered significant harm or is likely to do so, a referral should be made immediately to local authority children’s social care.
Good practice should ensure effective join up between specific local early help services and universal services to ensure families can seamlessly transition from universal to more specialist support should a specific need be identified. The Family Hub Network provides a wide range of universal and Level 2 support for children, young people and families and provides a pathway into higher tier services where required. There should be an explicit link to the local area’s offer of short breaks for disabled children, as well as suitably adjusted services to support parents. Evidence should be collated to show their impact, including on those with a particular protected characteristic.
Specific local early help services typically include family and parenting programmes, assistance with school attendance, assistance with health issues including mental health, enabling financial stability, supporting secure housing, responses to emerging concerns in extra-familial contexts, responding to a parent in custody, and help for emerging problems relating to domestic abuse, drug or alcohol misuse. In Buckinghamshire, the Family Hub Network brings together early help providers to support communities as a place-based way of joining-up the planning and delivery of family support services, offering a universal access points for children and families.
Early help services may also focus on improving family functioning and building the family’s own capability to establish positive routines and solve problems. This should be done within a structured, evidence-based practice framework, which is shared across the early help partnership and involves regular review to ensure that real progress is being made. Where family networks are supporting the child and parents, it might be appropriate to use family group decision-making to support work with the family. Some of these services may be delivered directly to parents but should always be evaluated to demonstrate the impact they are having on the outcomes for the child.
RELATED CHAPTERS
RELATED GUIDANCE
Working Together to Safeguard Children 2023 (Department for Education)
REFERRAL INFORMATION
See also Types of Abuse and Neglect chapter
The Children Act 1989 section 31 defines harm as ill-treatment (including sexual abuse and forms of ill-treatment which are not physical) or the impairment of physical or mental health or physical, intellectual, emotional, social or behavioural development including, for example, impairment suffered from seeing or hearing the ill-treatment of another. Where the question of whether harm suffered by a child is significant turns on the child’s health or development, their health or development is to be compared with that which could reasonably be expected of a similar child.
Practitioners should be alert to potential indicators of abuse, neglect, and exploitation, and listen carefully to what a child says, how they behave, and observe how they communicate if non-verbal (due to age, special needs and/or disabilities, or if unwilling to communicate).
Practitioners should never assume that information has already been shared by another professional or family member and should always remain open to changing their views about the likelihood of significant harm.
All practitioners working with children and families, including those in universal services and those providing services to adults with children, need to understand their role in identifying emerging problems. They need appropriate training so that they:
See also Professional Reporting Concerns (BSCP website)
Anyone who has concerns about a child’s welfare should consider whether a referral needs to be made to local authority children’s social care and should do so immediately if there is a concern that the child is suffering significant harm or is likely to do so. Where a child is admitted to a mental health facility, practitioners should make a referral to local authority children’s social care.
Local authority children’s social care has the responsibility for the referral process in their area. This includes specific arrangements for referrals in areas where there are secure youth establishments.
Contact details should be signposted clearly so that children, parents, other family members and community partners are aware of who they can contact if they wish to make a referral, require advice or support.
When practitioners refer a child, they should include any information they have on the child’s developmental needs, the capacity of the child’s parents, carers, or family network to meet those needs and any external factors that may be undermining their capacity to parent. This information may be included in any assessment, including an early help assessment, which may have been carried out prior to a referral into local authority children’s social care. An early help assessment is not a prerequisite for a referral but where one has been undertaken, it should be used to support the referral.
Once the referral has been accepted by local authority children’s social care, a social work qualified practice supervisor or manager should decide, with partners where appropriate, who the most appropriate lead practitioner will be and with the lead practitioner’s agreement, allocate them.
The lead practitioner role can be held by a range of people, including social workers. When allocating the lead practitioner, local authorities and their partners should consider the needs of the child and their family to ensure the lead practitioner has the time required to undertake the role. The lead practitioner should have the skills, knowledge, competence, and experience to work effectively with the child and their family.
For child protection enquiries, the lead practitioner should always be a social worker
Lead practitioners should have access to high quality supervision. Effective supervision can play a critical role in ensuring a clear focus on a child’s welfare and support practitioners to reflect critically on the impact of their decisions on the child and their family. All lead practitioners should also continue to receive appropriate supervision and support for continuing professional development and to maintain professional registration, where appropriate, within their existing line management arrangements.
The responsibility for providing support and services remains with the local authority. Decision-making responsibilities, including the lead practitioner and social work qualified practice supervisor or manager should be set out in the local protocol for assessment.
In response to the referral, the lead practitioner should:
Within one working day of a referral being received, local authority children’s social care should acknowledge receipt to the referrer and a social work qualified practice supervisor or manager should decide next steps and the type of response required. This will include determining whether:
If the lead practitioner decides that no further local authority children’s social care involvement is necessary at this stage, but other action may be necessary, they should refer the child and their family to early help assessment or help from universal and targeted services (see also Early Help chapter).
Decisions on the nature and level of the child’s needs, and the level of actual or likely significant harm, if any, should be reviewed by a social work qualified practice supervisor or manager.
Feedback should be given by local authority children’s social care to the referrer on the decisions taken. Where appropriate, this feedback should include the reasons why a case may not meet the statutory threshold and offer suggestions for other sources of more suitable support.
Practitioners should always follow up their concerns if they are not satisfied with the local authority children’s social care response and should escalate their concerns in line with the Escalation, Challenge and Conflict Resolution Procedure if they remain dissatisfied.
RELATED CHAPTERS
Provision of Support and Services for Children in Need
RELATED GUIDANCE
Working Together to Safeguard Children (Department for Education)
Each child who has been referred to Children’s Social Care, where the threshold is met for statutory intervention, will have an individual assessment to identify the support needs required. If the referral meets threshold for Early Help intervention, a family assessment will be completed.
All agencies and professionals involved with the child, and the family, have a responsibility to contribute to the assessment process. This might take the form of providing information in a timely manner and/or direct or joint work.
The assessment will involve drawing together and analysing available information from a range of sources, including any previous history with services, existing records, obtaining information from professionals in relevant agencies and others in contact with the child and family. Where an Early Help Assessment has already been completed this information should be used to inform the assessment. The child and family’s lived experience, and history should be understood to inform support offered.
Where a child is involved in other assessment processes, it is important that these are coordinated so that the child does not become lost between the different agencies involved and the different procedures. Where there are multiple plans, these should be joined up and developed together so that the child and family experience a single assessment and planning process, which shares a focus on the outcomes for the child.
The Local Assessment Protocol published by Buckinghamshire County Council which sets out local arrangements for how a child’s needs will be managed once a child is referred to Children’s Social Care. This should be referenced alongside these procedures.
Under the Children Act 1989, local authorities have a duty to undertake assessments of the needs of individual children to determine what services to provide and action to take.
A Child in Need is defined under the Children Act 1989 as:
a child who is unlikely to achieve or maintain a satisfactory level of health or development, or their health and development will be significantly impaired, without the provision of services; or a child who is disabled.
In these cases, assessments by a social worker are carried out under Section 17 of the Children Act 1989. Children in Need may be assessed under Section 17 of the Children Act 1989, in relation to their Special Educational Needs, disabilities, or as a carer, or because they have committed a crime. The process for assessment should also be used for children whose parents are in prison and for asylum seeking children.
When assessing Children in Need and providing services, specialist assessments may be required. Where possible, this should be coordinated so that the child and family experience a coherent process and a single plan of action.
Concerns about maltreatment may be the reason for a referral to local authority children’s social care or concerns may arise during the course of providing services to the child and family. In these circumstances, local authority Children’s Social Care must initiate enquiries to find out what is happening to the child and whether protective action is required.
Local authorities, with the help of other organisations as appropriate, also have a duty to make enquiries under Section 47 of the Children Act 1989 if they have reasonable cause to suspect that a child is suffering, or is likely to suffer, significant harm to enable them to decide whether they should take any action to safeguard and promote the child’s welfare. There may be a need for immediate protection whilst the assessment is carried out.
Some Children in Need may require accommodation because there is no one who has Parental Responsibility for them, or because they are alone or abandoned. Under Section 20 of the Children Act 1989, the local authority has a duty to accommodate such Children in Need in their area. Following an application under Section 31A, where a child is the subject of a Care Order, the Local authority, as a Corporate Parent, must assess the child’s needs and draw up a Care Plan which sets out the services which will be provided to meet the child’s identified needs.
Whatever legislation the child is assessed under, the purpose of the assessment is always:
The assessment should be led by a qualified and experienced social worker supervised by a experienced and qualified social work manager.
The date of the commencement of the assessment will be recorded in the electronic database; Liquidlogic Children’s System (LCS).
The qualified social worker should carefully plan that the following are carried out:
If it is determined that a child should not be seen as part of the assessment, this should be recorded by the manager with the reasons.
The parent’s consent should usually be sought, before discussing a referral about them with other agencies, unless this may place the child at risk of significant harm, in which case the manager should authorise the discussion of the referral with other agencies without parental knowledge or consent. The authorisation should be recorded with reasons.
If during the course of the assessment, it is discovered that a school age child is not attending an educational establishment, the social worker should contact the Local Education service to establish a reason for this.
If there is suspicion that a crime may have been committed including sexual or physical assault or neglect of the child, the Police must be notified immediately.
In planning the assessment and in providing the parent and child with feedback, the social worker will need to consider and address any communication issues, for example language or impairment.
Where a child or parent speaks a language other than that spoken by the social worker, an interpreter should be provided. Any decision not to use an interpreter in such circumstances must be approved by the Team Manager and recorded.
Where a child or parent with disabilities has communication difficulties it may be necessary to use alternatives to speech. In communicating with a child with such an impairment, it may be particularly useful to involve a person who knows the child well and is familiar with the child’s communication methods. However, caution should be given in using family members to facilitate communication. Where the child has had a communication assessment, its conclusions and recommendations should be observed.
Children should be seen and listened to and included throughout the assessment process. Their ways of communicating should be understood in the context of their lived experiences within their family, community as well as their behaviour and developmental stage.
All professionals should be aware that children may not feel ready or know how to tell someone that they are being abused, exploited, or neglected, and/or they may not recognise their experiences as harmful. For example, children may feel embarrassed, humiliated, or being threatened.
Assessments, service provision and decision making should regularly review the impact of the assessment process and the services provided on the child so that the best outcomes for the child can be achieved. Any services provided should be based on a clear analysis of the child’s needs, and the changes that are required to improve the outcomes for the child.
Children should be actively involved in all parts of the process based upon their age, developmental stage and identity. Direct work with the child and family should include observations of the interactions between the child and the parents/care givers.
All agencies involved with the child, the parents and the wider family have a duty to collaborate and share information to safeguard and promote the welfare of the child.
All assessments should be planned and coordinated by a social worker and the purpose of the assessment should be transparent, understood and agreed by all participants. There should be an agreed statement setting out the aims of the assessment process.
Planning should identify the different elements of the assessment including who should be involved. It is good practice to hold a planning meeting to clarify roles and timescales as well as services to be provided during the assessment where there are a number of family members and agencies likely to play a part in the process.
Questions to be considered in planning assessments include:
The assessment process can be summarised as follows:
Assessment should be a dynamic process, which analyses and responds to the changing nature and level of need and/or risk faced by the child. A good assessment will monitor and record the impact of any services delivered to the child and family and review the help being delivered. Whilst services may be delivered to a parent or carer, the assessment should be focused on the needs of the child and on the impact any services are having on the child.
Research has demonstrated that taking a systematic approach to assessments using a conceptual model is the best way to deliver a comprehensive analysis. A good assessment is one which investigates the three domains; set out in the assessment Framework Triangle. The interaction of these domains requires careful investigation during the assessment. The aim is to reach an informed decision about the nature and level of needs and/or risks that the child may be facing within their family.
An assessment should establish:
The assessment will involve drawing together and analysing available information from a range of sources, including existing records, and involving and obtaining relevant information from professionals in relevant agencies and others in contact with the child and family. Where an Early Help Assessment has already been completed this information should be used to inform the assessment. The child and family’s history and lived experiences should be sought and understood.
Where a child is involved in other assessment processes, it is important that these are coordinated so that the child does not become lost between the different agencies involved and their different procedures. All plans for the child developed by the various agencies and individual professionals should be joined up so that the child and family experience a single assessment and planning process, which shares a focus on the outcomes for the child.
The social worker should analyse all the information gathered from the enquiry stage of the assessment to decide the nature and level of the child’s needs and the level of risk, if any, they may be facing. The social work manager should provide regular supervision, space for reflection and challenge any assumptions with the social worker as part of this process. An informed decision should be taken on the nature of any action required and which services should be provided. Social workers, their managers and other professionals should be mindful of the requirement to understand the level of need and risk in a family from the child’s perspective and ensure action or commission services which will have maximum positive impact on the child’s life.
When new information comes to light or circumstances change the child’s needs, any previous conclusions should be updated and critically reviewed to ensure that the child is not overlooked as noted in many lessons from Child Safeguarding Practice Reviews.
The child should participate and contribute directly to the assessment process based upon their age, understanding and identity. They should be seen alone and if this is not possible or in their best interest, the reason should be recorded. The social worker should work directly with the child in order to understand their views and wishes, including the way in which they behave both with their care givers and in other settings. The agreed local assessment framework should make a range of age appropriate tools available to professionals to assist them in this work.
The pace of the assessment needs to acknowledge the pace at which the child can contribute. However, this should not be a reason for delay in taking protective action. It is important to understand the resilience of the individual child in their family and community context when planning appropriate services.
Every assessment should be child centred. Where there is a conflict between the needs of the child and their parents/carers, decisions should always be made in the child’s best interests. The parents should be involved at the earliest opportunity unless to do so would prejudice the safety of the child.
The parents’ involvement in the assessment will be central to its success. At the outset they need to understand how they can contribute to the process and what change is expected of them in order to improve the outcomes for the child. The assessment process must be open and transparent with the parents. However, the process should also challenge parents’ statements and behaviour where it is evidenced that there are inconsistencies, questions or obstacles to progress. All parents or care givers should be involved equally in the assessment and should be supported to participate whilst the welfare of the child must not be overshadowed by parental needs. There may be exceptions to the involvement in cases of sexual abuse or domestic abuse for example, where the plan for the assessment must consider the safety of an adult as well as that of the child.
All agencies and professionals involved with the child, and the family, have a responsibility to contribute to the assessment process. This might take the form of providing information in a timely manner and direct or joint work. Differences of opinion between professionals should be resolved speedily but where this is not possible, the local arrangements for resolving professional disagreements should be implemented (see Escalation Challenge and Conflict Resolution Procedure).
It is possible that professionals have different experiences of the child and family and understanding these differences will actively contribute to the understanding of the child / family.
The professionals should be involved from the outset and through the agreed, regular process of review.
The social worker’s supervisor will have a key role in supporting the practitioner to ensure all relevant agencies are involved.
Agencies providing services to adults, who are parents, carers or who have regular contact with children must consider the impact on the child of the particular needs of the adult in question.
Every assessment should be focused on outcomes, deciding which services and support to provide to deliver improved welfare for the child and reflect the child’s best interests. In the course of the assessment, the social worker and the social work manager should determine:
The possible outcomes of the assessment should be decided on by the social worker and the social work manager, who should agree a plan of action setting out the services to be delivered how and by whom in discussion with the child and family and the professionals involved.
The outcomes may be as follows:
The maximum time frame for the assessment to conclude, such that it is possible to reach a decision on next steps, should be no longer than 45 working days from the point of referral. No assessment should be open longer than 30 days without the permission of the Locality Service Manager or Head of Service. If, in discussion with a child and their family and other professionals, an assessment exceeds 45 working days, the social worker and professionals involved should record the reasons for exceeding the time limit on the child’s file.
The assessment plan must set out timescales for the actions to be met and stages of the assessment to progress, which should include regular points to review the assessment. The work with the child and family should ensure that the agreed points are achieved through regular reviews. Where delays or obstacles occur these must be acted on and the assessment plan must be reviewed if any circumstances change for the child.
The social worker’s line manager (or other nominated Team Manager) must review the assessment plan regularly with the social worker and ensure that actions such as those below have been met:
A useful comment from ‘Working Together to Safeguard Children 2023’ to bear in mind for all professionals when reviewing progress:
“The plan should be reviewed regularly to analyse whether sufficient progress has been made to meet the child’s needs. This will be important for neglect cases where parents and carers can make small improvements. In such cases, the test should be whether any improvements in adult behaviour are sufficient and sustained. Practitioners should consider the need for further action and record their decisions. The review points should be agreed with other practitioners supporting the child.”
Recording by all professionals should include information on the child’s development so that progress can be monitored to ensure their outcomes are improving. This is particularly significant in circumstances where neglect is an issue.
Records should be kept of the progress of the assessment on the individual child’s record and in their Chronology to monitor any patterns of concerns.
Assessment plans and action points arising from plans and meetings should be circulated to the participants including the child, if appropriate, and the parents.
The recording should be such that a child, requesting to access their records, could easily understand the process taking place and the reasons for decisions and actions taken.
Supervision records should clearly reflect the reasoning for decisions and actions taken.
The assessment triangle in Working Together to Safeguard Children 2023 provides a model, which should be used to examine how the different aspects of the child’s life and context interact and impact on the child. It notes that quality assessments should:
Figure 1: Assessment Framework (click on the image to enlarge it).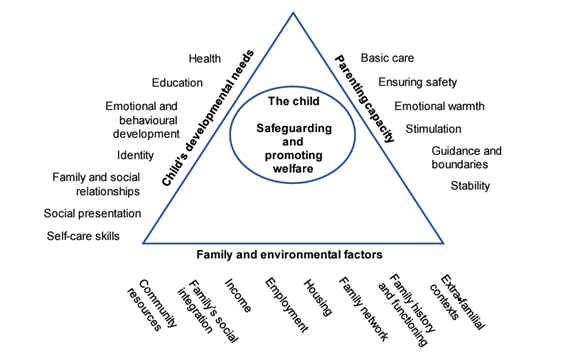
An increasing number of cases involve families from abroad, necessitating assessments of family members in other countries. However, the Court of Appeal has pointed out that it might not be professional, permissible or lawful for a social worker to undertake an assessment in another jurisdiction. CFAB advise that enquiries should be made as to whether the assessment can be undertaken by the authorities in the overseas jurisdiction. UK social workers should not routinely travel overseas to undertake assessments in countries where they have no knowledge of legislative frameworks, cultural expectations or resources available to a child placed there.
When undertaking an assessment of a disabled child, it must also be considered whether it is necessary to provide support under Section 2 of the Chronically Sick and Disabled Persons Act (CSDPA) 1970, and that support must be provided where necessary.
When assessing the needs of a disabled child, it may also be necessary to undertake an assessment of the ability of their carer to provide care for the child.
If a parent carer of a disabled child has support needs, an assessment must be carried out under section 17ZD of the Children Act 1989. Such an assessment must consider whether it is appropriate for the parent carer to provide, or continue to provide, care for the disabled child, in light of the parent carer’s needs and wishes.
If a young carer has support needs, an assessment under section 17ZA of the Children Act 1989 should be carried out.
Such an assessment must consider whether it is appropriate or excessive for the young carer to provide care for the person in question, in light of the young carer’s needs and wishes. The Young Carers’ (Needs Assessment) Regulations 2015 require Local Authorities to look at the needs of the whole family when carrying out a young carer’s needs assessment.
Young carers’ assessments can be combined with assessments of adults in the household, with the agreement of the young carer and adults concerned.
Any assessment of children in secure youth establishments should take account of their specific needs. In all cases, the local authority in which a secure youth establishment is located is responsible for the safety and welfare of the children in that establishment.
The host local authority should work with the governor, director, manager or principal of the secure youth establishment and the child’s home local authority, their relevant Youth Offending Team and, where appropriate, the Youth Custody Service to ensure that the child has a single, comprehensive support plan.
Where a child becomes looked-after, as a result of being remanded to Youth Detention Accommodation (YDA), the child’s needs must be assessed before taking a decision. This information must be used to prepare a Detention Placement Plan (DPP), which must set out how the YDA and other practitioners will meet the child’s needs whilst the child remains remanded. The DPP must be reviewed in the same way as a care plan for any other looked-after child.
Working Together to Safeguard Children 2023 also details the support required for children that may be experiencing abuse and exploitation outside the family home. This is often referred to as “extra-familial harm”
Forms of extra-familial harm include exploitation by criminal and organised crime groups and individuals (such as county lines and financial exploitation), serious violence, modern slavery and trafficking, online harm, sexual exploitation, teenage relationship abuse, and the influences of extremism which could lead to radicalisation.
Working Together to Safeguard Children 2023 outlines where children may be experiencing extra-familial harm, Children’s Social Care assessments should determine whether a child is in need under section 17 of the Children Act 1989 or whether to make enquires under Section 47 of the same Act, following concerns that the child is suffering or likely to suffer significant harm.
Working Together to Safeguard Children 2023 outlines that a good assessment where extra-familial harm is identified should:
Where there are concerns that more than one child may be experiencing harm in an extra-familial context, practitioners should consider the individual needs of each child as well as work with the group. Practitioners will need to build an understanding of the context in which the harm is occurring and draw on relevant knowledge and information from the children and wider partners in order to decide on the most appropriate interventions.
Practitioners should consider the influence of groups or individuals perpetrating harm, including where this takes place online, and identify patterns of harm, risk and protective factors in these contexts. This may include working across safeguarding and community safety partnerships to agree a plan for keeping children safe.
RELATED GUIDANCE
Working Together to Safeguard Children (Department for Education)
This chapter considers the different types of abuse and neglect as specified in Working Together to Safeguard Children (Department for Education). Practitioners should not limit their view of what constitutes abuse or neglect, as they can take many forms. The circumstances of the individual case should always be considered.
All forms of physical and/or emotional ill-treatment, sexual abuse, neglect, or negligent treatment or commercial or other exploitation, resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power.
A form of maltreatment of a child or young person. Somebody may abuse or neglect a child by inflicting harm, or by failing to act to prevent harm. Harm can include ill treatment that is not physical as well as the impact of witnessing ill treatment of others. This can be particularly relevant, for example, in relation to the impact on children of all forms of domestic abuse, including where they see, hear, or experience its effects. Children may be abused in a family or in an institutional or extra-familial contexts by those known to them or, more rarely, by others. Abuse can take place wholly online, or technology may be used to facilitate offline abuse. Children may be abused by an adult or adults, or another child or children.
Where an individual or group takes advantage of an imbalance of power to coerce, control, manipulate or deceive a child or young person under the age of 18 into any criminal activity:
a) in exchange for something the victim needs or wants; and / or
b) for the financial or other advantage of the perpetrator or facilitator; and/or
c) through violence or the threat of violence.
The victim may have been criminally exploited even if the activity appears consensual. Child criminal exploitation does not always involve physical contact; it can also occur through the use of technology.
For more information see, Multi Agency Child Exploitation Protocol
Child sexual exploitation is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity:
a) in exchange for something the victim needs or wants; and/or
b) for the financial advantage or increased status of the perpetrator or facilitator.
The victim may have been sexually exploited even if the sexual activity appears consensual. Child sexual exploitation does not always involve physical contact; it can also occur through the use of technology.
For more information see Sexual Exploitation and Abuse (including Organised Abuse)
The persistent emotional maltreatment of a child so as to cause severe and persistent adverse effects on the child’s emotional development. It may involve conveying to a child that they are worthless or unloved, inadequate, or valued only insofar as they meet the needs of another person. It may include not giving the child opportunities to express their views, deliberately silencing them, or making fun of what they say or how they communicate. It may feature age or developmentally inappropriate expectations being imposed on children. These may include interactions that are beyond a child’s developmental capability, as well as overprotection and limitation of exploration and learning, or preventing the child participating in normal social interaction. It may involve seeing or hearing the ill-treatment of another. It may involve serious bullying (including cyber bullying), causing children frequently to feel frightened or in danger, or the exploitation or corruption of children. Some level of emotional abuse is involved in all types of maltreatment of a child, though it may occur alone.
See also Supporting Children at Risk of, or Experiencing, Harm Outside the Home chapter
Children may be at risk of or experiencing physical, sexual, or emotional abuse and exploitation in extra-familial contexts. Extra-familial contexts include a range of environments outside the family home in which harm can occur. These can include peer groups, school, and community / public spaces, including known places in the community where there are concerns about risks to children (for example, parks, housing estates, shopping centres, takeaway restaurants, or transport hubs), as well as online, including social media or gaming platforms.
While there is no legal definition for the term extra-familial harm, it is widely used to describe different forms of harm that occur outside the home. Children can be vulnerable to multiple forms of extra-familial harm from both adults and/or other children. Examples of extra-familial harm may include (but are not limited to): criminal exploitation (such as county lines and financial exploitation), serious violence, modern slavery and trafficking, online harm, sexual exploitation, child-on-child (non-familial) sexual abuse and other forms of harmful sexual behaviour displayed by children towards their peers, abuse, and/or coercive control, children may experience in their own intimate relationships (sometimes called teenage relationship abuse), and the influences of extremism which could lead to radicalisation.
Financial exploitation can take many forms. It can include exploitation which takes place for the purpose of money laundering. This is when criminals target children and adults and take advantage of an imbalance of power to coerce, control, manipulate or deceive them into facilitating the movement of illicit funds. This can include physical cash and / or payments through financial products, such as bank and cryptocurrency accounts.
The persistent failure to meet a child’s basic physical and / or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to:
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs.
A form of abuse which may involve hitting, shaking, throwing, poisoning, burning, or scalding, drowning, suffocating, or otherwise causing physical harm to a child. Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child.
The Child Protection Evidence Systematic Review on Bruising (RCPCH) found that bruising was the most common injury in children who have been abused. However, it is also a common injury in children who have not been abused, and can be caused by accidental bumps or falls for example. The exception to this is infants or children who are not independently mobile, where accidental bruising is rare (0-1.3%). A child who is not independently mobile is one who cannot crawl, cruise, bottom shuffle or roll over.
The number of bruises a child sustains through everyday activity increases as they get older and their level of independent mobility increases.
A report from the Child Safeguarding Practice Review Panel recommends that bruising in children who are not independently mobile is reviewed by a health professional who has the appropriate expertise to assess the nature and presentation of the bruise, any associated injuries, and to consider the circumstances of the presentation including the developmental stage of the child, whether there is any evidence of a medical condition that could have caused or contributed to the bruising, or a plausible explanation for the bruising.
A multi-agency discussion to consider any other information on the child and family and any known risks, and to jointly decide whether any further assessment, investigation or action is needed to support the family or protect the child is also recommended. This multi-agency discussion should always include the health professional who reviewed the child.
See also: Bruises on Children: Core Info Leaflet (NSPCC Learning).
Involves forcing or enticing a child or young person to take part in sexual activities, not necessarily involving a high level of violence, whether or not the child is aware of what is happening. The activities may involve physical contact, including assault by penetration (for example, rape or oral sex) or non-penetrative acts, such as masturbation, kissing, rubbing, and touching outside of clothing. They may also include non-contact activities, such as involving children in looking at, or in the production of, sexual images, watching sexual activities, encouraging children to behave in sexually inappropriate ways, or grooming a child in preparation for abuse. Sexual abuse can take place online, and technology can be used to facilitate offline abuse. Sexual abuse is not solely perpetrated by adult males. Women can also commit acts of sexual abuse, as can other children.
The Children Act 1989 section 31defines harm as ill-treatment (including sexual abuse and forms of ill-treatment which are not physical) or the impairment of physical or mental health or physical, intellectual, emotional, social or behavioural development including, for example, impairment suffered from seeing or hearing the ill-treatment of another. Where the question of whether harm suffered by a child is significant turns on the child’s health or development, their health or development shall be compared with that which could reasonably be expected of a similar child.
RELATED GUIDANCE
Working Together to Safeguard Children (Department for Education)
Working Together to Safeguard Children Flowchart 3: Immediate Protection (Department for Education)
Where there is a risk to the life of a child or a likelihood of serious immediate harm, whether from inside or outside the home, the local authority, the police (including British Transport Police) or NSPCC should use their statutory child protection powers to act immediately to secure the safety of the child, as set out in Section 46 of Children Act 1989.
If it is necessary to remove a child from their home, a local authority must, wherever possible and unless a child’s safety is otherwise at immediate risk, apply for an Emergency Protection Order (EPO). Police powers to remove a child in an emergency should be used only in exceptional circumstances where there is insufficient time to seek an EPO or for reasons relating to the immediate safety of the child.
An EPO, made by the court, gives authority to remove a child, or prevent a child being removed from a hospital or other place the child is being accommodated, and places them under the protection of the applicant.
When considering whether emergency action is necessary, the local authority or the police should always consider the needs of other children in the same household or in the household of an alleged perpetrator.
The local authority in whose area a child is found in circumstances that require emergency action (the first authority) is responsible for taking emergency action. If the child is looked after by, or the subject of a child protection plan in another authority, the first authority must consult the authority responsible for the child. Only when the second local authority explicitly accepts responsibility (to be followed up in writing) is the first authority relieved of its responsibility to take emergency action.
Planned emergency action will normally take place following an immediate strategy discussion (see Strategy Discussions chapter). Social workers, the police or NSPCC should:
An Emergency Protection Order (EPO) enables the child to be removed from where they are, or to be kept where they are, if this is necessary to provide immediate short-term protection. Any person may apply for an EPO, although in practice the vast majority of applications are made by local authorities.
On receipt of an application, the court can only make an EPO if it is satisfied that there is reasonable cause to believe that the child is likely to suffer significant harm if they:
Where the applicant is the local authority or the NSPCC, an emergency protection order may also be made if enquiries (in the case of local authorities, made under section 47) are being frustrated by unreasonable refusal of access to the child, and the applicant has reasonable cause to believe that access is needed as a matter of urgency.
If there is a need for further investigation of the child’s health and development but they are not considered to be in immediate danger, then the local authority should apply for a child assessment order.
An EPO gives authority to the local authority to remove a child to accommodation provided by or on behalf of the applicant. It also confers upon the person in whose favour it is made (usually the local authority) limited parental responsibility for the child. That parental responsibility must only be exercised to the extent that is necessary to safeguard the child’s welfare. Applications for an EPO are a very serious step and the court must be satisfied that the EPO is both necessary and proportionate and that there is ‘no less radical form of order available’.
Its duration is limited to a maximum period of eight days, with a possible extension of up to a further seven days, to a maximum of 15 days. Applications to extend can be made by the original applicant, with the court being able to grant an extension if it has reasonable cause to believe that the child concerned is likely to suffer significant harm if the order is not extended. During the order the child must be permitted to have reasonable contact with their parents and other significant individuals, unless the court directs otherwise. The court may also give specific directions with regard to contact, and about medical or psychiatric examination or other assessment of the child.
The court can attach an exclusion requirement to an EPO which can exclude the relevant person from the home, and from a designated area around the home. A power of arrest can be attached to the exclusion requirement.
The court has the power to grant orders without notice being given to parents or on short notice, but will only consider applications without notice in high risk cases where the child’s safety would be endangered if the parents knew of the application, or for other reasons it is not possible to notify them.
When an EPO is in force and the applicant has removed the child, the applicant is under a duty to return the child to the care of their parents as soon as it is safe to do so, even if the order is still in force.
In situations where those looking after the child do not readily agree to hand the child over, the EPO provides a formal direction to any person who is in a position to do so to comply with any request to produce the child to the applicant. If the applicant for an EPO does not know the whereabouts of a child, but that information is held by another person, the court may order that person to disclose the information when requested to do so by the applicant. This provision is intended to ensure that access to the child is not frustrated by information being withheld from the applicant.
The Act also gives the courts power to authorise an applicant to enter and search specified premises for a child who is the subject of an EPO.
If the applicant believes there may be another child on the premises which is to be searched, who ought also to be the subject of an EPO, they should always seek an order authorising them to search for that child as well. Where the applicant cannot name the child, they should be described as clearly as possible in the order.
If a second child is found on the premises and the applicant is satisfied that there are sufficient grounds for making an EPO, the order authorising the search for the second child has effect as if it were an EPO. The authorised person must report the result of the search to the court and, what action was taken and/or is planned as a result. The court should also be told whether the order providing the power to search for the child is deemed to have the effect of an EPO, on the basis that the applicant is satisfied that the grounds for making an EPO exist in respect of that second child.
If an authorised person is, or is likely to be, obstructed from exercising their powers under the EPO the court can issue a warrant authorising any police officer to assist the authorised person in entering and searching the named premises. The warrant will authorise the police officer to use reasonable force if necessary in order to assist the applicant in the exercise of their powers to enter and search the premises for the child. If an applicant gains access and finds the child is not harmed and is not likely to suffer significant harm they should not remove the child. The power to remove the child would persist if the circumstances changed and the order was still in force.
There is no right of appeal against an EPO, however the child, a parent of the child, any person who is not a parent but who has parental responsibility for them, or any person with whom they were living immediately before the making of the EPO, may apply to the court for an EPO to be discharged: This right to apply to discharge an EPO is limited to those who did not receive notice of the EPO and were not present at the hearing.
The police have specific powers to protect children under Part V of the Children Act 1989. These should only be used in exceptional circumstances where there is insufficient time to apply for an Emergency Protection Order, or for reasons relating to the immediate safety of the child.
Where a police officer has reasonable cause to believe that a child would otherwise be likely to suffer significant harm they may remove the child to suitable accommodation and keep them there. Alternatively, they may take such steps as are reasonable to ensure that the child’s removal from hospital, or other place in which they are being accommodated, is prevented.
When a police officer has exercised this power the child is held to be in police protection. No child may be kept in police protection for more than 72 hours.
As soon as is practicable after taking the child into police protection, the case should be inquired into by a designated officer (an officer designated for the purposes of section 46 Children Act 1989 by the chief officer of the police area concerned). On completing the inquiry, the designated officer must release the child from police protection, unless they consider that there is still reasonable cause to believe that the child would be likely to suffer significant harm if released.
Upon taking the child into police protection, the police office concerned (rather than the designated officer) must inform the relevant local authority, and where possible inform the child of the steps that have been taken, the reasons for taking them and of any further steps that may be taken. The officer should also take steps to enable the child to be moved to accommodation provided by the local authority. The officer should also take such steps as are reasonably practicable to inform the child’s parents and those with parental responsibility.
The local authority has concurrent duties to make enquiries about whether it should take any action to safeguard or promote the child’s welfare. One such course of action is for the local authority to ask the police to apply for an EPO.
The designated officer has a number of additional responsibilities. They may apply, on behalf of the local authority in whose area the child is ordinarily resident, for an emergency protection order to be made in respect of the child. The EPO application may be made whether or not the authority knows of it or agrees to it being made.
Neither the officer concerned, the designated officer (nor the local authority) acquires parental responsibility for the child. The designated officer must nevertheless do what is reasonable in all the circumstances to promote the child’s welfare.
The designated officer must allow the following persons to have such contact with the child as, in their opinion, is both reasonable and in the child’s best interests:
A child assessment order enables an assessment of the child’s health or development, or of the way in which they have been treated, to be carried out where significant harm is suspected. Its use is most relevant in circumstances where the child is not thought to be at immediate risk, to the extent that removal from their parents’ care is required, but where parents have refused to cooperate with attempts to assess the child. This may be where the suspected harm to the child appears to be longer-term and cumulative rather than sudden and severe.
It can only be made if the court is satisfied:
A child assessment order may be appropriate where insufficient information is available to justify an application for a care or supervision order and an assessment is needed to help establish facts about the child’s condition.
Before making an application to the court, the local authority should always make enquiries into the child’s circumstances. The nature of the case will dictate the manner in which enquiries should be carried out and the degree of urgency. If possible, before an application is made, the child should have been seen by someone who is competent to form a judgement about the child’s welfare and development. When considering an application for any order, the court will expect to be given details of the enquiries made including, in particular, details of the extent to which, if at all, the enquiries have been frustrated by the failure or refusal of the parents to co-operate.
A child assessment order must specify the date by which the assessment is to begin and will have effect for a specified period, not exceeding 7 days from that date. The local authority should make arrangements in advance of the application, so that any necessary multi-disciplinary consideration of the child’s needs can be completed within the specified period.
The order requires any person who is in a position to do so (usually a parent) to produce the child to the person named in the order, and comply with any directions relating to the assessment included in the order. It does not confer on the local authority parental responsibility for the child, and a child of sufficient understanding to make an informed decision may refuse to consent to the assessment.
When making a child assessment order, the court may make directions about related matters, for example as to whether the assessment should be limited to a medical examination or cover other aspects of the child’s health and development. It also has the power to direct that the child should be kept away from home for a specified period if it is necessary for the purpose of the assessment. In these circumstances it must also give directions as it thinks fit about the contact the child must be allowed with other persons during this period.
If, upon considering an application for a child assessment order, the court is satisfied that there are grounds for making an Emergency Protection Order (EPO), then it should make an EPO instead of a child assessment order. Deliberate refusal by the persons responsible for the child to comply with a child assessment order is very likely to add to concern for the child’s welfare and would probably justify an application by the relevant local authority for an EPO (or a care order) or a request to the police that their police protection powers be exercised.
RELATED GUIDANCE
Working Together to Safeguard Children (Department for Education)
Working Together to Safeguard Children Flowchart 3: Immediate Protection (Department for Education) (opens as PDF)
Whenever there is reasonable cause to suspect that a child is suffering or is likely to suffer significant harm, there should be a strategy discussion involving local authority children’s social care (including the residential or fostering service, if the child is looked after), the police, health, and other bodies such as the referring agency, education, early help, or other practitioners involved in supporting the child. This might take the form of a multi-agency meeting and more than one discussion may be necessary. A strategy discussion can take place following a referral or at any other time, including during the assessment process and when new information is received on an already open case.
The purpose of a strategy discussion is to determine the child’s welfare and plan rapid future action if there is reasonable cause to suspect the child is suffering or is likely to suffer significant harm.
A local authority social worker, health practitioners and a police representative should, as a minimum, be involved in the strategy discussion. Other relevant practitioners will depend on the nature of the individual case but may include those who have concerns about the child and / or those involved in the child’s life, for example:
All attendees should be sufficiently senior to make decisions on behalf of their organisation and agencies. They should be sufficiently skilled and experienced to prepare for and engage with the strategy discussion and be able to critically assess and challenge their own and others’ input.
The discussion should be used to:
It is for the local authority to decide whether to make enquiries and the strategy discussion should inform this decision.
Where there are grounds to initiate an enquiry under section 47 of the Children Act 1989, decisions should be made as to:
The timescale for the assessment to reach a decision on next steps should be based upon the needs of the individual child, consistent with the local protocol and no longer than 45 working days from the point of referral into local authority children’s social care.
The assessment framework should be followed for assessments undertaken under section 47 of the Children Act 1989. The lead practitioner for section 47 enquiries should be a social worker.
Lead practitioners should convene the strategy discussion and make sure they:
Health practitioners should:
The police should:
RELATED CHAPTERS
RELATED GUIDANCE
Working Together to Safeguard Children 2023, Chapter 3 (Department for Education)
Where information gathered following a referral being received, or as part of completing an assessment result in the social worker suspecting that the child is suffering or likely to suffer significant harm, a Strategy Discussion/Meeting should be held. This meeting is usually held within 24 hours, unless a carefully planned response is needed, in which case it should take place within 15 working days and always led by the seriousness of the case. The purpose of a strategy meeting is to decide whether to initiate enquiries under Section 47 of the Children Act 1989. Where such a decision is made the Section 47 Enquiry must be completed within 15 working days.
A multi-agency assessment is the means by which Section 47 Enquiries are carried out. The Child and Family assessment will have commenced at the point of referral and must continue whenever threshold for Section 47 Enquiries are satisfied. Whilst the maximum timescale for a Child and Family assessment to be completed is 45 working days (this can be extended with management authorisation for complex cases), the outcome of enquiries under Section 47 must be available in time for an Initial Child Protection Conference (ICPC). If an ICPC is required, this must be convened within 15 working days of the Strategy Discussion/Meeting when the enquiries were initiated.
A Section 47 Enquiry is carried out whilst continuing with a Child and Family assessment in accordance with the guidance set out in this chapter and following the principles and parameters of a good assessment as set out in the Assessment Procedure. There will need to be a particular emphasis on the issues of concern, the analysis of risk and what needs to be put in place to reduce the risk of harm to the child/children.
Local authority social workers have a statutory duty to lead Section 47 Enquiries. The Police, Health professionals, Teachers and other relevant professionals should support the local authority in undertaking its enquiries. The Children’s Social Care manager has responsibility for authorising a Section 47 Enquiry following a Strategy Discussion.
The Section 47 Enquiry and Child and Family assessment must be led by a qualified social worker from Children’s Social Care, who is responsible for its coordination and completion. The social worker must consult with all other agencies involved with the child and family to obtain a holistic picture of the lived experiences of all children in the household, identifying parenting strengths and protective factors, and any risk factors (unknown and unknown). Enquiries may also need to cover children in other households with whom the alleged offender may have had contact. All agencies consulted are responsible for providing any information known to assist.
A Section 47 Enquiry is initiated to decide whether and what type of action is required to safeguard and promote the welfare of a child who is suspected of, or likely to be, suffering significant harm. The enquiry is carried out by undertaking or continuing with a Child and Family assessment in accordance with the guidelines set out in this chapter and following the principles and parameters of a good assessment (see Assessment Procedure for further details).
The social worker, when conducting a Section 47 Enquiry, must assess the potential needs and safety of any other child in the household of the child in question. In addition, Section 47 Enquiries may be required concerning any children in other households with whom the alleged abuser may have contact.
In determining which professionals should be involved in a Section 47 Enquiry, consideration could include who are the family most likely to cooperate with. In all cases where there is evidence of a known propensity to violence within the family household, consideration should be given to the strategy to be adopted, with Police advice or assistance if appropriate, about how to reduce the risks before any visits take place.
The child must always be seen and communicated with alone in the course of a Section 47 Enquiry by the lead social worker, unless it is contrary to his or her interests to do so. The Strategy Discussion Meeting will plan any interview with the child. The record of Section 47 Enquiry and reports to Child Protection Conferences should include the date(s) when the child was seen alone by the lead social worker and, if not seen alone, who was present and the reasons for their presence.
Before a child is seen or interviewed parental permission must be gained unless there are exceptional circumstances that demonstrate that it would not be in the child’s interests and to do so may jeopardise the child’s safety and welfare. Relevant exceptional circumstances would include:
That the child in question did not wish the parent to be involved at that stage and is competent to take that decision.
In such circumstances, the social worker must take legal advice about how to proceed and whether legal action may be required, for example through an application for an Emergency Protection Order or a Child Assessment Order.
Local authority social workers are responsible for deciding what action to take and how to proceed following Section 47 Enquiries. The outcome of a Section 47 Enquiry must be endorsed by a Team Manager.
A Section 47 Enquiry may conclude that the original concerns are:
Enquiries have revealed that there are no causes for concern. The child may be a Child in Need; however the family do not wish for services to be provided, in which case the case will be closed.
Enquiries have revealed that there is no evidence that the child is suffering, or is likely to suffer, significant harm but there are support needs identified that could be met by the provision of services either under Section 17 of the Children Act 1989 or by signposting the family to another agency. The family are willing for a package of support to be provided or continue to be provided.
Where services are to be provided under Section 17 of the Children Act 1989, the social worker or their Team Manager should convene a Child in Need Meeting within 7 working days to agree a Child in Need Plan.
(Where immediate protective action is required, the advice of Legal Services should be sought)
The social worker should record the information gathered and actions during the course of the enquiry and its outcomes on a Record of Section 47 Enquiries, which should be approved by the Team Manager.
If the local authority decides not to proceed with a Child Protection Conference then other professionals involved with the child and family have the right to request that a Conference be convened, if they have serious concerns that a child’s welfare may not be adequately safeguarded. In the event of a continued difference of opinion, the Escalation, Challenge and Conflict Resolution Procedure should be followed.
The primary focus of this Protocol is to ensure that referrals in respect of children who are suffering or who are likely to suffer significant harm are seen as paramount and that agencies work together with a co-ordinated approach to ensure the safety and well- being of the child.
The Protocol sets out the agreement between Buckinghamshire County Council Children’s Social Care (also covering Buckinghamshire County Council) and Thames Valley Police and Partner agencies. The document aims to clarify key practice expectations around good practice in Section 47 Enquiries and is based on principles within Working Together to Safeguard Children 2023.
When a referral is received by Children’s Social Care indicating that a child has suffered or is likely to suffer significant harm partner agencies should be informed of this and their attendance at a Strategy Meeting requested. Children’s Social Care will decide on which agencies are invited to attend/contribute and will consider suggestions from other agencies.
A Strategy Meeting/Discussions should be convened. For urgent referrals this should take place at the earliest possible point. Good practice indicates this is done within 4 hours from point of referral and no later than 24 hours, unless the referral is complex, i.e. Child Sexual Exploitation (CSE), Fabricated or Induced illness (FII), and this should be done within 72 hours unless the risk is more imminent.
As a minimum, Strategy Meetings/Discussions will involve a Children’s Social Care Manager, Police representative (normally a Sergeant) and an appropriate Health representative.
When strategy meetings are held in the MASH, representatives co-located in the MASH are responsible for identifying the appropriate person from their agency and informing them of the time of the Strategy Meeting/Discussion.
Meetings in the MASH will be held in person and if this is not possible arrangements will be made for participants to contribute by tele-conferencing or MS Teams.
Where necessary a representative from the Thames Valley Police Child Abuse Investigation Unit (CAIU) and the receiving Locality Team should either attend or contribute to the meeting by tele-conference or MS Teams.
A Strategy Meeting/Discussion will be held using the principles above and chaired by a Children’s Social Care Manager mirroring the above process. Police attendance will be either in person if possible, by tele-conference or MS Teams. Health are also required to contribute (as a minimum Children’s Service Care/Health and Police must be present).
The record of the Strategy Meeting/Discussion will be recorded on the Children’s Social Care case management system: Liquidlogic Children’s System (LCS) at the time of the meeting by Children’s Social Care. A copy of the minutes will be given to all attendees at the end of the meeting.
A record of the information provided by partner agencies either involved in the Strategy Meeting/Discussion or otherwise will be kept on LCS.
The Strategy Meeting/Discussion should be the process for agreeing between the involved agencies that based on the referral information, there is reasonable cause to believe that a child is suffering or is likely to suffer significant harm.
Meeting structure:
In all cases the strategy meeting will include the sharing of all information within the knowledge of those agencies represented, relevant to the assessment of significant harm to the child/children concerned. Any gaps in information should be identified and arrangements on how to gain this information should be considered and included as actions were required.
Information shared should include the age, level of understanding, cultural and communication needs of the child/children. These factors are to be considered and addressed in the plan for the investigation.
The Strategy Meeting/Discussion should consider, identify and record the decision in relation how any interview of the victim(s) will be carried out; by whom and within what timescale.
Police and Children’s Social Care must follow the guidance set out in Achieving Best Evidence in Criminal Proceedings (Ministry of Justice), which covers interviewing victims and witnesses, and guidance on using special measures, where a decision has been made to undertake a joint interview of the child as part of the criminal investigations.
There is an expectation that where children are to be interviewed in relation to reasonably suspected criminal offence, the approach to those children will be joint (Police and Children’s Social Care) from the outset, unless there are exceptional circumstances which prevent this. Social Workers should as a minimum observe evidential interviews of children, and where their training and experience is to the required standard, may be materially involved in the process of interviewing children alongside Police.
Any delay in interviewing any of the above (particularly a child who is suspected to be the victim of abuse) should be explained and recorded as being in the best interests of the child.
The extent to which supportive adults/parents will be involved in the process of investigating safeguarding issues should be addressed and agreed upon at the Strategy Meeting/Discussion.
The Police will arrange for the involvement of an Intermediary in cases of a particularly young child or one who has significant communication difficulties.
The Strategy Meeting/Discussion should agree and record whether any specialist assessment (for example forensic or paediatric medical examination) will be required, within what timescales and by whom that will be arranged and facilitated.
Consideration should be given to concerns about any immediate safety issues for the child/children involved and plans for necessary protective action made and recorded. For Children’s Social Care, these should be clearly identified as an interim safety plan on the child’s LCS file.
The aim is that decisions regarding the safety of children in line with Section 47; Children Act 1989 are arrived at within 24 hours of the Strategy Meeting/Discussion. However it is acknowledged that some investigations (according to the level of risk/type of evidence present) may be more urgent than others.
In all cases the Strategy Meeting/Discussion should take place as soon as possible after the referral being received. Where child/children are likely to be at risk of immediate harm, the Strategy Meeting/Discussion should take place immediately and agree a plan to safeguard the child/children during the process of investigation.
If, in exceptional circumstances, these timescales are not met the reasons for this must be clearly recorded on the child’s file, e.g. would further compromise the safety of the child.
The outcome of the investigation will be recorded and documented on the child’s file on LCS and emailed to those agencies involved in the Strategy Discussion/Meeting. This record will reference all relevant information and evidence gathered during the process of the investigation by all agencies involved.
The outcome of a safeguarding investigation will be agreed between those agencies involved in the original Strategy Meeting/Discussion and will be based on the evidence gathered during the investigation. Agreement should be reached about whether the risk of significant harm to the child/children is substantiated, the means of protecting the child and any ongoing assessment or other action required. This will usually be agreed at a Review Strategy Meeting/Discussion.
The primary responsibility of Police Child Abuse Investigation Unit (CAIU) staff is to undertake criminal investigations of suspected, alleged or actual crime relating to child abuse.
Children’s Social Care has the statutory duty to make, or cause to be made, enquiries when circumstances defined in Section 47 of the Children Act 1989, exist.
Where a referral indicates a potential criminal offence, there is an expectation that a joint Police and Children’s Social Care investigation will take place. Police will have primacy with regard to the criminal investigation. Social Care will have primacy with regard to safeguarding of the child.
The joint investigation will usually involve the Police and Social Worker conducting joint interviews and working as co-investigators for the duration of investigation. Though the investigating Social Worker and Police Officer may not work together in undertaking every task during the investigation process, all information forthcoming should be shared between the agencies as soon as practically possible, in order to ensure that the understanding for each agency, views about risk and necessary actions are based on the same levels of understanding about evidence and assessment in the case.
There is a presumption that delay in progressing a safeguarding investigation will prejudice the welfare and could compromise the safety of the child.
Should there be difference of opinion that cannot be resolved cases should be escalated through the escalation process.
A joint decision will be made regarding the appropriate level of intervention and of Police involvement throughout the process, depending on the individual circumstances and context of each case.
Where initial allegations are imprecise or concerns arise gradually, it is likely that agreement will be reached for further assessment to determine whether a child is at risk of significant harm.
If agencies agree a single agency enquiry or investigation is appropriate, there should still be an exchange of relevant information, possible involvement in Strategy Meetings/Discussions and agreement reached as to the feedback required by the non-participating agency. A case may start with single agency status, but further assessment/information indicates a need for joint investigation.
Any decision to terminate enquiries or investigations must be communicated to the other agency for it to consider, and the rationale recorded by both agencies. This decision must be recorded on the child’s file.
The decision regarding single or joint agency investigations should be authorised and recorded by the designated line managers in both the Police (CAIU) and Children’s Social Care, noting which agency is going ahead.
A joint investigation must always be initiated whenever there is an allegation or reasonable suspicion that one of the circumstances below applies, regardless of the likelihood of a prosecution:
Cases of minor injury should always be considered for a joint enquiry/investigation if the child is:
In other cases of minor injury, the circumstances surrounding the incident must be considered to determine the ‘seriousness’ of the alleged abuse. The following factors should be included in any consideration by the Police CAIU and Children’s Social Care:
There will be times that after discussion, or preliminary work, cases will be judged less serious and it will be agreed that the best interests of the child are served by a Children’s Social Care led intervention, rather than a joint investigation.
In all cases, the welfare of the child remains paramount and always takes precedence over the need to commence or conclude any criminal investigation.
Where Children’s Social Care assess that the circumstances fall into one of the following criteria, it may progress single agency enquiries following discussion and agreement with the Police CAIU (and making relevant checks):
Where information is received indicating a person who has been identified as being a risk to children is living in, or has access to, a household where there are children, Children’s Social Care and Police CAIU must discuss the circumstances and agree the need for a single enquiry or joint investigation.
Where a minor crime, initially agreed by Police CAIU as inappropriate of further Police investigation, is subsequently discovered to be more serious, the case must be referred back to the Police CAIU.
Criteria for Police single agency investigations are those where:
Where the Police conduct a single agency investigation out of hours (in response to the duty to respond and take action to protect the child or obtain evidence), Children’s Social Care Emergency Social Work Team must be informed immediately and, if appropriate, a joint investigation commenced.
In all cases where the alleged abuser has current contact with children, a referral should be made to Children’s Social Care for a Strategy Meeting/Discussion to consider joint investigation and the protection of the child victim and other children.
In all cases where Police undertake a single agency investigation, details of any victim aged under 18 must be referred to Children’s Social Care, which is responsible for assessing if the investigation raises any child protection issues and if supportive or therapeutic services are appropriate.
Telephone referrals (sharing information that a child is, or is likely to be, suffering significant harm) must be confirmed in writing using agreed format (‘Record of Child Protection Discussion between the Police and Social Services Supervisors’ forms).
Children’s Social Care and the Police must inform each other of any allegations or suspicions of child abuse or neglect, including ‘stranger abuse’, in line with the Information Sharing Code of Practice. Line managers must be consulted in cases of uncertainty and advice recorded.
RELEVANT INFORMATION
Working Together to Safeguard Children, 2025 (Department for Education)
Working Together to Safeguard Children Flowchart 3: Immediate Protection (Department for Education)
RELATED CHAPTERS
Following section 47 enquiries, an initial child protection conference brings together family members (and the child where appropriate), with the supporters, advocates, and practitioners most involved with the child and family, to make decisions about the child’s future safety, health and development. If concerns relate to an unborn child, consideration should be given as to whether to hold a child protection conference prior to the child’s birth.
The purpose of the child protection conference is to bring together and analyse, in a multi-agency and multi-disciplinary meeting, all relevant information and plan how best to safeguard and promote the welfare of the child and protect them from harm. It is the responsibility of the conference to make recommendations on how organisations and agencies work together to safeguard the child in future.
Practitioners and parents should be provided with clear and accurate information about the conference process to support effective planning. All practitioners should approach the work with parents and carers in line with the principles set out in chapter 1 of Working Together to Safeguard Children (Department for Education).
Conference tasks include:
The conference chair:
Lead practitioners should:
All involved practitioners should:
Safeguarding partners should:
The aim of the child protection plan is to:
Local authority children’s social care should:
Lead practitioners should:
The core group should:
For more information see Core Groups procedure.
The review conference procedures for preparation, decision-making and other procedures should be the same as those for an initial child protection conference.
The purpose of a child protection review conference is to review whether the child is continuing to suffer or is likely to suffer significant harm and review developmental progress against child protection plan outcomes. It is to also consider whether the child protection plan should continue or should be changed.
Lead practitioners should:
All involved practitioners should:
A child should no longer be the subject of a child protection plan if:
Lead practitioners should:
The Core Group is responsible for the implementation and ongoing development and progression of the Child Protection Plan as outlined at the Child Protection Conference (see Child Protection Conferences and the Child Protection Plan).
All agencies represented at the Core Group have a responsibility to ensure that they fulfil their role effectively and in accordance with Working Together to Safeguard Children.
The social worker is the Lead Professional and is responsible for ensuring that the arrangements for Core Groups are clearly communicated to children/young people, parents/carers and all professionals involved in working with the child and family.
However, where a child is subject to a Child Protection Plan, each professional part of the Core Group should also be proactive in identifying the dates for Core Groups and ensure they have all relevant up to date information.
All agencies represented at the Core Group also have a responsibility to progress the Core Group, should the Social Worker for any reason be absent, to avoid and drift and delay in interventions for the child is avoided. This includes ensuring the meeting goes ahead and providing Child Protection Plan updates to the social worker.
The allocated Social Worker and Core Group members are responsible for:
Membership of the Core Group will normally have been identified at the most recent Child Protection Conference and ideally will include:
Flexibility is required regarding who chairs the Core Group and should be dependent upon complexity of the case and best placed relationships with the child and their family. It does not have to be the lead social worker.
Core Groups are key to ensuring the safety of the child and an opportunity to develop positive working relationships with children and families and across agencies, building on the family’s strengths to achieve change. The best interests welfare and safety of the child should always take priority and is to be remembered where there are conflicts of interest between family members in the work of the Core Group.
The first Core Group must take place within 10 working days of the Initial Child Protection Conference.
Following the initial Core Group meeting further meetings should be within six weeks and every six weeks forthwith. It is important to remember that this is a guide and it may be that four weekly core groups are required dependent upon the needs and age of the child.
It is the responsibility of the allocated Chair of the Core Group (from whichever agency) to ensure that core groups record actions so that they can evidence implementation of child protection plans.
It is expected that the Social Worker attends, however if they are unable to, the remaining Core Group members must continue with the meeting and send an update on the outcomes and actions of the Child Protection Plan to the social worker within 2 working days.
The lead social worker can then update and distribute the Child Protection Plan within 5 working days to all attendees and those invited, and ensure it is placed on the child’s file.
Introduction
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
Children Act 1989: Court Orders and Pre Proceedings (Department for Education)
Pre-Proceedings and Family Justice Hub (Research in Practice)
Once the child protection process has been carried out, it may be deemed by the local authority that there is still not sufficient protection of the child by the parents and that the ‘threshold’ for care proceedings (under section 31 Children Act 1989) has been met in principle.
In this instance, the local authority should determine whether to initiate pre-proceedings and follow the Children Act 1989: Court Orders and Pre Proceedings (Department for Education).
This decision should be informed by engagement with other relevant agencies. During this period, the local authority should offer family group decision-making, such as family group conferences, to continue to explore potential placements within the family network and to clarify the realistic options available for the child. At pre-proceedings, records of key discussions with the family can be used as evidence of decision-making (see Practice Direction 12A – Care Supervision and Other Part 4 Proceedings: Guide to Case Management (Justice Department).
The pre-proceedings process acts as the final opportunity for parents to avoid care proceedings. Whilst pre-proceedings may be initiated at this final stage as per Flowchart 6 What Happens After the Child Protection Conference, Including Review? (opens as a PDF), where the local authority considers the ‘threshold’ for care proceedings to be met, proceedings can be initiated at any stage.
The local authority should work in partnership with families and, where possible, any extra support or services needed to support the family should be identified and put in place. There should be clear expectations set with parents about the changes they are required to make.
See also Children Act 1989: Court Orders and Pre Proceedings (Department for Education)
When initiating pre-proceedings, practitioners should review Practice Direction 12A – Care Supervision and Other Part 4 Proceedings: Guide to Case Management (Justice Department). The pre-proceedings checklist in this Practice Direction outlines the documentation that must be prepared in pre-proceedings or before and submitted as part of the local authority application for a court order.
Practitioners and strategic leads can also refer to the Pre-Proceedings and Family Justice Hub (Research in Practice) for access to resources and tools to support the delivery of best practice in pre-proceedings.
RELEVANT INFORMATION
Information Sharing Advice for Safeguarding Practitioners (Department of Education)
Many staff undertake risk assessments, which are carried out within the guidelines and models prescribed by their individual organisations or professions. These assessments are often directly or indirectly relevant to safeguarding and promoting the welfare of children and young people. Local audits and serious case reviews, however, reveal that whilst individual risk assessments may be robustly applied by staff in each agency, often they are done so with insufficient ‘linkage’ to risk assessments completed by other agencies, that may be relevant to the same child/family.
Many staff also become involved in informal risk assessments; identifying risks without this being the primary intention, for example while advising on benefits or demonstrating equipment, they might observe or hear about behaviour that causes concern. Any subsequent referral to another agency would contribute to the overall understanding of risk.
This guidance has been produced to encourage the sharing of relevant information contained in different risk assessments, whether they be formal or informal.
This does not mean that agencies should adopt the same model of risk assessment – the distinct methods and models of individual agencies’ assessments must be maintained, as they draw upon the essential knowledge and focus associated with different professional disciplines.
This guidance aims to:
The sharing of relevant information from risk assessments applies to all agencies working with family members, even where the implications may not be obvious. If when working with adult service users there are changes in behaviour (e.g. changes in offending behaviour or take-up of medication), it is important to always consider the potential impact for any children in the family.
This does not mean that the professional has to assess the impact on the child/children themselves, but that they share the changes in their risk assessment with those who assess risk for the child/children and that they contribute relevant opinions to help others in revising their own risk assessment.
Similarly, if a professional’s work involves assessing risk to children, any changes in a child’s circumstances (e.g. exclusion from school) may need to be shared with those who are working with the parent (who may, for example, be receiving mental health services).
Key questions:
With newly identified risks or changes in risk, always consider who else needs to be informed in both Adult and Children’s Services.
Do not assume that the changes will not be relevant to another agency’s interpretation of risk.
Confirm which agencies/services are involved and share any new or revised risk assessment. Think beyond those agencies currently involved – new risks might require the involvement of different agencies/services.
Information about decreases in risk should also be shared. Not to do so might undermine progress for the service user and prolong service intervention unnecessarily.
Be open and honest with the service user (and/or their family where appropriate) from the outset about why, what, how and with whom information will, or could be, shared, and seek their agreement, unless it is unsafe or inappropriate to do so.
Remember that information may be shared with professionals who need to know in order to promote the wellbeing of a child or young person – the Data Protection Act 2018 is not a barrier to sharing information (see Data Protection chapter). Different agencies may have different processes for sharing information. Professionals should be guided by their agency’s policies and procedures and, where applicable, by their professional code. Further guidance on information sharing is available.
When in doubt about whether to share a risk assessment, seek advice from a line manager or the designated lead for child protection.
When sharing a risk assessment, always specify whether it is currently relevant or historical information.
Ensure that subsequent professional decisions about risks associated with the service user involved are informed by the risks assessments associated with other family members, and vice versa. This might mean inviting a wider group of professionals to professional meetings (or to relevant parts of the meeting) and/or sharing reports (or sections of reports) with other agencies.
Always alert other professionals working with family members when planning or proposing to close the case.
The purpose of this document is to provide practitioners within health, social care and the police with simple guidelines to follow when presented with a child who may need a medical assessment in cases of suspected non-accidental injury, sexual abuse and neglect. It does not apply to children who may need a psychiatric assessment. It has been produced by safeguarding children professionals across the health economy in Buckinghamshire, in consultation with colleagues in Children’s Social Care and the police. The document has been reviewed by the Local Medical Council and the Buckinghamshire Safeguarding Children Partnership.
This guidance details agreed procedures and decision-making pathways to ensure that when a child or young person is alleged or suspected to have suffered significant harm, the child will be medically assessed by a doctor with appropriate skills and expertise following multi-agency agreement/strategy discussion that a medical assessment is appropriate.
When a child has an unexplained or suspicious injury, has symptoms and signs of neglect, or is a suspected victim of child sexual abuse, a medical assessment is usually an essential part of the multi-agency investigation.
The majority of children should be seen during the daytime. Examination of children out of hours is rarely needed other than in cases of acute assault, either for medical or forensic necessity.
Why medical assessment may be needed:
Even when there is multi-agency agreement that a medical assessment is appropriate, consent is sought and the medical is only undertaken with the agreement of the child.
Where the child appears in urgent need of medical attention s/he should be taken to the nearest Accident & Emergency (A&E) department, regardless of age, explanation of injury or any other factor.
A&E staff will contact the on-call paediatric registrar to assess the child if non-accidental injury (NIA), abuse or neglect is suspected. The paediatric registrar will inform the consultant on call.
The paediatrician will refer to Children’s Social Care and the police via telephone on 101 or 999 at the earliest opportunity and then complete the online referral form within 24 hours.
In cases of suspected non-accidental injury, the GP or other health professionals in primary care should:
Except for in cases of child neglect, paediatricians do not accept referrals directly from GPs.
GPs can seek advice from the named doctor during normal working hours from Monday to Friday or from the paediatrician on call out of hours.
Named Doctor: Dr Ash Joshi, 01296 566055 /56
Designated Doctor: Dr Lesley Ray, 07342 064612
Clinical Director Thames Valley Sexual Assault Service (Forensic Doctor): Dr Sheila Paul, 07899 870679
These Buckinghamshire Safeguarding Children Partnership (BSCP) procedures state that medical assessments must be considered when there is a suspicion or allegation of child abuse and/or neglect involving:
Whenever there is reasonable cause to suspect that a child is suffering, or is likely to suffer, significant harm there should be a strategy discussion involving local authority Children’s Social Care, the police, health and other agencies as appropriate.
The strategy discussion will plan the medical assessment, deciding what the objectives of the assessment are, when it needs to take place, who should conduct it and where is the most appropriate venue.
Consideration will be given to the need for any other children in the household to be assessed.
A specific and detailed record must be made of the decision about whether to undertake a medical assessment and its rationale clearly stated.
The strategy discussion must plan what will be explained to parents/carers so that they understand the reason for assessment.
If a criminal prosecution is considered by the police to be a possibility, a statement for court by the paediatrician may be required.
If a criminal investigation is urgent, police action may be taken prior to a full strategy meeting.
The following may give consent to a paediatric assessment:
When a child is looked after under section 20 and a parent has given general consent authorising medical treatment for the child, legal advice must be taken about whether this provides consent for paediatric assessment for child protection purposes (the parent still has full parental responsibility for the child).
A child of any age who has sufficient understanding (generally to be assessed by the doctor with advice from others as required) to make a fully informed decision can provide lawful consent to all or part of a paediatric assessment or emergency treatment.
A young person aged 16 or 17 has an explicit right (s8 Family Law Reform Act 1969) to provide consent to surgical, medical or dental treatment and unless grounds exist for doubting their mental health, no further consent is required.
A child who is of sufficient age and understanding may refuse some or all of the paediatric assessment, though refusal can potentially be overridden by a court.
Wherever possible, the permission of a parent should be sought for children under 16 prior to any paediatric assessment and/or other medical treatment.
Where circumstances do not allow permission to be obtained and the child needs emergency medical treatment, the medical practitioner may:
In non-emergency situations, when parental permission is not obtained, the social worker and manager must consider whether it is in the child’s best interests to seek a court order.
If the child does not require urgent medical care, contact Children’s Social Care First Response Team 01296 383962 / Out of hours 0800 999 7677.
The social worker will contact the on-call consultant paediatrician by ringing the following number and asking the operator for the consultant paediatrician on call:
The consultant will discuss the case with social worker – see above strategy discussion. A suitable time and place for the child to be seen will be arranged. This may not be on the same day as the discussion.
If the child does not require urgent medical care, contact Children’s Social Care First Response Team 01296 383962 / Out of hours 0800 999 7677.
Telephone the community paediatrician on number below and ask to speak to doctor on call for neglect cases:
If the community paediatrician is not available, the social worker’s contact details will be taken and the doctor will return the call within 4 hours or before 5pm, whichever is sooner.
Following a strategy discussion with the social worker, the paediatrician will decide when and where the medical is to take place. These medicals are not urgent but should take place within a timely manner ideally before the initial case conference and definitely before the first review conference. Younger children may need to be seen more quickly.
The appointment for the medical should be sent to the parents/carers, social worker and school nurse/health visitor as appropriate. In cases of neglect all children in the family may be seen for medical assessment.
Local policy with regard to examination in cases of suspected sexual abuse is underpinned by the Guidelines on Paediatric Forensic Examination in relation to Possible Child Sexual Abuse produced by the Royal College of Paediatrics and Child Health (RCPCH), and the Faculty of Forensic and Legal Medicine (FFLM).
The Thames Valley Sexual Assault Referral Centre (SARC) is run by Harmoni for Health and has been named ‘Solace’.
The contact number for Solace is 0300 1303036.
In all cases, medical needs are paramount and come before forensic needs if necessary. If the child requires urgent medical treatment they should be taken to the nearest A&E department.
If the child does not require urgent medical care, contact Children’s Social Care First Response Team 01296 383962 / Out of hours 0800 999 7677.
The timing of the medical depends on the time of the sexual assault (acute or historic) and the pubertal status of the child.
If an urgent forensic medical examination is required, the police should contact Solace who will arrange an appointment with the duty forensic doctor on the SARC rota. If that doctor does not have all the core and case dependent skills required to examine the child, the forensic medical examination should ideally be carried out by a forensic doctor experienced in paediatric examination or, if not available, jointly by the duty forensic doctor and a consultant paediatrician on call.
Professionals can call Solace directly for advice on any sexual assault case regardless of age on 0300 130 3036. They should also contact police/social care as per the flow chart (Appendix A).
Cases of acute sexual assault in pre-pubertal children (aged usually less than 12 years) are rare. These cases require an urgent forensic examination as soon as practicable so that forensic evidence is not lost. Persistence data reveal the opportunity of up to three days to collect samples for foreign DNA from a pre-pubertal child, depending on the type of sexual assault. Research shows this is often reduced to 13 hours in practice.
Cases of acute sexual assault, within the last 7–10 days, in post-pubertal children (usually aged more than 12 years) need an urgent forensic medical examination. The timing of a medical examination needs to balance the welfare of the child with the need to secure forensic evidence. More evidence is likely to be secured the sooner a medical examination takes place, but in achieving this effort should be made to minimise the distress to child. The timing depends on the disclosure but always as soon as possible and usually the same day or night, so that forensic evidence is not lost and distress is minimised. The examination should be carried out by the duty forensic doctor on the SARC rota and should be arranged through the police.
It is important to recognise that urgent examinations to capture forensic evidence such as healing injuries, or provide appropriate treatment such as emergency contraception, may be needed outside the persistent data time scales and this is reflected in the FFLM and the RCPCH service specification for the clinical evaluation of children and young people who may have been sexually abused. In this document it is emphasised that acute examinations may be needed for the above reasons up to 21 days post-alleged event.
Pre-pubertal (children aged usually less than 12 years) and post-pubertal (usually aged more than 12 years) cases where there is delay in reporting sexual abuse (abuse occurred usually more than 21 days) are non- acute cases that do not need an urgent out of hours examination. Police should make arrangements with the forensic doctor.
If you have concerns about medical examinations the named and designated doctors are available for advice and contact details are given below:
Appendix A Flow Charts (opens as a PDF)
Appendix B – Body Map (opens in Word)
To follow.
RELATED CHAPTERS
RELATED GUIDANCE
Working Together to Safeguard Children, Chapter 3 (Department for Education)
Under section 17 Children Act 1989, local authorities are under a general duty to provide services for children in need for the purposes of safeguarding and promoting their welfare. A child in need is defined under section 17 as:
a child who is unlikely to achieve or maintain a reasonable level of health or development, or whose health and development is likely to be significantly or further impaired without the provision of services, or a child who is disabled.
Local authorities can also ask other agencies to assist in the delivery of support and services under section 17 of the Children Act 1989, but those agencies are under no legal obligation to do so. However, whilst the duty to deliver support and services under section 17 of the Children Act 1989 is with the local authority, other safeguarding partners may play a critical role in the delivery of services for children and their families. Local safeguarding partners are responsible for setting the strategic direction, vision, and culture of the local multi-agency safeguarding arrangements, including agreeing and reviewing shared priorities, and the resources required to deliver services effectively.
Some children in need may require accommodation because there is no one who has parental responsibility for them, they are lost or abandoned, or the person who has been caring for them is prevented from providing them with suitable accommodation or care. Under section 20 of the Children Act 1989, the local authority has a duty to accommodate such children in need in their area.
Where a child in need is approaching 18 years of age, this transition point should be planned for in advance. This includes where children are likely to transition between child and adult services.
To fulfil this duty, practitioners undertake assessments of the needs of individual children, giving due regard to a child’s age and understanding when determining what, if any, services to provide. Following acceptance of a referral by local authority children’s social care, a social work qualified practice supervisor or manager should initiate a multi-agency assessment under section 17 of the Children Act 1989. The assessment should be led by a lead practitioner and approved by a social work qualified practice supervisor or manager. Local authorities have a duty to ascertain the child’s wishes and feelings and take account of them when planning the provision of services.
For the assessment process, see the Assessments chapter.
Every assessment must be informed by the views of the child as well as the family, and a child’s wishes and feelings must be sought regarding the provision of services to be delivered. Where possible, children should be seen alone. Where a child requests to be seen with a trusted adult, this should be supported. A child’s communication needs should be taken into account.
When assessing children in need and providing services, specialist assessments may be required and, where possible, should be co-ordinated so that the child and family experience a coherent process and a single plan of action.
Assessments should be carried out in a timely manner reflecting the needs of the individual child.
Assessments should determine whether the child is in need, the nature of any services required and whether any specialist assessments should be undertaken to assist the local authority in its decision-making.
Where information gathered during an assessment result in the lead practitioner and social work qualified practice supervisor or manager suspecting that the child is suffering or likely to suffer significant harm, the local authority should hold a strategy discussion to enable it to decide, with other agencies, whether it must initiate enquiries under section 47 of the Children Act 1989 (see Strategy Discussions chapter).
Where the local authority children’s social care decides to provide services, a multi-agency child in need plan should be developed which sets out which organisations and agencies will provide which services to the child and family.
The plan should set clear measurable outcomes for the child and expectations for the parents. The plan should reflect the positive aspects of the family situation as well as the weaknesses, acknowledging any factors beyond the family that may be undermining their capacity to parent or keep their child safe.
Where a child in need has moved permanently to another local authority area, the original local authority should ensure that all relevant information (including the child in need plan) is shared with the receiving local authority as soon as possible. The receiving local authority should consider whether support services are still required and discuss with the child and family what might be needed, based on a timely reassessment of the child’s needs. Support should continue to be provided by the original local authority in the intervening period. The receiving local authority should work with the original local authority to ensure that any changes to the services and support provided are managed carefully.
RELATED CHAPTERS
RELATED GUIDANCE
Working Together to Safeguard Children 2023 (Department for Education)
REFERRAL INFORMATION
See also Types of Abuse and Neglect chapter
The Children Act 1989 section 31 defines harm as ill-treatment (including sexual abuse and forms of ill-treatment which are not physical) or the impairment of physical or mental health or physical, intellectual, emotional, social or behavioural development including, for example, impairment suffered from seeing or hearing the ill-treatment of another. Where the question of whether harm suffered by a child is significant turns on the child’s health or development, their health or development is to be compared with that which could reasonably be expected of a similar child.
Practitioners should be alert to potential indicators of abuse, neglect, and exploitation, and listen carefully to what a child says, how they behave, and observe how they communicate if non-verbal (due to age, special needs and/or disabilities, or if unwilling to communicate).
Practitioners should never assume that information has already been shared by another professional or family member and should always remain open to changing their views about the likelihood of significant harm.
All practitioners working with children and families, including those in universal services and those providing services to adults with children, need to understand their role in identifying emerging problems. They need appropriate training so that they:
See also Professional Reporting Concerns (BSCP website)
Anyone who has concerns about a child’s welfare should consider whether a referral needs to be made to local authority children’s social care and should do so immediately if there is a concern that the child is suffering significant harm or is likely to do so. Where a child is admitted to a mental health facility, practitioners should make a referral to local authority children’s social care.
Local authority children’s social care has the responsibility for the referral process in their area. This includes specific arrangements for referrals in areas where there are secure youth establishments.
Contact details should be signposted clearly so that children, parents, other family members and community partners are aware of who they can contact if they wish to make a referral, require advice or support.
When practitioners refer a child, they should include any information they have on the child’s developmental needs, the capacity of the child’s parents, carers, or family network to meet those needs and any external factors that may be undermining their capacity to parent. This information may be included in any assessment, including an early help assessment, which may have been carried out prior to a referral into local authority children’s social care. An early help assessment is not a prerequisite for a referral but where one has been undertaken, it should be used to support the referral.
Once the referral has been accepted by local authority children’s social care, a social work qualified practice supervisor or manager should decide, with partners where appropriate, who the most appropriate lead practitioner will be and with the lead practitioner’s agreement, allocate them.
The lead practitioner role can be held by a range of people, including social workers. When allocating the lead practitioner, local authorities and their partners should consider the needs of the child and their family to ensure the lead practitioner has the time required to undertake the role. The lead practitioner should have the skills, knowledge, competence, and experience to work effectively with the child and their family.
For child protection enquiries, the lead practitioner should always be a social worker
Lead practitioners should have access to high quality supervision. Effective supervision can play a critical role in ensuring a clear focus on a child’s welfare and support practitioners to reflect critically on the impact of their decisions on the child and their family. All lead practitioners should also continue to receive appropriate supervision and support for continuing professional development and to maintain professional registration, where appropriate, within their existing line management arrangements.
The responsibility for providing support and services remains with the local authority. Decision-making responsibilities, including the lead practitioner and social work qualified practice supervisor or manager should be set out in the local protocol for assessment.
In response to the referral, the lead practitioner should:
Within one working day of a referral being received, local authority children’s social care should acknowledge receipt to the referrer and a social work qualified practice supervisor or manager should decide next steps and the type of response required. This will include determining whether:
If the lead practitioner decides that no further local authority children’s social care involvement is necessary at this stage, but other action may be necessary, they should refer the child and their family to early help assessment or help from universal and targeted services (see also Early Help chapter).
Decisions on the nature and level of the child’s needs, and the level of actual or likely significant harm, if any, should be reviewed by a social work qualified practice supervisor or manager.
Feedback should be given by local authority children’s social care to the referrer on the decisions taken. Where appropriate, this feedback should include the reasons why a case may not meet the statutory threshold and offer suggestions for other sources of more suitable support.
Practitioners should always follow up their concerns if they are not satisfied with the local authority children’s social care response and should escalate their concerns in line with the Escalation, Challenge and Conflict Resolution Procedure if they remain dissatisfied.
RELATED GUIDANCE
Working Together to Safeguard Children (Department for Education)
This chapter considers the different types of abuse and neglect as specified in Working Together to Safeguard Children (Department for Education). Practitioners should not limit their view of what constitutes abuse or neglect, as they can take many forms. The circumstances of the individual case should always be considered.
All forms of physical and/or emotional ill-treatment, sexual abuse, neglect, or negligent treatment or commercial or other exploitation, resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power.
A form of maltreatment of a child or young person. Somebody may abuse or neglect a child by inflicting harm, or by failing to act to prevent harm. Harm can include ill treatment that is not physical as well as the impact of witnessing ill treatment of others. This can be particularly relevant, for example, in relation to the impact on children of all forms of domestic abuse, including where they see, hear, or experience its effects. Children may be abused in a family or in an institutional or extra-familial contexts by those known to them or, more rarely, by others. Abuse can take place wholly online, or technology may be used to facilitate offline abuse. Children may be abused by an adult or adults, or another child or children.
Where an individual or group takes advantage of an imbalance of power to coerce, control, manipulate or deceive a child or young person under the age of 18 into any criminal activity:
a) in exchange for something the victim needs or wants; and / or
b) for the financial or other advantage of the perpetrator or facilitator; and/or
c) through violence or the threat of violence.
The victim may have been criminally exploited even if the activity appears consensual. Child criminal exploitation does not always involve physical contact; it can also occur through the use of technology.
For more information see, Multi Agency Child Exploitation Protocol
Child sexual exploitation is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity:
a) in exchange for something the victim needs or wants; and/or
b) for the financial advantage or increased status of the perpetrator or facilitator.
The victim may have been sexually exploited even if the sexual activity appears consensual. Child sexual exploitation does not always involve physical contact; it can also occur through the use of technology.
For more information see Sexual Exploitation and Abuse (including Organised Abuse)
The persistent emotional maltreatment of a child so as to cause severe and persistent adverse effects on the child’s emotional development. It may involve conveying to a child that they are worthless or unloved, inadequate, or valued only insofar as they meet the needs of another person. It may include not giving the child opportunities to express their views, deliberately silencing them, or making fun of what they say or how they communicate. It may feature age or developmentally inappropriate expectations being imposed on children. These may include interactions that are beyond a child’s developmental capability, as well as overprotection and limitation of exploration and learning, or preventing the child participating in normal social interaction. It may involve seeing or hearing the ill-treatment of another. It may involve serious bullying (including cyber bullying), causing children frequently to feel frightened or in danger, or the exploitation or corruption of children. Some level of emotional abuse is involved in all types of maltreatment of a child, though it may occur alone.
See also Supporting Children at Risk of, or Experiencing, Harm Outside the Home chapter
Children may be at risk of or experiencing physical, sexual, or emotional abuse and exploitation in extra-familial contexts. Extra-familial contexts include a range of environments outside the family home in which harm can occur. These can include peer groups, school, and community / public spaces, including known places in the community where there are concerns about risks to children (for example, parks, housing estates, shopping centres, takeaway restaurants, or transport hubs), as well as online, including social media or gaming platforms.
While there is no legal definition for the term extra-familial harm, it is widely used to describe different forms of harm that occur outside the home. Children can be vulnerable to multiple forms of extra-familial harm from both adults and/or other children. Examples of extra-familial harm may include (but are not limited to): criminal exploitation (such as county lines and financial exploitation), serious violence, modern slavery and trafficking, online harm, sexual exploitation, child-on-child (non-familial) sexual abuse and other forms of harmful sexual behaviour displayed by children towards their peers, abuse, and/or coercive control, children may experience in their own intimate relationships (sometimes called teenage relationship abuse), and the influences of extremism which could lead to radicalisation.
Financial exploitation can take many forms. It can include exploitation which takes place for the purpose of money laundering. This is when criminals target children and adults and take advantage of an imbalance of power to coerce, control, manipulate or deceive them into facilitating the movement of illicit funds. This can include physical cash and / or payments through financial products, such as bank and cryptocurrency accounts.
The persistent failure to meet a child’s basic physical and / or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to:
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs.
A form of abuse which may involve hitting, shaking, throwing, poisoning, burning, or scalding, drowning, suffocating, or otherwise causing physical harm to a child. Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child.
The Child Protection Evidence Systematic Review on Bruising (RCPCH) found that bruising was the most common injury in children who have been abused. However, it is also a common injury in children who have not been abused, and can be caused by accidental bumps or falls for example. The exception to this is infants or children who are not independently mobile, where accidental bruising is rare (0-1.3%). A child who is not independently mobile is one who cannot crawl, cruise, bottom shuffle or roll over.
The number of bruises a child sustains through everyday activity increases as they get older and their level of independent mobility increases.
A report from the Child Safeguarding Practice Review Panel recommends that bruising in children who are not independently mobile is reviewed by a health professional who has the appropriate expertise to assess the nature and presentation of the bruise, any associated injuries, and to consider the circumstances of the presentation including the developmental stage of the child, whether there is any evidence of a medical condition that could have caused or contributed to the bruising, or a plausible explanation for the bruising.
A multi-agency discussion to consider any other information on the child and family and any known risks, and to jointly decide whether any further assessment, investigation or action is needed to support the family or protect the child is also recommended. This multi-agency discussion should always include the health professional who reviewed the child.
See also: Bruises on Children: Core Info Leaflet (NSPCC Learning).
Involves forcing or enticing a child or young person to take part in sexual activities, not necessarily involving a high level of violence, whether or not the child is aware of what is happening. The activities may involve physical contact, including assault by penetration (for example, rape or oral sex) or non-penetrative acts, such as masturbation, kissing, rubbing, and touching outside of clothing. They may also include non-contact activities, such as involving children in looking at, or in the production of, sexual images, watching sexual activities, encouraging children to behave in sexually inappropriate ways, or grooming a child in preparation for abuse. Sexual abuse can take place online, and technology can be used to facilitate offline abuse. Sexual abuse is not solely perpetrated by adult males. Women can also commit acts of sexual abuse, as can other children.
The Children Act 1989 section 31defines harm as ill-treatment (including sexual abuse and forms of ill-treatment which are not physical) or the impairment of physical or mental health or physical, intellectual, emotional, social or behavioural development including, for example, impairment suffered from seeing or hearing the ill-treatment of another. Where the question of whether harm suffered by a child is significant turns on the child’s health or development, their health or development shall be compared with that which could reasonably be expected of a similar child.
RELATED GUIDANCE
Working Together to Safeguard Children (Department for Education)
Working Together to Safeguard Children Flowchart 3: Immediate Protection (Department for Education) (opens as PDF)
Whenever there is reasonable cause to suspect that a child is suffering or is likely to suffer significant harm, there should be a strategy discussion involving local authority children’s social care (including the residential or fostering service, if the child is looked after), the police, health, and other bodies such as the referring agency, education, early help, or other practitioners involved in supporting the child. This might take the form of a multi-agency meeting and more than one discussion may be necessary. A strategy discussion can take place following a referral or at any other time, including during the assessment process and when new information is received on an already open case.
The purpose of a strategy discussion is to determine the child’s welfare and plan rapid future action if there is reasonable cause to suspect the child is suffering or is likely to suffer significant harm.
A local authority social worker, health practitioners and a police representative should, as a minimum, be involved in the strategy discussion. Other relevant practitioners will depend on the nature of the individual case but may include those who have concerns about the child and / or those involved in the child’s life, for example:
All attendees should be sufficiently senior to make decisions on behalf of their organisation and agencies. They should be sufficiently skilled and experienced to prepare for and engage with the strategy discussion and be able to critically assess and challenge their own and others’ input.
The discussion should be used to:
It is for the local authority to decide whether to make enquiries and the strategy discussion should inform this decision.
Where there are grounds to initiate an enquiry under section 47 of the Children Act 1989, decisions should be made as to:
The timescale for the assessment to reach a decision on next steps should be based upon the needs of the individual child, consistent with the local protocol and no longer than 45 working days from the point of referral into local authority children’s social care.
The assessment framework should be followed for assessments undertaken under section 47 of the Children Act 1989. The lead practitioner for section 47 enquiries should be a social worker.
Lead practitioners should convene the strategy discussion and make sure they:
Health practitioners should:
The police should:
RELEVANT INFORMATION
Working Together to Safeguard Children, 2025 (Department for Education)
Working Together to Safeguard Children Flowchart 3: Immediate Protection (Department for Education)
RELATED CHAPTERS
Following section 47 enquiries, an initial child protection conference brings together family members (and the child where appropriate), with the supporters, advocates, and practitioners most involved with the child and family, to make decisions about the child’s future safety, health and development. If concerns relate to an unborn child, consideration should be given as to whether to hold a child protection conference prior to the child’s birth.
The purpose of the child protection conference is to bring together and analyse, in a multi-agency and multi-disciplinary meeting, all relevant information and plan how best to safeguard and promote the welfare of the child and protect them from harm. It is the responsibility of the conference to make recommendations on how organisations and agencies work together to safeguard the child in future.
Practitioners and parents should be provided with clear and accurate information about the conference process to support effective planning. All practitioners should approach the work with parents and carers in line with the principles set out in chapter 1 of Working Together to Safeguard Children (Department for Education).
Conference tasks include:
The conference chair:
Lead practitioners should:
All involved practitioners should:
Safeguarding partners should:
The aim of the child protection plan is to:
Local authority children’s social care should:
Lead practitioners should:
The core group should:
For more information see Core Groups procedure.
The review conference procedures for preparation, decision-making and other procedures should be the same as those for an initial child protection conference.
The purpose of a child protection review conference is to review whether the child is continuing to suffer or is likely to suffer significant harm and review developmental progress against child protection plan outcomes. It is to also consider whether the child protection plan should continue or should be changed.
Lead practitioners should:
All involved practitioners should:
A child should no longer be the subject of a child protection plan if:
Lead practitioners should:
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
Children Act 1989: Court Orders and Pre Proceedings (Department for Education)
Pre-Proceedings and Family Justice Hub (Research in Practice)
Once the child protection process has been carried out, it may be deemed by the local authority that there is still not sufficient protection of the child by the parents and that the ‘threshold’ for care proceedings (under section 31 Children Act 1989) has been met in principle.
In this instance, the local authority should determine whether to initiate pre-proceedings and follow the Children Act 1989: Court Orders and Pre Proceedings (Department for Education).
This decision should be informed by engagement with other relevant agencies. During this period, the local authority should offer family group decision-making, such as family group conferences, to continue to explore potential placements within the family network and to clarify the realistic options available for the child. At pre-proceedings, records of key discussions with the family can be used as evidence of decision-making (see Practice Direction 12A – Care Supervision and Other Part 4 Proceedings: Guide to Case Management (Justice Department).
The pre-proceedings process acts as the final opportunity for parents to avoid care proceedings. Whilst pre-proceedings may be initiated at this final stage as per Flowchart 6 What Happens After the Child Protection Conference, Including Review? (opens as a PDF), where the local authority considers the ‘threshold’ for care proceedings to be met, proceedings can be initiated at any stage.
The local authority should work in partnership with families and, where possible, any extra support or services needed to support the family should be identified and put in place. There should be clear expectations set with parents about the changes they are required to make.
See also Children Act 1989: Court Orders and Pre Proceedings (Department for Education)
When initiating pre-proceedings, practitioners should review Practice Direction 12A – Care Supervision and Other Part 4 Proceedings: Guide to Case Management (Justice Department). The pre-proceedings checklist in this Practice Direction outlines the documentation that must be prepared in pre-proceedings or before and submitted as part of the local authority application for a court order.
Practitioners and strategic leads can also refer to the Pre-Proceedings and Family Justice Hub (Research in Practice) for access to resources and tools to support the delivery of best practice in pre-proceedings.
The purpose of this document is to provide practitioners within health, social care and the police with simple guidelines to follow when presented with a child who may need a medical assessment in cases of suspected non-accidental injury, sexual abuse and neglect. It does not apply to children who may need a psychiatric assessment. It has been produced by safeguarding children professionals across the health economy in Buckinghamshire, in consultation with colleagues in Children’s Social Care and the police. The document has been reviewed by the Local Medical Council and the Buckinghamshire Safeguarding Children Partnership.
This guidance details agreed procedures and decision-making pathways to ensure that when a child or young person is alleged or suspected to have suffered significant harm, the child will be medically assessed by a doctor with appropriate skills and expertise following multi-agency agreement/strategy discussion that a medical assessment is appropriate.
When a child has an unexplained or suspicious injury, has symptoms and signs of neglect, or is a suspected victim of child sexual abuse, a medical assessment is usually an essential part of the multi-agency investigation.
The majority of children should be seen during the daytime. Examination of children out of hours is rarely needed other than in cases of acute assault, either for medical or forensic necessity.
Why medical assessment may be needed:
Even when there is multi-agency agreement that a medical assessment is appropriate, consent is sought and the medical is only undertaken with the agreement of the child.
Where the child appears in urgent need of medical attention s/he should be taken to the nearest Accident & Emergency (A&E) department, regardless of age, explanation of injury or any other factor.
A&E staff will contact the on-call paediatric registrar to assess the child if non-accidental injury (NIA), abuse or neglect is suspected. The paediatric registrar will inform the consultant on call.
The paediatrician will refer to Children’s Social Care and the police via telephone on 101 or 999 at the earliest opportunity and then complete the online referral form within 24 hours.
In cases of suspected non-accidental injury, the GP or other health professionals in primary care should:
Except for in cases of child neglect, paediatricians do not accept referrals directly from GPs.
GPs can seek advice from the named doctor during normal working hours from Monday to Friday or from the paediatrician on call out of hours.
Named Doctor: Dr Ash Joshi, 01296 566055 /56
Designated Doctor: Dr Lesley Ray, 07342 064612
Clinical Director Thames Valley Sexual Assault Service (Forensic Doctor): Dr Sheila Paul, 07899 870679
These Buckinghamshire Safeguarding Children Partnership (BSCP) procedures state that medical assessments must be considered when there is a suspicion or allegation of child abuse and/or neglect involving:
Whenever there is reasonable cause to suspect that a child is suffering, or is likely to suffer, significant harm there should be a strategy discussion involving local authority Children’s Social Care, the police, health and other agencies as appropriate.
The strategy discussion will plan the medical assessment, deciding what the objectives of the assessment are, when it needs to take place, who should conduct it and where is the most appropriate venue.
Consideration will be given to the need for any other children in the household to be assessed.
A specific and detailed record must be made of the decision about whether to undertake a medical assessment and its rationale clearly stated.
The strategy discussion must plan what will be explained to parents/carers so that they understand the reason for assessment.
If a criminal prosecution is considered by the police to be a possibility, a statement for court by the paediatrician may be required.
If a criminal investigation is urgent, police action may be taken prior to a full strategy meeting.
The following may give consent to a paediatric assessment:
When a child is looked after under section 20 and a parent has given general consent authorising medical treatment for the child, legal advice must be taken about whether this provides consent for paediatric assessment for child protection purposes (the parent still has full parental responsibility for the child).
A child of any age who has sufficient understanding (generally to be assessed by the doctor with advice from others as required) to make a fully informed decision can provide lawful consent to all or part of a paediatric assessment or emergency treatment.
A young person aged 16 or 17 has an explicit right (s8 Family Law Reform Act 1969) to provide consent to surgical, medical or dental treatment and unless grounds exist for doubting their mental health, no further consent is required.
A child who is of sufficient age and understanding may refuse some or all of the paediatric assessment, though refusal can potentially be overridden by a court.
Wherever possible, the permission of a parent should be sought for children under 16 prior to any paediatric assessment and/or other medical treatment.
Where circumstances do not allow permission to be obtained and the child needs emergency medical treatment, the medical practitioner may:
In non-emergency situations, when parental permission is not obtained, the social worker and manager must consider whether it is in the child’s best interests to seek a court order.
If the child does not require urgent medical care, contact Children’s Social Care First Response Team 01296 383962 / Out of hours 0800 999 7677.
The social worker will contact the on-call consultant paediatrician by ringing the following number and asking the operator for the consultant paediatrician on call:
The consultant will discuss the case with social worker – see above strategy discussion. A suitable time and place for the child to be seen will be arranged. This may not be on the same day as the discussion.
If the child does not require urgent medical care, contact Children’s Social Care First Response Team 01296 383962 / Out of hours 0800 999 7677.
Telephone the community paediatrician on number below and ask to speak to doctor on call for neglect cases:
If the community paediatrician is not available, the social worker’s contact details will be taken and the doctor will return the call within 4 hours or before 5pm, whichever is sooner.
Following a strategy discussion with the social worker, the paediatrician will decide when and where the medical is to take place. These medicals are not urgent but should take place within a timely manner ideally before the initial case conference and definitely before the first review conference. Younger children may need to be seen more quickly.
The appointment for the medical should be sent to the parents/carers, social worker and school nurse/health visitor as appropriate. In cases of neglect all children in the family may be seen for medical assessment.
Local policy with regard to examination in cases of suspected sexual abuse is underpinned by the Guidelines on Paediatric Forensic Examination in relation to Possible Child Sexual Abuse produced by the Royal College of Paediatrics and Child Health (RCPCH), and the Faculty of Forensic and Legal Medicine (FFLM).
The Thames Valley Sexual Assault Referral Centre (SARC) is run by Harmoni for Health and has been named ‘Solace’.
The contact number for Solace is 0300 1303036.
In all cases, medical needs are paramount and come before forensic needs if necessary. If the child requires urgent medical treatment they should be taken to the nearest A&E department.
If the child does not require urgent medical care, contact Children’s Social Care First Response Team 01296 383962 / Out of hours 0800 999 7677.
The timing of the medical depends on the time of the sexual assault (acute or historic) and the pubertal status of the child.
If an urgent forensic medical examination is required, the police should contact Solace who will arrange an appointment with the duty forensic doctor on the SARC rota. If that doctor does not have all the core and case dependent skills required to examine the child, the forensic medical examination should ideally be carried out by a forensic doctor experienced in paediatric examination or, if not available, jointly by the duty forensic doctor and a consultant paediatrician on call.
Professionals can call Solace directly for advice on any sexual assault case regardless of age on 0300 130 3036. They should also contact police/social care as per the flow chart (Appendix A).
Cases of acute sexual assault in pre-pubertal children (aged usually less than 12 years) are rare. These cases require an urgent forensic examination as soon as practicable so that forensic evidence is not lost. Persistence data reveal the opportunity of up to three days to collect samples for foreign DNA from a pre-pubertal child, depending on the type of sexual assault. Research shows this is often reduced to 13 hours in practice.
Cases of acute sexual assault, within the last 7–10 days, in post-pubertal children (usually aged more than 12 years) need an urgent forensic medical examination. The timing of a medical examination needs to balance the welfare of the child with the need to secure forensic evidence. More evidence is likely to be secured the sooner a medical examination takes place, but in achieving this effort should be made to minimise the distress to child. The timing depends on the disclosure but always as soon as possible and usually the same day or night, so that forensic evidence is not lost and distress is minimised. The examination should be carried out by the duty forensic doctor on the SARC rota and should be arranged through the police.
It is important to recognise that urgent examinations to capture forensic evidence such as healing injuries, or provide appropriate treatment such as emergency contraception, may be needed outside the persistent data time scales and this is reflected in the FFLM and the RCPCH service specification for the clinical evaluation of children and young people who may have been sexually abused. In this document it is emphasised that acute examinations may be needed for the above reasons up to 21 days post-alleged event.
Pre-pubertal (children aged usually less than 12 years) and post-pubertal (usually aged more than 12 years) cases where there is delay in reporting sexual abuse (abuse occurred usually more than 21 days) are non- acute cases that do not need an urgent out of hours examination. Police should make arrangements with the forensic doctor.
If you have concerns about medical examinations the named and designated doctors are available for advice and contact details are given below:
Appendix A Flow Charts (opens as a PDF)
Appendix B – Body Map (opens in Word)
Loss and bereavement are an inevitable part of our lifecycle. During childhood and adolescence some children will experience the death of someone they know. By the age of 16, it is estimated that 4.7% or around 1 in 20 young people will have experienced the death of one or both of their parents. Most will be supported by family and friends, so that their grief takes place within a nurturing framework, promoting healthy development into adult life.
Some children have particular needs which arise as a result of bereavement. For example, some children may enter the ‘Looked After’ system because they have lost a parent; some are bullied because of their bereavement; and some families may face financial difficulty and may experience housing or other problems as a consequence of such a loss. In these cases, a coordinated multi-agency response is required to deal sensitively and effectively with each particular situation.
Lessons from Child Safeguarding Practice Reviews in Buckinghamshire have highlighted the need for us all to take the bereavement of young people seriously and consider, in particular, the additional risks that grief can introduce to those already in vulnerable circumstances. This finding mirrors research that found those who experience multiple bereavements, or bereavement alongside other difficulties, are statistically ‘at risk’ of experiencing negative outcomes in areas such as education, depression, self-esteem and risk-taking behaviour later in life.
This guidance is to help staff recognise and respond appropriately when a young person is grieving.
The more ongoing proactive support that is given across a whole community, the more likely children, young people and their community will show good resilience to the impact of events involving loss and bereavement, and will not require longer-term additional specialist support. Appropriate support is therefore best provided proactively in anticipation of events, and also as an immediate and longer-term response to events.
Some guidance on responding to bereavement is provided below. A list of national organisations that can provide support is also provided at Appendix A.
Where bereavement for a child or young person is known or anticipated, consider:
If the answer to these questions is yes:
If the answer is no, consider the options outlined below.
A child/young person will have additional or more complex needs in the following circumstances:
Where the needs are more complex, as listed above, or in situations where the family are unable (perhaps due to their own grief) or unavailable (due to physical absence), advice can be sought from the CAMHS Single Point of Access.
In addition to the complex needs listed at Section 2.2, some deaths are likely to present much deeper trauma for the child and family, e.g. murder, multiple family deaths from accidents, deaths witnessed by child/young child or major incidents.
In such cases, specialist trauma and bereavement services should be sought from the CAMHS Single Point of Access.
Adults can play a vital role in preparing themselves and the young people they work with in the following ways:
Children and young people of all ages who have experienced a death have said that they prefer to be supported by known adults and older peers rather than someone who is unfamiliar. Professionals can be effective by working together with the child’s parents, carers, school staff, etc to help them support the child rather than directly with the child themselves. However, it can sometimes be helpful for children to talk to someone out of the family who is not affected by the sadness.
It may be helpful to go through the following information with adults or older peers who are helping a bereaved child – to help raise their confidence that they have the skills to do this:
There are some reactions which start to cause concern, for example because they continue for some time and appear to be increasing rather than diminishing. These need to be acted upon and the help of specialist services may need to be considered. Professionals should follow the usual procedures where they have a safeguarding concern (see Referrals chapter).
The following (non-exhaustive) list of warning signs should be taken together with an assessment of what else is happening in the child’s life:
A number of factors are known to make young people’s bereavement more difficult. These include having an ambivalent relationship with the person who has died and having little support available.
Following a traumatic bereavement such as suicide or murder, young people can develop a variety of traumatic stress reactions which may inhibit their grief.
There is increasing evidence that bereavement in circumstances that are already disadvantaged, can increase young people’s vulnerability to mental and emotional health difficulties, self-harm and risky health behaviours.
Vulnerable young people are over-represented among children in care (Children Looked After). The Childhood Bereavement Network (CBN) in a UK study cited drug and alcohol misuse and other risk-taking behaviour, poor general health, severe emotional and mental health problems, domestic violence and involvement in crime, as contributing factors to higher mortality rates – and greater proportions of sudden and traumatic deaths among the birth families and friends of Children Looked After. Some of these factors are similar to those that could have led to a child or young person becoming looked after in the first place.
In addition, some children and young people come into care because of the death of a parent and absence of other family members to look after them. This highlights the importance of planning for the care of children and young people who experience the death of a lone parent/carer.
The CBN study described children and young people’s feelings, such as aggression, being withdrawn, self-harming, suicide, eating disorders, incontinence, vomiting clinginess, poor memory and, in some cases, symptoms of post-traumatic stress disorder.
Children in care experience a variety of separations and losses in their lives. These losses can make the impact of the death of someone close to them more acute.
Problems with contact can mean that a child doesn’t have time to prepare for a death, even when others are expecting it.
In addition to the issues faced by Children Looked After, a secure setting can bring additional challenges that affect their experience and ability to access support for bereavement, including:
Many of these losses thwart the coping strategies and emotional reliance that children and young people might otherwise use to get comfort and reassurance at times of great stress, such as when someone close dies.
Children and young people in secure accommodation are likely to be placed some way from home, making it more difficult for them to be involved in any family remembrances and funeral arrangements.
“My Gran died five months ago. I was not allowed to go to the funeral even though it meant so much to me to say goodbye… I should have been allowed to go to the funeral. I will never get my chance to say goodbye now, and I am really angry about that”. Young woman in a medium secure psychiatric unit. CBN study.
Following a traumatic experience, such as witnessing an accident, or even the murder of one parent by another, children and young people may develop a variety of stress reactions. These can include intrusive thoughts about what has happened, flashbacks, separation difficulties, problems concentrating, difficulties in talking with parents, carers and friends, and heightened fears and anxiety about safety. Studies suggest that children and young people who are bereaved through the murder or suicide of a parent are at greater risk of depression and post-traumatic stress disorder.
Asylum-seeking young people are also likely to have experienced multiple losses, including separation from family and often the death of someone close to them, which they may also have witnessed.
Language and cultural difference can make it difficult for young people to talk about their fear and anxieties that they may feel in their new and often uncertain circumstances. It is not uncommon for these young people to experience symptoms of post-traumatic stress disorder.
In some cultures, mental health difficulties are understood and dealt with differently, so some young people may not be interested in a referral for counselling or other support. This does not mean that their bereavement needs should not be assessed in the same way, but the response should be even more sensitive to their background and understanding, which may differ from Western perspectives.
The emotional and practical needs of asylum-seeking young people may be overwhelmed by the need to get used to their new life. Great care should be taken to ensure that bereavement, amongst all these other stresses, is identified and given sufficient attention.
For children and young people with learning disabilities there may be additional considerations related to the disability itself and the attitudes of others towards their disability. This has been described as the ‘double taboo’ of death and disability (M Oswin, Am I Allowed to Cry? Study of Bereavement Amongst People Who Have Learning Difficulties, 1991). People with learning disabilities are often protected from the true impact of death, by well-meaning carers who want to minimise their distress.
Over-protective attitudes may not help bereaved children/young people to accommodate their grief, e.g. if they are not encouraged to say goodbye to their loved one, not invited to attend the funeral, or in some cases not even told about the death when it occurs.
Like all children and young people, those with learning difficulties do not need protection from the feelings and emotions associated with grief, but support and help to express them, and reassurance that these sometimes powerful and overwhelming emotions are normal and necessary.
Bereavement affects people in different ways, and familiar carers might offer a strong sense of social support, while also having a pivotal role in anticipating identifying and acknowledging individual response and the need for additional specialist input. Support at this time is crucial, both to bereaved people and those responsible for their care. Service providers need to be mindful of the importance of support at such times, and that such support may be needed in the short and long term.
By identifying, acknowledging and addressing such challenges in an open, honest and sensitive way, carers can help the child/young person with a learning disability to confront and deal with the sadness and other associated feelings following the death of a loved one.
When death and bereavement is dealt with in a supportive, sensitive and consistent way, all children/young people may learn to develop personal coping strategies and learn to cope with future losses in a more constructive manner. Meaningful support is crucial to this process.
Children with learning difficulties may find the concept of death and its permanence particularly difficult to grasp and will benefit from simple, practical examples to illustrate the difference between dead and living things.
However, visiting a graveyard can be especially confusing for children with learning difficulties due to the lack of visual evidence as to exactly where the dead body has gone.
Children with learning difficulties may have less vocabulary and tend to express their feelings even more through behaviour rather than words.
In working with bereaved children/young people, opportunities for helping to capture memories that are meaningful for them should always be considered. For Looked After Children, obtaining a thorough ‘life story’ for the child will be a priority piece of work within the care plan itself, but all children/young people can benefit from someone helping them to capture objects or moments in their history.
Cultural and religious customs, particularly around death, should be taken into consideration. Workers should seek advice where needed and take care not to impose their own customs.
Where death is anticipated, the child can be helped to identify and communicate things they may want to say to, or do with, the person they are going to lose. This may include having some pictures taken together and/or a film; writing them a letter or poem; giving each other a lock of hair. In conversations or other communications, the child might want to think about any questions they want answered.
If the death was unexpected, staff may need to give consideration to who else in the family or community might be able to supply the child with relevant information and objects.
Thought should be given to whether it is appropriate and helpful for a child to be given the opportunity to see the deceased person before burial or cremation. This is an area where there can be well-meaning, but considerable debate, particularly among family members. The child/young person’s wishes should be sought and communicated to those making arrangements. Like adults, some children may want to remember the lost person as they were, whereas others will find that seeing the deceased person assists them in accepting the reality of their loss.
The child could be asked whether they wish to have a relevant piece of jewellery, clothing, lock of hair etc following the death.
Regarding attendance at funerals, staff should respect the wishes of the family concerned, but keep in focus the support and involvement that the child or young person might need. This might mean speaking on behalf of the child/ young person when they wish to be involved in attending, or making arrangements for, the funeral.
If they are attending the funeral, the child might benefit from being accompanied by a member of staff, particularly if the family are absorbed by their own grief. Such arrangements will need to be discussed sensitively with those arranging the funeral.
Talking to a child or family about the death of someone close may be hard for staff to do. Supporting a child experiencing loss or bereavement can be exhausting and possibly bring back painful memories. Staff should talk to other team members and their line manager if they need support.
If a staff member has suffered a recent bereavement themselves, it is advisable for them and for the bereaved child/young person that they discuss the appropriateness of this piece of work with their line manager. If they are already working with the child/young person, a sudden retreat might of course reinforce their feelings of loss. Support from someone to work alongside them for certain tasks might prove a better solution.
Employers have a duty of care to their staff. The provision of training can enable staff to operate in this highly sensitive area and ensure quality of care for those who are bereaved. The provision of support for staff who may be adversely effected by their exposure to traumatic deaths, and to grief which may be emotionally draining, will be essential to enable them to continue to function effectively.
Staff members may carry their own grief and bereavements, which may influence how they react to any related circumstance. It is essential therefore that support/supervision takes into account the past experience of the individual and recognises the need for self-awareness and reflection on their history. Support/supervision should take this into account and help staff to recognise the need for self-awareness and reflection.
Training and guidance for staff should include identified core elements:
High-risk cases should be identified and prioritised for regular support/supervision.
Support for staff should be provided by creating a culture of ‘checking out’ that staff are coping. Where possible, sensitivity should be shown to staff by not exposing them to very stressful deaths within work too soon following a personal bereavement.
A supportive culture needs to be created within each organisation to facilitate staff coping with bereavement especially in traumatic situation.
Internal provision of support by the organisation is encouraged, but staff should also have the opportunity to access employee counselling services where necessary, or preferred.
A resource list of where to access support should be available for managers and staff.
| Name | Contact Information | Details |
| Buckinghamshire Educational Psychology Team | Email: [email protected]
Telephone: 01296 382135 |
Educational psychologists can offer training to school staff on how to support grieving students. This includes understanding children’s reactions to bereavement and effective strategies to help them cope. In cases where the bereavement affects the entire school community, such as the death of a student or staff member, educational psychologists can help manage the situation. They can provide guidance on how to communicate the news, support affected individuals, and maintain a sense of normalcy. |
| National Child Death Helpline | www.childdeathhelpline.org.uk/
0800 282 986 |
Freephone service to anyone affected by the death of a child of any age – whether they are parents, grandparents, siblings, family members, friends or involved professionals. All volunteers are bereaved parents. |
| CRUSE Bereavement Support | Home – Cruse Bereavement Support
0808 808 1677 |
Offers support, advice and information to children, young people and adults when someone dies. |
| Child Bereavement Uk | https://www.childbereavementuk.org/
0800 02 888 40 |
Supports families and educates professionals when a baby or child of any age dies or is dying, or when a child is facing bereavement. |
| Winston’s Wish | https://winstonswish.org/
08088 020 021
|
Winston’s Wish is a charity that helps children, teenagers and young adults (up to the age of 25) find their feet when their worlds are turned upside down by grief. |
| Childhood Bereavement Network | https://childhoodbereavementnetwork.org.uk/
|
Seeks to ensure that all children and young people, together with their families and other caregivers, including professional carers, can easily access a choice of high-quality local and national information, guidance and support. |
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
Any assessment of children in secure youth establishments should take account of their specific needs. In all cases, the responsibility for the welfare and safety of a child is located jointly with the home and host local authority. Any professional conduct issues should be dealt with by the local authority in which the establishment is located. Partners should work with the secure youth establishment and, where appropriate, the Youth Custody Service to ensure that the child has a single, comprehensive support plan.
Where a child becomes looked after, as a result of being remanded to youth detention accommodation (YDA), the local authority should visit the child and assess the child’s needs before taking a decision on how they should be supported. This information should be used to prepare the care plan, which should set out how the YDA and other practitioners will meet the child’s needs whilst the child remains remanded, and at any point of transition they will experience (either returning to the community or upon receiving a custodial sentence). The care plan must be reviewed in the same way as a care plan for any other looked after child.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
A crucial role of children’s social care is to provide help and support to children with disabilities and their families. When undertaking an assessment of a child with disabilities, practitioners should recognise the additional pressures caring for a child with disabilities can place on the family, and the distinct challenges they may have had to negotiate as a result of their child’s disability.
The assessment process should focus on the needs of the child and family, be strengths-based, and gather information to inform decisions on the help needed to:
The local authority must also consider whether it is necessary to provide support under section 2 of the Chronically Sick and Disabled Persons Act 1970. Where a local authority is satisfied that the identified services and assistance can be provided under section 2 of the Act, and it is necessary in order to meet the needs of a child with disabilities, it must arrange to provide that support.
Where a local authority is assessing the needs of a child with disabilities, a carer of that child may also require the local authority to undertake an assessment of their ability to provide, or to continue to provide, care for the child, under section 1 of the Carers (Recognition and Services) Act 1995. The local authority must take account of the results of any such assessment when deciding whether to provide services to the child.
If a local authority considers that a parent carer of a child with disabilities may have support needs, it must carry out an assessment under section 17ZD of the Children Act 1989. The local authority must also carry out such an assessment if a parent carer requests one. Such an assessment must consider whether it is appropriate for the parent carer to provide, or continue to provide, care for the child. The assessment should also take account of parent carer’s needs and wishes, and the specific needs and circumstances of the child resulting from their disability. Parent carers have the right to request an assessment under section 17ZD of the Children Act 1989, including where a child is not otherwise known to children’s social care. Local authorities must ensure they have a process to facilitate these assessments if requested.
In line with the commitments made in the Special Educational Needs and Alternative Provision Improvement Plan, local authorities are encouraged to implement the role of Designated Social Care Officer (DSCO) in each local area. The DSCO role is intended to provide the capacity and expertise to improve the links between social care services and the SEND system. Similar to the Designated Clinical Officer (DCO) or Designated Medical Officer (DMO) role in health, the DSCO role will support both operational input (such as the contributions from care to education, health and care assessments) and more strategic planning functions (such as the commissioning of care services such as short breaks) for children with special educational needs and disabilities.
RELEVANT GUIDANCE
Modern Slavery: statutory guidance for England and Wales (Home Office)
Safeguarding children who may have been trafficked (Department for Education and Home Office)
This chapter should be read in conjunction with the following government guidance: Care of unaccompanied migrant children and child victims of modern slavery: statutory guidance for local authorities (Department for Education) which sets out the steps which local authorities should take to plan for the provision of support for Looked After Children / Children in Care who are unaccompanied asylum seeking children, unaccompanied migrant children or child victims of modern slavery including trafficking. Elements of the guidance will also be relevant for the care of Looked After Children who are UK nationals and who may also be child victims of modern slavery.
The cohort of unaccompanied migrant children and child victims of modern slavery includes a wide range of children in a variety of circumstances that a local authority will need to be aware of in order to ensure that the child receives appropriate legal advice and support. Some will have been trafficked or persecuted and may have witnessed, or been subject to, horrific acts of violence. Other migrant children may have been sent to the UK in search of a better life, or may have been brought here for a private fostering arrangement and subsequently exploited or abandoned when the arrangement fails.
There are a wide range of status possibilities for migrant children that the local authority will need to be aware of. In brief, the following categories regarding status are the most likely to be encountered. However this list is not exhaustive and legal advice should be sought wherever there is uncertainty about a migrant child’s status.
Categories of unaccompanied children include:
Where it is established that a referral concerns a young unaccompanied child migrant, regardless of the category, this will always satisfy the criteria for services as a Child in Need.
An unaccompanied child will become a Looked After Child, after they have accommodated by the local authority under Section 20(1) of the Children Act 1989 for 24 hours. Once accommodated, they will be subject to the appropriate regulations and the same provision as any other Looked After Child.
The local authority should record any modern slavery concerns on the child’s care plan.
As part of the general duty to assess and meet the needs of an Unaccompanied Asylum Seeking Child, the local authority should ensure that the child has access to a legal representative.
Unaccompanied children are highly likely to require specialist support from a variety of organisations and agencies (see for example, the Independent Unaccompanied Asylum-Seeking Children Support Service (IUSS) provided by the Refugee Council).
All professionals involved in the care of unaccompanied children and child victims of modern slavery should be able to recognise indicators of trafficking, slavery, servitude and forced or compulsory labour and should have an understanding of the particular issues likely to be faced by these children.
This is a highly complex area of work, and professionals will need to have available to them a solid understanding of the asylum process or colleagues or other professionals with such expertise.
The kinds of issues that may need to be negotiated include:
For more information, see Processing children’s asylum claims (UK Visas and Immigration).
Social workers should also have a broad understanding of the immigration system – for example, the immigration application process, different types of leave, making further leave to remain applications and the appeals process. Social workers should also have an understanding of the trafficking referral process and the wider safeguarding system around child victims of modern slavery, including how and when to refer a child to the National Referral Mechanism (NRM).
Legal advice can only be provided by a registered immigration advisor, ideally one with expertise in working with children. Legal Aid is available for asylum cases and Looked After Children will generally be eligible.
Independent Reviewing Officers (IRO) should consider the child’s needs as an unaccompanied child or child victim of modern slavery, including trafficking, when planning and providing care. They should also have an awareness of the particular needs and issues children may face as a result of being an unaccompanied child or child victim of modern slavery so that they can provide appropriate challenge at review.
Service providers should ensure that foster carers and all other care staff in placement settings are aware of appropriate steps to reduce the risk of trafficked children returning to their traffickers.
Social workers should consider all unaccompanied migrant children as potential victims of modern slavery in the first instance until this possibility is either confirmed or discounted and they should also have an understanding of the trafficking referral process under the National Referral Mechanism.
The social worker must ensure that all unaccompanied children have access to specialist asylum and/or immigration legal advice and representation in their assessment so as to ensure the child can fully present their case for asylum or leave to remain.
The assessment will take account of:
Unaccompanied migrant children and child victims of modern slavery will need access to specialist legal advice and support. This will be in relation to immigration and asylum applications, and decisions and any associated legal proceedings. If they have been a victim of modern slavery, they will also need support in relation to criminal proceedings or compensation claims. The assessment should note that specialist legal support is required and how it will be provided. The child’s social worker should ensure that they are accompanied in all meetings, including meetings with legal professionals. The person accompanying the child does not have to be the child’s social worker.
In determining an unaccompanied young person’s accommodation needs, the assessment must have regard to their age and independent living skills and consider the intensity of service required. This may range between independent accommodation, semi-independent accommodation foster or residential placements, or in specific cases, a specialist residential therapeutic unit.
No assumptions should be made about the child’s language skills. An appropriately qualified and vetted interpreter must be used to assist in all assessments (see Interpreting, Signing and Communication Needs).
When completing cases records, it is important to pay particular attention to the detail of spelling names and of descriptions of family relationships.
Planning for the child should include planning for a variety of possible outcomes regarding the child’s immigration status – see Section 10, Asylum Process – Possible Outcomes.
Where the age of the child is uncertain and there are reasons to believe they are a child, they will be presumed to be a child in order to receive immediate assistance, support and protection in accordance with Section 51 Modern Slavery Act 2015. Assessments must be undertaken in accordance with standards established in case law and should only be carried out where there is reason to doubt that the child is the age they claim. For further guidance see: Age Assessment Guidance published by ADCS. In all cases where a referral is received concerning an unaccompanied child, the relevant Team will carry out an assessment in accordance with the Assessment Procedure, to determine whether they are a Child in Need.
Young unaccompanied child migrants should be provided with information about the services available to them from the local authority and other agencies.
The young person will also be given assistance to register with a GP and dentist, and enrol in a local school or college. The health professionals and the school should be aware of the child’s status and senior managers such as the Virtual School Head should be informed of the school placement. There will be a need to set out clearly any particular implications of the child’s status for non-specialist professionals such as GPs and teachers, including any urgency of involvement – particularly with health practitioners. An interpreter should be booked to accompany the young person to appointments with the GP or school, where necessary.
Where a young person’s needs are for independent or semi-independent accommodation, and the manager agrees, assistance should be given with completion of the necessary Housing Application.
Where the assessment identifies that an unaccompanied young child migrant needs to be Looked After, all the procedures in relation to Care Plans, Health Care Plans, Personal Education Plans and Placement Plans must be completed (see Decision to Look After, Buckinghamshire Children’s Social Care Procedures).
For unaccompanied migrant children who are Looked After, the placement decision will also need to be informed by careful consideration of the wider support needs of the child, including their cultural and social needs. It may be that the accommodation setting or carers cannot meet those needs on their own so other more creative ways, such as mentors or links to diaspora groups, could be used. As with all Looked After Children, an unaccompanied child’s ethnicity, cultural and linguistic background should be taken into account when placing the child with foster carers. However, these are not overriding considerations and should be taken into account alongside all of the child’s needs. Nevertheless, the placement should meet the child’s needs as a whole and be consistent with their wishes and feelings.
Where there are safeguarding concerns relating to the care and welfare of any unaccompanied child, including where modern slavery is suspected or has been identified, these should be investigated in line with the statutory provisions contained in Working Together to Safeguard Children. The opportunity to intervene to prevent any further exploitation might be very narrow, so the entry local authority should convene a Strategy Meeting/Discussion as soon as possible and take any necessary immediate action to safeguard and promote the child’s welfare. This Strategy Meeting/Discussion should involve the police, Immigration officials and any other relevant agencies and plan rapid further action if concerns are substantiated.
Provision may need to be made for the child to be in a safe place before any further assessment takes place and for the possibility that they may not be able to disclose full information about their circumstances immediately. The location of the child should not be divulged to any enquirers until their identity and relationship with the child have been established and the local authority is assured of their motives, if necessary, with the help of police and Immigration officials. The installation of police installed alarms should be considered and the child or young person advised about the safe use of mobile phones, so they cannot be traced etc.
All unaccompanied young asylum-seekers who are eligible for a service will be entitled to financial assistance which must first be authorised by the manager. The social worker should arrange for payment of the relevant amounts in accordance with the local authority procedures.
Travel cards or warrants will be issued to young unaccompanied asylum-seekers in relation to appointments at the Home Office.
Where an assessment identifies that an unaccompanied child migrant does not meet the criteria for a service from Children’s Social care but appears to be in need of services from elsewhere, the social worker will refer the young person to the appropriate agency which may be a different local authority Children’s Social Care department, the Refugee Council, UK Visas and Immigration and/or an appropriate voluntary agency.
In such circumstances, the duty social worker should make an appointment for the young person and advise them of the name, address (including a map where necessary) and contact number of the person with whom the appointment has been made. In addition, the duty worker must send a copy of the referral and assessment to the relevant office.
In all cases where a service is to be refused, the social worker must consult their manager before the decision is made and the letter confirming the decision is sent. Any correspondence received in relation to the decision should be referred to the manager.
The provision of a service is dependent on the young person continuing to qualify for the service.
Services to an unaccompanied child migrant may be withdrawn, for example, where another adult wishes to assume Parental Responsibility and this is assessed as appropriate.
The service must not be withdrawn without a Child in Need Plan Review (see Child in Need Plans and Reviews Procedure, Buckinghamshire Children’s Services) and the agreement of the social worker’s manager. Any such decision must be clearly recorded, with reasons. In all such cases, legal advice should usually be obtained before a final decision is made.
Where a service is withdrawn, the social worker should inform the Finance Office, if appropriate, immediately.
Planning transition to adulthood for unaccompanied children is a particularly complex process that needs to address their developing care needs in the context of their immigration status.
Pathway Planning to support an unaccompanied child’s transition to adulthood must cover the areas that would be addressed within any care leaver’s plan as well as any additional needs arising from their immigration status and the action required to resolve this. (See Leaving Care and Transition Procedure, Buckinghamshire Children’s Services.)
Former unaccompanied children who qualify as care leavers and who have been granted leave to remain, or who have an outstanding asylum or other human rights claim or appeal, are entitled to the same level of care and support from the local authority as any other care leaver.
The extent of any care leaver duties on local authorities to provide support to former unaccompanied children who have turned 18, exhausted their appeal rights, established no lawful basis to remain in the UK and should return to their home country is subject to a Human Rights Assessment by the local authority. This is set out under the restrictions on local authority support for adults without immigration status.
For former unaccompanied children whose long-term future is in the UK, transition planning will need to consider the challenges and issues facing any care leaver, such as education or preparing for independent living. Planning for children and young adults who have been granted refugee status or humanitarian protection should also consider when they may be required to make a further application for leave to remain.
Where an unaccompanied child or child victim of modern slavery qualifies for local authority care leaving support, a personal adviser must be appointed to support them.
Pathway plans should always consider and reflect the implications for the child or young adult if their asylum claim is refused without a grant of leave, if their application to extend their leave is refused or if their appeal against a refusal is dismissed. In such circumstances, the person will become unlawfully present in the UK and be expected to make plans for a return to their home country. A plan for a return to their home country may also need to be made at any other point, should the care leaver decide to leave the UK.
Planning may have to be based around short-term achievable goals whilst entitlement to remain in the UK is being determined. For the majority of unaccompanied children who do not have permanent immigration status, transition planning should initially take a dual or triple planning perspective, which, over time should be refined as the young person’s immigration status is resolved.
Planning cannot pre-empt the outcome of any immigration decision and may be based on:
Assistance should be given in advance of their 18th birthday with the necessary applications for housing, Housing Benefit and any other relevant benefits. The social worker must ensure that the young person has accommodation to which to move on their 18th birthday. The provider of the young person’s present accommodation and the Finance Office should be informed when the accommodation arrangement will end.
Financial support for care leavers who are former unaccompanied child migrants should reflect their needs and their immigration status. Financial policies should highlight any entitlements and how their immigration status may affect these. Pathway plans should address employment opportunities and funding arrangements for education and training, taking account of the young person’s immigration status.
If a young person has No Recourse to Public Funds (NRPF), they will be unable to access a number of welfare benefits and social housing. Subject to the Human Rights Assessment by the Local Authority under Schedule 3 Nationality, Immigration and Asylum Act 2002 (as amended), the provision of accommodation may form part of the Leaving Care support provided to a young person who has NRPF. For further information please go to Families with No Recourse to Public Funds Procedure, Buckinghamshire Children’s Services.
Having NRPF does not prevent a person from accessing other publicly funded services, but many of these will have eligibility criteria based on immigration status which will need to be considered. (See NRPF Network – What are public funds?)
Where a young person is Looked After, their circumstances will be reviewed in accordance with the Looked After Reviews Procedure.
Any other services provided should be reviewed at least every 6 months as set out in the Child in Need Plans and Reviews Procedure.
In advance of each review, the social worker will send the young person a checklist setting out the documents which are required to be produced at the Review, such as confirmation of registration with a GP, enrolment at schools/college and updated information concerning their asylum status.
The young person should be invited to the Review and an interpreter should be booked as necessary.
Independent Reviewing Officers (IRO) should have regard to the child’s needs as an unaccompanied child or child victim of modern slavery, including trafficking, when planning and providing care. They should also have an awareness of the particular needs and issues children may face as a result of being an unaccompanied child or child victim of modern slavery so that they can provide appropriate challenge at review. Service providers should ensure that foster carers and all other care staff in placement settings are aware of appropriate steps to reduce the risk of trafficked children returning to their traffickers.
Guidance for cases where the child has been the subject of sexual exploitation can be found in the Multi Agency Child Exploitation Protocol.
Where a Review confirms the service, the Financial Assessment Form should be updated. Where additional support services are identified as necessary, the Plan should be updated to reflect this.
Where services are withdrawn as a result of the Review, the relevant teams should be notified immediately.
There are four main possible outcomes of the asylum process for an unaccompanied child, which will determine what the long term solution might be:
Granted refugee status (i.e. granted asylum), with limited leave to remain for five years, after which time they can normally apply for settlement (i.e. indefinite leave to remain);
Refused asylum but granted humanitarian protection, with limited leave to remain for five years, after which time they can normally apply for settlement (i.e. indefinite leave to remain). This is most commonly granted where the person is at risk of a form of ‘ill treatment’ in their country of origin but which does not meet the criteria of the Refugee Convention. As it is very likely that those granted refugee status or humanitarian protection will qualify for indefinite leave to remain, their care and pathway planning should primarily focus on their long-term future in the UK, in the same way as for any other Care Leaver;
Refused asylum but granted Unaccompanied Asylum Seeking Child (UASC) Leave. This is normally for 30 months or until the age of 17½, whichever is the shorter period. This form of leave is granted to unaccompanied children where they do not qualify for refugee status or humanitarian protection, but where the Home Office cannot return them to their home country because it is not satisfied that safe and adequate reception arrangements are in place in that country. It is a form of temporary leave to remain and is not a route to settlement. It is important to note that this decision is a refusal of the child’s asylum claim and will attract a right of appeal. The child should be assisted to obtain legal advice on appealing against such a refusal. Before the child’s UASC Leave expires, they can submit an application for further leave to remain and/or a fresh claim for asylum, which will be considered. It is essential that they are assisted to access legal advice and make any such further application or claim before their UASC Leave expires. In such cases, care and pathway planning should therefore consider the possibility that the child may have to return to their home country once their UASC Leave expires or that they may become legally resident in the UK long-term (if a subsequent application or appeal is successful). Planning should also cover the possibility that they reach the age of 18 with an outstanding application or appeal and are entitled to remain in the UK until its outcome is known;
Refused asylum and granted no leave to remain. In this case the unaccompanied child is expected to return to their home country and their care plan should address the relevant actions and the support required. The Home Office will not return an unaccompanied child to their home country unless it is satisfied that safe and adequate reception arrangements are in place in that country. Any appeal or further application should be submitted where appropriate by the child’s legal adviser.
Although the above are the four main types of outcomes for an unaccompanied child, there may be others. For example, a child may be granted discretionary leave depending on whether they meet other criteria such as needing to stay in the UK to help police with their enquires after being conclusively identified as a victim of trafficking. Other examples include: leave as a stateless person; limited or discretionary leave for compassionate reasons; and limited leave on the basis of family or private life.
Local Government Association – Council Support: Refugees, Asylum Seekers and Unaccompanied Children – resource for council staff, designed to answer questions about supporting refugees, asylum seekers and unaccompanied children.
National Referral Mechanism: Guidance for Child First Responders – provides details on how to refer a child into the NRM and complete the referral form, reviews of decisions and the benefits of referral.
Guidance on Processing Children’s Asylum Claims – Case worker guidance – sets out the process which immigration officials follow in determining an asylum claim from a child and the possible outcomes for the child
Modern Slavery and Exploitation Helpline (Unseen)
National Transfer Protocol for Unaccompanied Asylum Seeking Children – interim national transfer procedure and transfer flow chart for the safe transfer of UASC from one UK Local Authority to another.
Child Protection: Working with Foreign Authorities (Department for Education) – guidance on child protection cases and care orders where the child has links to a foreign country
Modern Slavery: How to identify and support victims (Home Office)
RELEVANT CHAPTERS
Unaccompanied Asylum Seeking Children
Multi-Agency Child Exploitation Protocol
RELATED GUIDANCE
Evidence from research demonstrates that a significant proportion of children who go missing are at risk of serious harm. There are links between going missing and a number of different risk factors. For example, there are particular concerns about the links between children going missing and the risks of exploitation (criminal and sexual), especially for looked after children (LAC) who go missing from their placements. Other risks and vulnerabilities include, but are not limited to, trafficking, forced marriage, radicalisation and involvement in gangs.
This guidance is relevant for all agencies working in Buckinghamshire in cases where children go missing from either home, care or education. It is designed to ensure that when a child goes missing there is an effective and coordinated safeguarding response from all agencies involved. In particular:
This guidance should be read in conjunction with the Statutory guidance on children who run away or go missing from home or care (Department for Education).
The following safeguarding principles should be adhered to in relation to identifying and locating children who go missing:
All practitioners working with children at risk of going missing should discuss the dangers relating to this with the child and, if appropriate, their family. They should be told about support services and this should include information about helplines.
Anyone whose whereabouts cannot be established will be considered as missing until located and their well-being or otherwise confirmed.
All reports of missing people sit within a continuum of risk from ‘no apparent risk (absent)’ through to high-risk cases that require immediate, intensive action.
| No apparent risk (absent) | |
| There is no apparent risk of harm to either the subject or the public. | Actions to locate the subject and/or gather further information should be agreed with the informant and a latest review time set to reassess the risk. |
| Low risk | |
| The risk of harm to the subject or the public is assessed as possible but minimal. | Proportionate enquiries should be carried out to ensure that the individual has not come to harm. |
| Medium risk | |
| The risk of harm to the subject or the public is assessed as likely but not serious. | This category requires an active and measured response by the police and other agencies in order to trace the missing person and support the person reporting. |
| High risk | |
| The risk of serious harm to the subject or the public is assessed as very likely. | This category almost always requires the immediate deployment of police resources – action may be delayed in exceptional circumstances, such as searching water or forested areas during hours of darkness.
There should be a press/media strategy and/or close contact with outside agencies. Although please note that caution must be exercised when making decisions on whether to use media appeals, as sometimes children who are the victims of exploitation may be at increased risk in relation to gang involvement. Children’s services must also be notified immediately if the person is under 18. |
Thames Valley Police will not categorise the following as ‘no apparent risk’; they will always be the subject of a missing person investigation:
Professionals or others reporting a child missing to the police should not make a judgement about the level of risk. This decision will be made by the police on the basis of the information provided.
Children of compulsory school age who are not registered pupils at a school and are not receiving suitable education otherwise than at a school. Children missing education are at significant risk of underachieving, being victims of harm, exploitation or radicalisation, and becoming NEET (not in education, employment or training) later in life.
Children missing education should not be confused with children missing from. These are children who run away from school, or have missing episodes during the time they should be at school.
Parents and those with parental responsibility are normally expected to have undertaken the following basic measures to try to locate the missing child, if considered safe to do so. Anyone else who has care of a child without parental responsibility should take all reasonable steps to locate the child and ascertain their safety. Professionals working with families should support parents and carers in taking the following necessary steps;
At the point where a parent / person with parental responsibility consider the child to be missing, they should inform the police without delay.
When reporting a child missing to the police any relevant information that might help find or support the child should be shared, including;
Anyone who has care of a child without parental knowledge or agreement should do what is reasonable to safeguard and promote the child’s welfare. In these circumstances, they should inform the police, Children’s Social Care and the parents of their whereabouts and safety. If this is not complied with, the police should consider advice or warning under the Child Abduction Act (1984), if appropriate.
The police are the lead agency for investigating and finding missing children. However, some missing children who have not been reported to the police may come to the attention of agencies. Agencies should work with families to help them recognise the risks associated with a child going missing and the importance of reporting this to the police.
When Thames Valley Police receives a report that a child is missing, they will determine the level of risk based on the answers to 10 standard risk assessment questions:
The person reporting a missing child to the police should provide the police with up-to-date information to inform decision making, as well as details of any action they have taken to trace the missing child.
When accepting a missing person report, the police will advise the caller that they will share information about the missing child and seek assistance from partner agencies to find the child. They will presume that all missing children are vulnerable unless a risk assessment determines otherwise. The police have the ultimate responsibility for determining the action that needs to be taken and when it needs to be escalated.
The continued response and classification of a child as missing is based on on-going risk assessment and undertaken in line with current police guidance.
If a child is risk assessed to be recorded as ‘no apparent risk’, their details will be added to the Police National Computer (PNC) and an appropriate call-back time agreed with the caller. This will be dependent upon the risk assessment, and will remain subject to constant review in light of new information and changing circumstances. When the call back time is reached, the police will call the reporting person and review the 10 questions. If at that time, or earlier, there is information to indicate a higher or increased level of risk, the police will change the status of the missing child and officers will be deployed to commence a missing person investigation.
Where the police have risk assessed a missing child to be ‘no apparent risk, it will be the responsibility of the reporting person to collect the child and establish the reasons behind their absence once they are located. The police will not conduct a safe and well check unless crimes or other safeguarding issues are suspected.
Where risk is identified, either to the missing child or to the public, as a result of responses to the standard risk assessment questions, the police response will be determined by the identified level of risk (see risk assessment table above). A police officer will visit the reporting person and commence a missing person investigation.
A missing child would be prioritised as ‘high risk’ where:
All high risk cases will be led by a senior police officer.
Police officers will:
The police will undertake a secondary investigation to identify any incidents or issues which may inform the risk assessment or help locate the child more quickly, e.g. domestic violence, child protection reports, the child is in care, potentially at risk from child exploitation or another crime, or particularly vulnerable for any reason. Police should consider contacting Children’s Social Care and the risk assessment must be continually reviewed.
In some cases, the police may feel it is necessary to publicise information relating to a missing chid via the media. They may also utilise the website facility of the UK Missing Person’s Unit.
The police may also utilise ‘Text Safe’ as this provides a way of proactively texting a missing person’s mobile phone with a message from Missing People about the service. This lets the missing person know that we care for their safety and want to help, and encourages them to get in touch.
The police are responsible for liaising with the family as well as with other agencies and force areas. If the child is in care, it may be more appropriate for Children’s Social Care to undertake enquiries with the family and other agencies, and report their findings back to the police. This approach should be decided on a case-by-case basis.
The local Police Missing Person Co-ordinator is the single point of contact for all agencies. Out of weekday office hours the local Duty Inspector is the contact. Both can be contacted via 101.
A missing child would be prioritised as ‘medium risk’ where the risk of harm to the subject or the public is assessed as likely but not serious. This category requires an active and measured response by the police and other agencies in order to trace the missing person and support the person reporting. This will involve a proactive investigation and search in accordance with the circumstances to locate the missing child as soon as possible.
In cases where the report is initially made to Children’s Social Care the child of concern should still be referred to the police on 101. In cases where the report to Children’s Social Care was from a third party, there should be agreement, informed by risk assessment, about who makes this report.
All missing persons are reviewed by the Duty Shift Inspector during their tour of duty. Any child who is missing will be referred by the police to Children’s Social Care within 24 hours.
Children’s Social Care must be notified immediately in the case of any high risk missing children.
Where a child discloses a safeguarding issue, there are concerns about a child’s vulnerability or that the child may be at risk of significant harm, the police should make a referral to Children’s Social Care as soon as this becomes evident.
If the child has been missing for more than 24 hours, the case will be reviewed at the police daily management meeting.
In all high-risk cases, or once a child has been missing for over 24 hours, the police, in consultation with partner agencies, must consider a media strategy, although as stated previously, caution must be exercised as in some cases a media appeal could increase the risk to the child. Each case to be treated on its own merits. Such an approach is not routine but is usually a response to very serious concerns for the child’s safety. Either carers or the police may suggest such an approach. Normally, such decisions to publicise will be made jointly, and where appropriate, in consultation with parents and Children’s Social Care. However, for operational reasons primacy over such decisions must lie with the police.
When a child deemed to be medium risk has been missing for more than 48 hours, the case will be reviewed by a Detective Inspector.
All missing persons are notified to the UK Missing Person’s Unit (National Crime Agency) after 48 hours, or earlier if the child is at high risk of harm.
When a child has been missing for over three days, Children’s Social Care will convene a strategy meeting. Children’s Social Care will call a strategy meeting sooner if they consider the child is likely to suffer significant harm. The meeting will review:
Further reviews will take place at least every five days thereafter or earlier, if deemed appropriate.
If the child has been missing for more than 10 weeks, the Missing Person Co-ordinator will ask for the PNC entry to remain in place for up to a year.
Section 13 Children Act 2004 requires local authorities and other named statutory partners to make arrangements to ensure that their functions are discharged with a view to safeguarding and promoting the welfare of children. This includes planning to prevent children from going missing and to do everything possible to ensure their safe return when they do go missing.
The Local Authority should have a named senior manager within Children’s Services who is responsible for monitoring policies and performance relating to children who go missing from home or care.
The Local Authority must ensure that all incidents where children go missing are appropriately risk assessed, and should record all incidents of looked after children who are missing or away from placement without authorisation.
Children who are looked after should have information about and easy access to help lines and support services including emergency accommodation. Support should also be made available to families to help them understand why the child has gone missing and how they can support them on their return.
The local authority should consult with the police regarding what action should be taken to share information about a missing child who is looked after, subject to a child protection plan or a child in need. This should include an assessment of whether to release information to the media. The local authority should also notify other local authorities according to the degree of concern. Consideration should also be given to whether the child or their family has links to other areas either within the UK or abroad.
On receipt of a notification from another local authority, a flag should be added to the electronic record system for Children’s Social Care and consideration should be given to notifying health and other relevant partners.
In all circumstances where a child goes missing, local safeguarding procedures should be followed. If there is concern that the child may be at risk of significant harm if returned home, a referral should be made to Children’s Social Care so that an assessment can be undertaken and where necessary arrangements made for accommodation.
MACE is a multi-agency risk management meeting that seeks to ensure that children living in Buckinghamshire are effectively safeguarded and protected from harm in cases where:
High risk means the risk posed is immediate and there are substantial grounds for believing that the subject is in danger through their own vulnerability; or may have been the victim of a serious crime; or the risk posed is immediate and there are substantial grounds for believing that the public is in danger.
Repeat missing person means someone who is reported missing three times or more in a 90 day period.
Information is shared between agencies and actions set with the intention of reducing the risk to children, providing early intervention and considering how harmful activities can be disrupted.
MACE does not replace the provisions of Section 17 (Child in Need) or 47 (Child in need of protection) of the Children Act. It compliments statutory processes by helping to ensure that the bigger picture is considered, that action to safeguard is being completed and the appropriate multi-agency response is in place.
See also Multi-Agency Child Exploitation Protocol.
When a 16 or 17 year old goes missing they are no less vulnerable than younger children and are equally at risk, particularly of sexual exploitation or involvement with gangs.
When a 16 or 17 year old presents as homeless, Children’s Social Care must assess their needs as for any other child. Where this assessment indicates that the young person is in need and requires accommodation under Section 20 of the Children Act 1989, they will usually become looked after.
The accommodation provided must be suitable, risk assessed and meet the full range of the young person’s needs. The sustainability of the placement must be considered. Children aged 16 or 17 who have gone missing and are at risk of homelessness may be placed in supported accommodation, with the provision of relevant specialist support. For example, a specialist service might be provided for those who have been sexually exploited, or at risk of sexual exploitation.
Local authorities should have regard to:
Professionals should be aware of the ‘hidden missing’. These are children who have not been reported missing to the police, but have come to an agency’s attention after accessing other services. There may also be trafficked children who have not previously come to the attention of children’s services or the police. Research demonstrates that children from black and minority ethnic groups, and children that go missing from education are less likely to be reported as missing.
Some of the children looked after by the Local Authority may be unaccompanied asylum seeking children or other migrant children. Some children in this group may have been trafficked into the UK and may remain under the influence of their traffickers even while they are looked after. Trafficked children are at high risk of going missing, with most going missing within one week of becoming looked after and many within 48 hours. Unaccompanied migrant or asylum seeking children who go missing immediately after becoming looked after should be treated as children who may be victims of trafficking. See also, Unaccompanied Asylum Seeking Children.
Children who have been trafficked may be exploited for sexual purposes and the possible link to sexual exploitation should be considered. Professionals should also refer to the Multi Agency Child Exploitation Protocol.
The assessment of need to inform the care plan will be particularly critical in these circumstances and should be done immediately, as the window for intervention is very narrow. The assessment must seek to establish
In conducting this assessment, it will be necessary for the Local Authority to work in close co-operation with the UK Human Trafficking Centre and immigration staff who will be familiar with patterns of trafficking into the UK. Immigration staff should be able to provide advice on whether information about the individual child suggests that they fit the profile of a potentially trafficked child.
Provision may need to be made for the child to be in a safe place before any assessment takes place, and for the possibility that the child may not be able to disclose full information about their circumstances immediately. The location of the child should not be divulged to any enquirers until their identity and relationship with the child has been established, if necessary with the help of the police and immigration services. In these situations the roles and responsibilities of care providers must be fully understood and recorded in the placement plan. Proportionate safety measures that keep the child safe and take into account their best interests should also be put in place to safeguard the child from going missing from care or from being re-trafficked.
It will be essential that the local authority continues to share information with the police and immigration staff concerning potential crimes against the child, the risk to other children, or other relevant immigration matters.
Safeguarding Children Who May Have Been Trafficked: Practice Guidance (gov.uk) contains practical guidance for agencies that are likely to encounter children who may have been trafficked.
The NSPCC Child Trafficking Advice Centre (CTAC) can provide advice and information to professionals who have concerns that a child may have been trafficked. CTAC can be contacted at free phone number: 0808 800 5000, Monday to Friday 9.30am to 4.30pm or email [email protected].
Where it is suspected that a child has been trafficked, they should be referred by the Local Authority into the UK’s victim identification framework, the National Referral Mechanism (NRM).
Grooming is when someone builds an emotional connection with a child to gain their trust for the purposes of abuse or exploitation. Children can be groomed online or in the real world, by a stranger or by someone they know – for example a family member, friend or professional. Groomers may be male or female. They could be any age. Many children don’t understand that they have been groomed, or that what has happened is abuse.
Children can be groomed for the purpose of sexual abuse as well as other forms of exploitation including involvement in criminal and extremist activity. Children who are missing are more vulnerable to being groomed and may also go missing as a result of being groomed.
Children can suffer harm when exposed to extremist ideology. This harm can range from a child adopting or complying with extreme views which limit their social interaction and full engagement with their education, to children being groomed for involvement in violent attacks.
Children can by exposed to harmful, extremist ideology in the immediate or extended family, or relatives/family friends who live outside the family home but have influence over the child’s life. Older children might self-radicalise over the internet or through the influence of their peer network – in this instance their parents might not know about this or feel powerless to stop their child’s radicalisation.
Going missing is a risk factor in relation to radicalisation:
CSE is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child under the age of 18 into sexual activity in exchange for something the victim needs or wants, and/or for the financial advantage or increased status of the perpetrator or facilitator.
The victim may have been sexually exploited even if the sexual activity appears consensual. CSE does not always involve physical contact; it can also occur through the use of technology.
Involvement in exploitative relationships is characterised by the limited availability of choice as a result of their social, economic or emotional vulnerability.
A common feature of CSE is that the child does not recognise the coercive nature of the relationship and does not see themselves as a victim of exploitation.
Going missing is a significant risk factor in relation to CSE:
Because there is such a strong link between children going missing and risk of sexual exploitation, professionals should always assess whether a child who has gone missing is being sexually exploited or at risk of being sexually exploited.
Professionals should also refer to Sexual Exploitation and Abuse, and can also contact the First Response Team for advice.
Children who go missing from care, home and education also need safeguarding against the risk of being criminally exploited by organised crime groups (OCGs) in relation to the supply of drugs. For example, some children have become involved in what has become known as the ‘county lines’ issue. This involves children being used by gangs to transport and distribute drugs outside of London and other major cities as drug sales operations are expanded into the home-counties and beyond. Involvement in county lines and criminal exploitation places children at increased risk of serious violence.
When a child in care goes missing it is the responsibility of the carer to undertake the basic measures as outlined to try and locate the missing child. When the child is established as missing and the carer contacts the police, it is important that they make it clear that they are reporting the child as missing. In addition to sharing all the relevant information, they should inform the police that the child is in care and under what legal orders. The carer should always ask for, and record, the Police Incident Number.
If a child goes missing out of office hours, the carer should inform the Buckinghamshire Out of Hours Emergency Duty Team (see Local Contacts) and follow their agency’s policies and procedures.
It is important to note that local authorities have very similar duties and responsibilities towards 16 and 17 year old care leavers as they do to children in care and for the purposes of this guidance, the response to a missing care leaver age 16 and 17 year old should be the same.
Local authorities continue to have a range of responsibilities towards children leaving care until the young person’s 21st birthday and in some instances their 25th birthday. It is good practice to follow the guidance set out below whilst a young person remains ‘leaving care’.
Care leavers, particularly 16 and 17 year olds, are vulnerable to sexual exploitation and may go missing from their home or accommodation. Local authorities must ensure that care leavers live in “suitable accommodation” as defined in Section 23B (10) of the Children Act 1989 and Regulations 9(2) of the Care Leavers Regulations. In particular young people should feel safe in their accommodation and the areas where it is located. Local authorities should ensure that pathway plans set out where a young person may be vulnerable to exploitation, trafficking or going missing, and put in place support services to minimise this risk.
When a child is placed out of their local authority area, the host Local Authority must be notified by the allocated social worker in advance of the placement. The responsible authority should seek to ensure that the child has access to the services they need. Any missing report whilst the child is out of county must still be recorded on LCS by the allocated social worker.
It is possible that during a missing episode the child will return to the area of the responsible authority. It is therefore essential that liaison between the police and professionals in both authorities is well managed and coordinated.
This procedure should be followed with additional reference to policies and procedures that apply in the host authority.
Sometimes a looked after child may be away from their placement without authorisation. While they are not missing because their whereabouts is known, they may still be at risk. The carer or social worker should take reasonable steps to ascertain the wellbeing of the child including, when appropriate, visiting the location. However, if there is a concern the child may be at significant risk of harm to themselves or to others then the police should also be notified in order that appropriate safeguarding measures can be taken. This should not be confused with reporting a child missing. Where appropriate, the social worker should consider whether a strategy meeting is required.
Local authorities have a duty to place a looked after child in the most appropriate placement to safeguard the child and minimise the risk of the child going missing. The care plan and the placement plan should include details of the arrangements that will need to be in place to keep the child safe and minimise the risk of the child going missing from their placement.
Where a child already has an established pattern of going missing, the care plan should include a strategy to keep the child safe and minimising the likelihood of the child running away in the future. This should be discussed and agreed as far as possible with the child and with the child’s carers and should include detailed information about the responsibilities of all services, the child’s parents and other adults involved in the family network.
Independent Reviewing Officers (IROs) should be informed about missing episodes and they should address these in statutory reviews.
Designated health professionals for Looked After Children should be informed by the allocated social worker of children missing from care who are deemed to be ‘high risk’. They should be included in any multiagency strategy meetings or activity to manage the child’s retrieval and any subsequent health needs.
Whenever the whereabouts of a looked after child is not known, the foster carer or the manager on duty in the children’s home is responsible for carrying out initial checks to see if the child can be found. For example, if a child was supposed to have returned home from school but has not arrived within the normal journey time, checks could include finding out if there are transport delays, phone calls to the child, phone calls to the school to see if the child has been delayed etc. If these initial checks do not succeed in locating the child or there are still concerns that, despite contact being made with the child they are at risk, the individuals and agencies listed below should be informed.
It is important that a deadline is set at the outset of initial checks so that they don’t continue beyond a reasonable timeframe. What timeframe is reasonable should be based on an assessment of the risks relating to the individual child. In some cases, there might be particular reasons to be worried for the child’s safety immediately and the agencies listed below should be contacted straight away alongside continued attempts to contact the child.
The following individuals and agencies should be contacted when a looked after child is missing:
The carer/s should take all reasonable steps, which a good parent would take, to secure the safe and speedy return of the child based on their own knowledge of the child and the information in the child’s placement plan. If there is suspected risk of harm to the child the carer/s should liaise immediately with the police.
Initial discussions between the allocated children’s social worker and the police should include agreement on an immediate strategy for locating the child. The strategy should incorporate a range of actions to locate and ensure the safe return of the child, and clarity around who will undertake these actions. Aspects to cover in the strategy include:
Within 3 days, a strategy meeting between relevant parties should take place. This should include the police, the child’s social worker and the care provider and other relevant parties. The action plan and risk assessment should be reviewed and updated.
Regular multi-agency meetings should be held at least monthly to update the action plan and share information.
Details of all missing children are shared with senior managers in children’s social care, including the Director of Children’s Social Care, who may request a ‘Need to Know’ form to be completed which is sent to the Corporate Director and used to notify the Lead Member.
Any publicity will be led by the police. The use of harbouring notices etc. will be agreed at the missing from care meeting. Recovery Orders may be used where the child is Looked After.
During the investigation to find the child, regular liaison and communication should take place between the police, Children’s Social Care and any other agencies involved. In the case of a child placed out of area, both the responsible local authority and the host local authority should be involved.
The authority responsible for the child should ensure that plans are in place to respond promptly once the child is found and for determining if the placement remains appropriate.
When a looked after child / care leaver has been located, care staff/ foster carers should promptly inform the child’s social worker and the Independent Reviewing Officer. If the child was not located by the police, then they should also be informed. The police will then arrange a safe and well check and trigger a return home interview.
The attitude of all practitioners towards a child which has been missing can have a big impact on how they will engage with any subsequent investigations and planning. A supportive approach, actively listening and responding to a child’s needs will have a greater chance of preventing the child from going missing again and safeguarding them against any risks.
Children missing from home are subject to risks and vulnerabilities similar to those for children who are looked after.
If the whereabouts of the child are known or suspected, it is the responsibility of the parents or carers to arrange for the child’s return. In exceptional circumstances, in the interests of the safe and speedy return of the child, the police may agree to requests from parents or carers to assist. All agencies need to work together to agree the most appropriate and safe return for the child.
The police will respond to any notifications of children missing from home in line with this procedure and their own procedures.
The usual child protection procedures must be initiated whenever there are concerns that a child who is missing may be suffering or likely to suffer, significant harm. For example:
Where the child meets the criteria for referral to Children’s Social Care, the Local Authority will ensure that an assessment takes place to determine the best course of action.
Where the child is already known to Children’s Social Care (for example they are subject of a child protection plan, or the subject of a Section 47 enquiry) a strategy meeting should be arranged as soon as practicable and within no more than 3 days. Representatives from the Police Missing Persons Unit and the Child Abuse Investigation Unit (CAIU) should attend the strategy meeting, as well as other practitioners involved with the child. If the child has returned prior to the date of the strategy meeting, it is not a requirement for the meeting to go ahead.
A safe and well check will be undertaken by the police as soon as possible and within 24 hours of a child returning from a missing episode. A safe and well check will not be conducted over the telephone. The purpose is to check for any indications that the child has suffered harm; where and with whom they have been; and to give them an opportunity to disclose any offending by, or against them.
Where a child goes missing frequently, it may not be practicable to see them every time they return. In these cases, a reasonable decision should be taken in agreement between the police and their child’s parent or carer, or their Social Worker with regard to the frequency of such checks. Consideration must be given to the link between frequent missing episodes and serious harm.
The assessment of whether a child might go missing again should be based on information about:
If further information comes to light as a result of the safe and well check, where relevant the police will share this information with Children’s Social Care.
If the child makes an allegation of crime that occurred whilst they were missing or that contributed to them going missing, the police will record this allegation and take appropriate action. If it is apparent, upon return, that a child has been the victim of a crime whilst missing, or that there is risk or a crime in relation to the circumstances involved in the missing episode, the police will instigate further enquiries.
In any situation which indicates that the child may have been subject to, or at risk of, significant harm, a referral must be made to Children’s Social Care in accordance with these safeguarding procedures.
Consideration must be given to securing evidence by police including by forensic examination. For sexual offences, professionals should consider an urgent referral to the SARC.
When a child is found they must be offered a return home interview to talk about going missing. Providing children with an opportunity to talk is key to safeguarding them. Return home interviews are designed to support a child in exploring his or her feelings and concerns; it should be gentle and inquisitive, not adversarial or seeking to attribute blame.
Return interviews should be completed by someone independent of their parents or carers. In Buckinghamshire they are usually conducted by staff from Barnardos R U Safe? but on some occasions may also be completed by other agencies. It is important to acknowledge that a returning child may well share different parts of their experience with different people. It is the responsibility of all agencies therefore, to attend to issues of immediate safety, future support and safeguarding needs, and to share relevant information in a way which respects and safeguards children.
The return home interview will be carried out within 72 hours of the child returning to their home or care setting, unless there are exceptional circumstances. The child should be seen on their own unless they specifically request to have someone with them. The child should be offered the option of speaking to an independent representative or advocate.
Where a child is placed out of area, the responsible local authority should ensure the return home review interview takes place, working closely with the host authority where appropriate.
The return home interview and actions that follow from it should:
Where appropriate the return home interview may also gather the views of the parents / carers. Parents and/or carers are sent a letter by R U Safe? following notification of their child going missing. This gives them the opportunity to provide any relevant information and intelligence they may be aware of. This should help to prevent further instances of the child going missing and identify early the support needed for them.
The interview may result in a referral being made to other services that can provide support to meet the assessed needs of the child.
Following a missing episode, Children’s Social Care, the police and other relevant agencies should continue to work together to understand and meet the ongoing needs of the child.
There is a strong link between repeat missing episodes and a risk of significant harm. If a child continually runs away, the actions undertaken following earlier missing episodes need reviewing and alternative strategies considered. This will include a referral to the Missing and Exploitation Hub for high risk missing children or those that go missing more than 3 times in 90 days (see above for further detail).
In the case of children looked after, children’s homes staff and foster carers should be supported to offer a consistent approach to the care of children, including being proactive about strategies to prevent children from running away; and to understand the procedures that must be followed if a child goes missing. There is evidence to show that children in care do not respond to one off or reactive return home interviews as well as children who go missing from home. A more consistent, relationship based approach is often required.
Where a child is, or has been, persistently absent without permission from a children’s home; or is at risk of harm, the children’s home should ask the local authority that looks after the child to review that child’s care plan.
Difficulties can arise when missing children are found but do not want to return. Under the Children Act 1989, where there is reasonable cause to believe that the child could suffer significant harm the police can take the child into Police Protection, and remove to suitable accommodation which could include the home from which the child originally went missing. The police are not given the power to use force to take children into Police Protection. There will be occasions when a child is found in a location that may be considered unsuitable, but where there would not be legal grounds for taking them into Police Protection. In such cases, the police and the accountable manager from the responsible Children’s Social Care will need to liaise to discuss what steps may be necessary in order to safeguard the child’s welfare. Consideration may need to be given to location and recovery orders.
This section should be read in conjunction with the Government’s statutory guidance for children missing education.
Statutory guidance defines children absent from education as those who are not on a school roll or receiving suitable education otherwise than at school. Those who are regularly absent or have missed 10 school days or more without permission may be at risk of becoming ‘children absent from education’. This should be distinguished from children who are missing from school or another form of education.
The Local Authority has a duty under section 436A of the Education Act 1996 to establish (so far as it is possible to do so) the identities of children in our area who are of compulsory school age but who are not registered pupils at a school or receiving some other form of suitable education.
The Children’s Services Protocol for Children Missing Education sets out local arrangements for ensuring all children not receiving a suitable education are identified quickly and effective tracking systems and support arrangements are put in place.
In line with the above Protocol, the Children Absent from Education Officer must be notified after 10 days of any children thought to be absent from education through the following routes:
As a result of daily registration, schools are particularly well placed to notice when a child has gone missing. This section provides guidance for schools where they are concerned that a child has gone missing.
If a member of school/educational establishment/college staff becomes aware that a child may have run away or gone missing, they should try to establish with the parents/ carers, what has happened. If this is not possible, or the child is missing, the designated safeguarding teacher/advisor should, together with the class teacher, assess the child’s vulnerability.
From the first day that a child does not attend school and there is no explanation or authorisation of the absence, the following steps should be taken:
In the following circumstances a referral to Children’s Social Care and /or the police should always be made promptly:
The following questions may assist a judgement on whether or not to inform Children’s Social Care and the police:
If the judgement reached on day one is that there is no reason to believe that the child is suffering, or likely to suffer, significant harm, then the school may delay making a referral to Children’s Social Care. They should continue to make reasonable enquiries to establish what has happened, for example checking with all members of staff the child may have had contact with, checking with the pupil’s friends and their parents, siblings and known relatives.
The length of time that a child remains out of school could, of itself, be an alerting factor of risk of harm to the child. Accordingly the assessment of risk should be ongoing and a referral to Children’s Social Care should be made at any point where there is reasonable cause to believe that the child is suffering or is likely to suffer significant harm. If there is no reasonable cause to believe that the threshold for significant harm has been met, the school should continue to take reasonable action to ascertain the whereabouts of the child, and in line with the Local Authority Protocol for Children Missing Education (CME), a referral should be made to the Children Missing Education Officer after 10 days.
Extended leave of absence can be authorised by the head teacher, at which point a return date is set. In these cases the time line for enquiries starts from when the child does not attend school on the expected return date, not from the day the extended leave started.
The CME team will make enquiries by visiting the child’s home. They should also check databases within the local authority, use agreed protocols to check other relevant local databases, check with agencies known to be involved with the family and with any other local authorities where the family has previously lived or to which the family may have moved.
The child’s circumstances and vulnerability should be regularly and jointly reviewed and reassessed by the school’s designated safeguarding lead and the local authority’s CME Officer. Other agencies should be involved in the discussions as appropriate.
This section applies to children who are ‘subject to restriction’ i.e. who have:
Where the whereabouts of a child subject to restrictions is not known, a missing person’s referral must be made by Home Office staff to the police, the UK Missing Person’s Unit and Children’s Social Care in a number of circumstances including:
If it is believed by Home Office staff that a child is being coerced to abscond or go missing, this must be reported as a concern that the child has suffered or is likely to suffer significant harm to the local police and children’s social care services.
Notifications will also be made where a missing child is found by Home Office staff.
The local authority and health are responsible for:
The police are responsible for:
The local authority will also notify the Home Office Evidence and Enquiry Unit when a child in their care goes missing or when a missing child returns or is found. The Home Office must maintain regular weekly contact with the local authority and the police until the child is found and record all contact with the police and local authority.
When a child subject to restrictions is found by Home Office Staff, the local police and local authority must be informed immediately. In consultation with the local police and Children’s Social Care, a decision will be made as to where the child is to be taken, if they are not to be left at the address where they are encountered. The Home Office must follow up enquires with the local police and children/adult services in order to identify if there are any safeguarding issues.
When a child subject to restrictions is found by the police or local authority. The Home Office must be notified.
RELATED GUIDANCE
Born into Care: Best Practice Guidelines and Other Resources (Nuffield Family Justice Observatory)
There is no single accepted definition of a concealed pregnancy, but it covers situations where a woman, through fear, ignorance or denial, does not accept, or is unaware of, her pregnancy. It can include no, or late, engagement with maternity services, such as presenting at hospital in labour or delivering the child with no medical intervention.
It can cover a variety of situations such as:
Women may conceal or deny their pregnancy for a variety of reasons including:
Whilst there is a criminal offence of concealment of birth (the secret disposal of the dead body of an infant to conceal knowledge of the child’s birth), there is no criminal offence of concealment of pregnancy. A woman with mental capacity is free to choose not to engage with maternity services. However, where the woman does not have mental capacity or there is uncertainty as to mental capacity, legal advice should be sought. Lack of mental capacity may be due to factors such as learning disability, mental health or age (see also Mental Capacity and Consent chapter). If the mother is a child herself, a referral should be made to children’s social care. Action may be required to safeguard the mother and / or the child once born. If she is less than 16 years of age, a criminal offence may have been committed and police should be informed for further investigation.
Lack of antenatal care presents a risk to the unborn child due to lack of assessment of the maternal history, gestational age and health of the pregnancy, and research has shown that women who do not engage, or engage very late, with maternity services are at higher risk of maternal and foetal complications.
Risks for the baby include:
Where there is considered to be a risk of significant harm to the child, a referral to children’s social care should be made (see Referrals chapter). Consideration should be given to the reason for the concealment and a risk assessment of the reason undertaken by means of a multi-agency assessment (see also Assessments chapter).
Previous concealed pregnancies are a risk factor for future concealed pregnancies, and multi-agency information sharing is an important consideration.
Action to safeguard a child may be necessary before the child is born where there are concerns around the ability of the parents to effectively care for and safeguard the child once born. This may include:
Born into Care: Best Practice Guidelines for When the State Intervenes at Birth (Nuffield Family Justice Observatory) sets out guidelines to inform multi-agency practice when action is taken to safeguard children at birth:
Any practitioner who has concerns about the welfare of the unborn child should discuss with their safeguarding lead and consider whether a referral needs to be made to local authority children’s social care. This should be done without delay if there is a concern that the child is likely to suffer significant harm (see Referrals chapter).
The focus of multi-agency work should be on assessing the ability of the parent/s to protect and care for the child once born, what support needs to be put in place to facilitate this, action needed to safeguard the child and plans for the birth.
An early help assessment may be undertaken to assess what help needs to be put in place. Where there are concerns that the child may be at risk of significant harm once born, a child protection conference should be held to enable agencies to share all relevant information and reach a decision as to whether the child will be made subject to a child protection plan at birth and a core group established to implement the child protection plan (see Child Protection Conferences and the Child Protection Plan chapter).
Timescales should allow for the possibility of premature birth, especially where there are risk factors such as substance misuse by the mother or previous premature birth/s.
Legal advice must be sought where concerns are such that the child needs to be removed from the parents at birth. Court orders cannot be granted in respect of the child until it is born, but arrangements must be made so that an application for an interim care order can be made as soon as the child is born and / or joint risk assessments to keep mum and baby safe.
A pre-birth planning meeting should be held with relevant agencies to set out the birth arrangements and plan for the baby after birth. This should contain sufficient detail of the management of any risks. The plan should cover necessary steps to safeguard the child immediately after birth, such as:
RELEVANT CHAPTERS
Multi-Agency Risk Assessment Conference (MARAC)
RELEVANT INFORMATION
Domestic Abuse Statutory Guidance (Home Office)
Controlling or Coercive Behaviour Statutory Guidance Framework (Home Office)
Domestic Abuse: How to get Help (Home Office)
SafeLives – Resources for Professionals working with victims of domestic abuse and their families
The Domestic Abuse Act 2021 provides a definition of domestic abuse.
It is the behaviour of one person towards another where:
Behaviour is defined as abusive if it consists of any of the following:
It does not make any difference whether the behaviour is a single incident or consists of a number of incidents over a period of time.
Economic abuse is any behaviour by a person that has a negative impact on the other person’s ability to:
Children are recognised as victims of domestic abuse if they see, hear, or experience the effects of the abuse, and are related to the victim and / or perpetrator of the domestic abuse, or if the victim and / or perpetrator have parental responsibility.
The definition of domestic abuse also includes ‘honour’ based abuse (see ‘Honour’ Based Abuse chapter), female genital mutilation (see Female Genital Mutilation chapter) and forced marriage (see Forced Marriage chapter).
Domestic abuse also includes child-to-parent abuse.
See also Controlling or Coercive Behaviour Statutory Guidance Framework (Home Office)
Controlling behaviour is a range of acts designed to make a person subordinate and/or dependent by isolating them from sources of support, exploiting their resources and capacities for personal gain, depriving them of the means needed for independence, resistance and escape and regulating their everyday behaviour.
Coercive behaviour is an act or a pattern of acts of assault, threats, humiliation and intimidation or other abuse that is used to harm, punish, or frighten their victim.
Both coercive and controlling behaviour can apply to people who are no longer in a relationship but were previously.
The Act introduced the term ‘personally connected’. This applies to people who:
Victims of domestic abuse do not solely come from one gender or ethnic group. Abuse occurs in same sex relationships, is committed by young people against other family members or partners (teenage domestic abuse is the most common), as well as abuse of older relatives or those with physical or learning disabilities. Domestic abuse occurs irrespective of social class, racial, ethnic, cultural, religious or sexual relationships or identity.
Domestic abuse has a significant impact on children and young people of all ages (up to 18 years old)
Section 76 Serious Crime Act 2015 created the offence of Controlling or Coercive Behaviour (CCB) in an intimate or family relationship.
Practitioners should be mindful of how CCB overlaps with other offences such as stalking, harassment and assaults.
Experience of domestic abuse is recognised as an Adverse Childhood Experience (ACE) and can contribute towards early trauma. The presence of domestic abuse has been identified as a risk factor for child physical and emotional abuse, with children who were exposed to domestic violence being more likely to be physically abused and neglected.
Young people can also experience abuse in their own relationships (‘peer on peer abuse’). Experiencing abuse in their own intimate relationships can be hugely damaging for young people and abuse in teenage relationships should be taken just as seriously as in adult relationships.
Broadly, some of the impacts that domestic abuse can have on children can include:
Non-physical forms of domestic abuse like coercive control have a significant impact on children and professionals focused on physical acts of violence may fail to understand the daily experience of victims and children, how it is affecting them, and the level of risk posed by perpetrators.
On average victims experience on average 50 incidents, and over a two and a half year period, before seeking support (see SafeLives).
Interventions with adults who are experiencing or at risk of domestic abuse should seek to:
Professionals from any agency may receive a disclosure from a victim or perpetrator about domestic abuse or have concerns that such behaviour is taking place. All staff working with children and families should be familiar with the signs of domestic abuse and know how to respond.
Concerns may also be reported by a member of the extended family, friend or neighbour for example. Such information must be responded to in accordance with these procedures.
Professionals in contact with adults who are threatening or abusive to them as professionals, should be aware of the potential for that individual to be also abusive in their personal relationships. They should, therefore, assess whether domestic abuse may be occurring within the family environment.
See also SafeLives: Resources for identifying the risk victims face including the Domestic Abuse, Stalking and Harassment (DASH) checklist.
When carrying out a risk assessment, professionals should see the adult on their own.
When assessing domestic abuse and the needs of the adult living with domestic abuse, the following factors should be considered:
The professional should decide, based on any assessment and their professional judgement as to whether there is a threat to the safety of the adult or anyone else in the home environment. If the threat is imminent, the police should be contacted immediately by telephoning 999.
The police are often the first point of contact for adults experiencing domestic abuse. However the Ambulance Service and hospital Emergency Departments may also be involved as a first point of contact.
Professionals should ensure that they make a full record of all discussions, including referrals to other agencies.
Under the Domestic Abuse Act, local authorities have a duty to provide support in refuges / other safe accommodation to victims of domestic abuse and their children. In addition, all eligible homeless victims of domestic abuse automatically have ‘priority need’ for homelessness assistance.
The first priority must always be the safety and welfare of the child.
Where there is an imminent risk of serious harm, the police must be contacted and steps taken to ensure immediate protection for the child. See Immediate Protection chapter.
Children and young people may be victims of domestic abuse both directly (in their own relationships) and by witnessing the abuse of others such as a parent. Domestic abuse also includes child-to-parent abuse.
Agencies should recognise the impact domestic abuse has on children and support them accordingly. Those responding to children experiencing domestic abuse should follow existing safeguarding, risk assessment and referrals processes and procedures.
A referral should be made to children’s social care and the safeguarding children process initiated and followed. See Referrals chapter.
It is vital that young people who experience domestic abuse within their own relationships are referred through a multi-agency risk assessment, using an appropriate risk assessment tool such as the Domestic Abuse, Stalking and Harassment (DASH) checklist. See SafeLives: Resources for Identifying the Risk Victims Face.
Professionals should be equipped to identify and respond to children and young people experiencing domestic abuse, drawing on the range of support available, from early intervention to crisis stage. Best practice responses involve an integrated response which combines child safeguarding and high-risk domestic abuse expertise, particularly in relation to risk assessment and safety planning. Further details on responding to young people experiencing abuse can be found in: Children and Young People (SafeLives), Work with Young People’s Violence and Abuse (Respect) and Good Practice Guidance for Specialist Services for Children and Young People (Women’s Aid).
Once their safety has been secured, children and young people should be offered support based on their individual needs, with a range of interventions, so that each child is able to access the specialised help they require. This could include access to psychoeducational support, therapeutic services (for example, counselling) or specialist children’s victim support workers or an independent domestic violence advisor (IDVA) who is able to work with children and young people. A strengths-based approach to recovery, building on ‘the resilient blocks in the child’s life’, has been shown to be effective in interventions for children.
Professionals should recognise the dynamics, impact, and risk when responding to cases of child-to-parent abuse. Where indicated, this may include, commissioning specialised local child-to-parent abuse services. It is important that a young person using abusive behaviour against a parent or family member receives a safeguarding response.
Professionals should develop an individual response for every child and young person affected, including for siblings. Professionals must take the individual needs of the child into consideration to support them to communicate in a way they feel comfortable. This may include drawing on multi-agency approaches, working with educational psychologists and drawing on the knowledge of those who know the child best, such as their teacher or any therapists currently involved in their support. It is important that children and young people have the communication tools appropriate to report abuse and engage with professionals trained to aid their communication where needed.
The Young People’s Family Justice Board have produced some Top Tips for Professionals Working with Children and Young People who Have Experience of and Been Affected by Domestic Abuse.
All agencies have a duty to assess whether a safeguarding response is required before referring an incident to a multi-agency partnership.
The response to domestic abuse is a complex one that spans several statutory and non-statutory agencies, including but not limited to, local authorities, community-based agencies, children’s services, schools, housing, health (including mental health), drug and alcohol services, specialist domestic abuse agencies, the police and the criminal justice system. Wider organisations, such as employers and financial services institutions also have a role to play.
Agencies have a responsibility to work together effectively to provide support and protection to victims of domestic abuse. This can be through strategic planning, co-commissioning and creating joined-up services. Working together is essential to help with identifying domestic abuse at an early stage and with responding to domestic abuse in a manner that can reduce the risk of escalation. It is vital to appropriately safeguard victims, including children, regardless of the level of risk.
An effective multi-agency response means that all frontline agencies consider domestic abuse and are trained to understand both the complex dynamics and the signs of domestic abuse.
Multi-agency working should be embedded into approaches to responding to domestic abuse and should offer a range of interventions and support, from early intervention to support for high-risk cases through formalised safeguarding arrangements. These responses can include but are not limited to:
A Multi-Agency Risk Assessment Conference (MARAC) is a non-statutory process that brings together statutory and voluntary agencies to jointly support adult and child victims of domestic abuse who are at a high risk of serious harm or homicide, and to disrupt and divert the behaviour of the perpetrator(s).
See Multi-Agency Risk Assessment Conference chapter
Agencies must work together and share information to ensure they are able to draw on all the available information held within each agency to build a full picture of the victims, including children, and perpetrators. This includes looking holistically at an individual’s case and circumstances to identify appropriate multi-agency support.
All relevant information should be recorded. Information sharing is only as good as the quality of the information being shared, and the level of detail can be crucial to accurate risk assessment. For example, simply recording “there is a history of domestic abuse” does not give other professionals the level of detail needed to be able to risk assess.
There must be a lawful basis to process (including sharing) any personal data. What lawful basis is appropriate will depend on the specific purpose for the processing. For further information see Information Sharing and Data Protection chapters.
See also Domestic Violence Protection Notices (DVPNs) and Domestic Violence Protection Orders (DVPOs) Guidance (gov.uk). (During 2024, these orders will become Domestic Abuse Protection Orders and Domestic Abuse Protection Notices under Domestic Abuse Act 2021).
DVPOs are a civil order that fills a ‘gap’ in providing protection to victims by enabling the police and magistrates’ courts to put in place protective measures in the immediate aftermath of a domestic violence incident where there is insufficient evidence to charge a perpetrator and provide protection to a victim via bail conditions. It is important to note that bail with conditions and protective measures can be used simultaneously to build up greater protection for the victim.
A DVPN is an emergency non-molestation and eviction notice which can be issued by the police, when attending to a domestic abuse incident, to a perpetrator. Because the DVPN is a police-issued notice, it is effective from the time of issue, thereby giving the victim the immediate support they require in such a situation. Within 48 hours of the DVPN being served on the perpetrator, an application by police to a magistrates’ court for a DVPO must be heard.
A DVPO can prevent the perpetrator from returning to a residence and from having contact with the victim for up to 28 days. This allows the victim a degree of breathing space to consider their options with the help of a support agency. Both the DVPN and DVPO contain a condition prohibiting the perpetrator from molesting the victim.
A Domestic Violence Protection Notice and subsequent Order are aimed at perpetrators who present an on-going risk of violence to the victim with the objective of securing a co-ordinated approach across agencies for the protection of victims and the management of perpetrators.
The DVPN / DVPO process builds on existing procedures and bridges the current protective gap, providing immediate emergency protection for the victim and allowing them protected space to explore the options available to them and make informed decisions regarding their safety.
The DVPN / DVPO process does not aim to replace the criminal justice system in respect of charge and bail of a perpetrator. A DVPN will be issued in circumstances where no other enforceable restrictions can be placed upon the perpetrator.
Although the power to issue a DVPN and subsequent application for a DVPO lies with the police and ultimately the criminal justice service, the success of any such process will be reliant on the partnership work with other agencies and organisations including those that contribute to Multi-Agency Risk Assessment Conferences (MARACs) and service providers for independent domestic violence advisors (IDVAs) or other, similar services.
Engagement with the victim and the agencies referred to above at the earliest opportunity, is crucial to the success of the DVPN / DVPO process.
See Multi-Agency Risk Assessment Conference chapter
The Domestic Violence Disclosure Scheme (also known as Clare’s Law) is made up of two elements: the Right to Ask and the Right to Know.
Under the right to ask, a person or relevant third party (for example, a family member) can ask the police to check whether a current or ex-partner has a violent or abusive past. If records show that an individual may be at risk of domestic abuse from a partner or ex-partner, the police will consider disclosing the information.
Right to Know enables the police to make a disclosure on their own initiative if they receive information about the violent or abusive behaviour of a person that may impact on the safety of that person’s current or ex-partner. This could be information arising from a criminal investigation, through statutory or third sector agency involvement, or from another source of police intelligence.
Addressing perpetrator behaviour is as important as safeguarding and supporting victims. Tackling perpetrator behaviour and placing the onus on them should be a key consideration for partnership work.
Agencies should take the earliest opportunity available to consider how the behaviour of the perpetrator can be disrupted or constrained, putting the emphasis for change on that individual. The response to the perpetrator must be appropriate for the unique context and needs of the victim. For instance, victims subject to ‘honour’-based abuse may be experiencing a spectrum of behaviours from multiple perpetrators.
Where the threshold for HM Prison and Probation Service (HMPPS) statutory interventions is not available, agencies should consider creative options to address the behaviour of the perpetrator, including recourse to Youth Offending Teams, Integrated Offender Management (IOM), Multi-Agency Targeting And Co-ordinating (MATAC), Domestic Abuse Perpetrator Programmes, safeguarding, housing, Department for Work and Pensions (DWP) and the full range of quality assured perpetrator programmes. Any approaches adopted should work closely with existing arrangements, including MARAC to ensure perpetrator management teams have key information from victim-focused panels.
See also Multi-Agency Public Protection Arrangements chapter
It is important that local areas commission safe, effective perpetrator programmes which take into account the needs in their areas and are accompanied by support for any associated victims. These should be ‘as well as’ support for victims, not ‘instead of’.
Behaviour change interventions aim to challenge and support perpetrators of abuse to make long term changes to their violent and abusive behaviour. They also consider additional needs such as alcohol and substance misuse and mental health difficulties.
It is important to assess any potential risks to professionals, carers or other staff who are providing services to a family where domestic abuse is or has occurred. In such cases a risk assessment should be undertaken. Professionals should speak with their manager and follow their own agency’s guidance for staff safety. Such issues should also be discussed during supervision.
RELEVANT INFORMATION
FGM Resource Pack (Home Office) – case studies, support materials and information on specialist organisations
Free E-Learning ‘Recognising and Preventing FGM’ (Home Office)
Female Genital Mutilation (FGM) is a procedure where the female genital organs are deliberately cut, injured or changed and there is no medical reason for this. It is often a very traumatic and violent act and can cause harm in many ways. FGM can cause immediate as well as long-term health consequences, including pain and infection, mental health problems, difficulties in childbirth and/or death (see Section 2, Consequences of Female Genital Mutilation).
The age at which FGM is carried out varies according to the community. The procedure may be carried out on new-born infants, during childhood or adolescence or just before marriage or during a woman’s first pregnancy. There is no religious reason, in the Bible or Koran for example, for FGM and religious leaders from all faiths have spoken out against the practice. The exact number of girls and women alive today who have undergone FGM is unknown; however, UNICEF estimates that over 200 million girls and women worldwide have had FGM procedures.
FGM has been classified by the World Health Organisation (WHO) into four types:
Under the Female Genital Mutilation Act 2003, FGM is a criminal offence and a form of violence against women and girls.
There are no health benefits to FGM. Removing and damaging healthy female genital tissue interferes with the natural functions of women’s bodies.
Personal accounts from survivors show that FGM is an extremely traumatic experience for girls and women, the effects of which remain with them throughout their life. Young women may feel betrayed by their parents, when they are involved in the decision to have the procedure, as well as feeling regret and anger.
In England (as well as Wales and Northern Ireland), under the Female Genital Mutilation Act 2003 (‘the 2003 Act’) it:
Regardless of individual status in the UK ie. Permanent or otherwise, the same safeguarding response will be afforded to all.
A FGMPO is a civil order which can be made to protect a girl against FGM offences or protect a girl against whom a FGM offence has taken place. Breaching an order carries a penalty of up to five years in prison.
The terms of the order can be flexible, and the court can include whatever terms it thinks are necessary and appropriate to protect the girl, including to protect her from being taken abroad or to order giving up her passport so she cannot leave the country. See also: Making an Application for an FGM Protection Order (FGMPO) – Flowchart.
The most significant factor to consider when assessing if a girl may be at risk of FGM is whether her family has a history of practising FGM. In addition, it is important to consider whether FGM is known to be practised in her community or country of origin.
As FGM is illegal and therefore not discussed openly, women who have undergone FGM may not fully understand what FGM is, what the consequences are, or that they themselves have had FGM. Discussions about FGM should therefore always be undertaken with care and sensitivity.
There are a number of other factors which could indicate a girl is at risk of being subjected to FGM.
Signs that FGM may have taken place include:
If you have concerns, do not be afraid to ask a girl or woman about FGM, using appropriate and sensitive language. Women and girls sometimes say that professionals have avoided asking questions about FGM, and this can then lead to a breakdown in trust. If a professional does not give a girl / woman the opportunity to talk about FGM, it can be very difficult for her to bring this up herself.
There are screening tools that can be used to support the conversations, e.g. Guidance – FGM: Mandatory Reporting in Healthcare (Department of Health and Social Care)
FGM is illegal in England and Wales, and practitioners should act to safeguard girls who may be at risk of FGM or have been affected by it.
The girl may be at imminent risk, in which case immediate protection should be taken to protect her such as a Female Genital Mutilation Protection Order or other action such as an Emergency Protection Order or the exercise by the police of their powers of protection (see Immediate Protection chapter).
Practitioners should consult with their safeguarding lead and information should be shared with relevant agencies as appropriate to ensure a multi-agency response as necessary. A referral should be made to Children’s Social Care (see Referrals chapter).
Discussions with family members should be conducted sensitively and with use of accredited interpreters (not known to the family) as required. However, it is important to remember that the child may be at risk of harm from family members who may believe that FGM is in the girl’s best interests and may not understand the legal situation and implications. The primary consideration at all stages should be the safety and welfare of the girl.
Action should include:
Practitioners should inform their safeguarding lead and make a referral to Children’s Social Care so that further safeguarding enquiries can be made.
Regulated health and social care professionals and teachers in England and Wales have a mandatory duty to make a report to the police if they become aware of a girl having had FGM. See Section 8, FGM Mandatory Reporting Duty.
Action should include:
Whenever a girl is identified as having had, or being at risk of, FGM professionals must consider whether she is at risk of further harm, and whether there are other girls or women in her family or wider social network who may be at risk of FGM.
NHS England collects the following data from NHS acute trusts, mental health trusts and GP practices:
For more information please see Female Genital Mutilation (FGM, NHS)
Where a regulated health and social care professional or a teacher in England and Wales becomes aware of a case of FGM on a girl under the age of 18, they must report this to the police as soon as possible, preferably by the end of the next working day. They may become aware of the FGM because the girl has disclosed it to them or because they observe physical signs.
Please note: This is in addition to the safeguarding process. If a practitioner is concerned that a child has had FGM, they should also consult their safeguarding lead and make a referral to Children’s Social Care (see Referrals chapter).
See also:
Guidance – Mandatory Reporting of Female Genital Mutilation: Procedural Information (gov.uk)
Guidance – FGM: Mandatory Reporting in Healthcare (Department of Health and Social Care)
To follow.
Problematic and Harmful Sexual Behaviour (NSPCC)
Harmful Sexual Behaviour among Children and Young People: Guideline NG55 (NICE)
.
RELATED POLICIES
Concealed Pregnancy and Pre-Birth Safeguarding
RELATED GUIDANCE
Parental mental health problems (NSPCC)
Parenting and mental health problem (MIND)
Think child, think parent, think family: A guide to parental mental health and child welfare (SCIE)
Oxford Health NHS Foundation Trust provide services such as psychological services, Adult Mental Health Teams (AMHT), complex needs service, Bucks Community Eating Disorders Team (BCEDT) and adult mental health inpatient services.
This procedure has been written to improve the coordination and communication between all agencies in Buckinghamshire engaged with children and families and those adults who have mental health needs.
The procedure should be applied whenever there are concerns about the well-being or safety of children whose parents or carers have mental health needs, specifically where these difficulties are impacting, or are likely to impact, on their ability to meet the needs of their children. This procedure also applies to pregnant women who have mental health problems or where their partners are known to have mental health problems.
The Final Analysis of Serious Case Reviews (2017 to 2019) published by the Department for Education reported that 55% involved parents with mental health problems. In these cases, the mental illness of the parent had a significant impact on their parenting capacity, resulting in the death or serious injury of the children. However, it remains the case that the majority of mentally ill parents do not harm their children. It also does not mean that parents who experience mental health problems have poor parenting skills.
However, the impact of parental mental health problems can, on some occasions, lead to children and families needing additional support; or, in a small number of cases, support and multi-agency action to prevent significant harm.
The guidance is underpinned by the following principles:
Here are some messages to mental health professionals written by young people from a Barnardo’s project in Liverpool2. The messages show how important it is to keep children informed.
Tell us if there is anyone we can talk to. MAYBE IT COULD BE YOU.
Mental ill health can sometimes lead to neglect of both the adults and their children’s physical, emotional and social needs. The children may have caring responsibilities, which are inappropriate to their age and may have an adverse impact on their development. Some forms of mental ill health may cause adults to be ‘unavailable’ or not responsive to the child; or to behave in bizarre, unpredictable or violent ways towards themselves, their children or environment.
The stigma and oppression associated with adult mental ill health can impair the adult’s ability to care for the child/ren and children can carry the burden of covering for parental behaviour. It can be difficult for adults to share their situation and struggles. Children may be reluctant to talk about family problems or seek support. Practitioners need to be sensitive to this. See also Section 4, Consider the Child / Children’s Experience – What is Life Like for the Child?
At the extreme, a child may be at risk of severe injury, profound neglect or even death.
An adult carer’s mental ill health will be less likely to have an adverse effect on a child when:
A significant history of violence is a risk indicator for children, as is parental and adult non- compliance with services and treatment.
Children most at risk of significant harm are those who:
The following factors may impact the ability of an adult to provide appropriate care and increase concerns that a child may have suffered, or is at risk of suffering, significant harm:
When an agency identifies a pregnant woman experiencing mental health problems, an assessment must be undertaken to determine what services she requires and the Concealed Pregnancy and Pre-Birth Safeguarding procedure must be followed.
This must include gathering relevant information from their Primary Care Team/GP, in addition to any other agencies involvement, to ensure that the full background is obtained about any existing or previous diagnosis, or treatment for mental illness or substance misuse. This is especially important where service awareness of earlier births may need to be clarified, for example, in the case of older or overseas children. If a person has moved recently, it is advisable to seek out health records from the previous Primary Care Team/GP. It is also important to identify partners of pregnant women who have mental health or substance misuse problems.
Pregnant women in Buckinghamshire now book their maternity appointments online and these are coordinated by midwives based at the hospital and not by Primary Care Teams/GPs. As such, it is possible that a pregnant woman may not see her GP during the pregnancy and the first contact with their GP may be at the face-to-face six-week post-natal appointment. It is important that those working with pregnant women do not assume that the pregnant women are being routinely seen by their GP.
Research has shown that pregnant women with a previous history of mental health needs are particularly vulnerable to breakdown during the later stages of pregnancy and following the birth of their baby.
When a parent has a substance misuse problem, as well as mental health needs, this can put the child at particular risk, especially where the potential for dealing with the substance misuse problem is limited. Where a parent/carer has mental health and substance misuse issues, the assessment of the adult should ideally be conducted in partnership between the Mental Health Care Management Team and the Adult Substance Misuse Care Management Team.
In addition, the Final Analysis of Serious Case Reviews (2017 to 2019) and previous reviews of Serious Case Reviews have shown that the three issues of domestic abuse, parental mental ill health, and alcohol or substance misuse are not the only risk factors that may contribute to cumulative risk of harm. Other risk factors often co-exist with these factors, and potentially interact with them to create harmful environments for the children. These include issues such as adverse experiences in the parent/carer’ own childhoods, a history of criminality – particularly violent crime, a pattern of multiple consecutive partners, and acrimonious separation. Professionals should be aware of this when undertaking an assessment of risk.
This flowchart is relevant to all services in Buckinghamshire which are treating or providing any kind of service to parents, carers, or pregnant women with mental health problems.
Informed assessments and effective multi-agency/disciplinary working are the key to ensuring that children and families receive the appropriate services to meet their identified needs and manage risk.
The key to ensuring children are safe, protected, and their needs are being met where parents/carers have additional needs, is to assess parent’s/carers capacity and ascertain if additional support is required. Consider the following areas:
Are parents/carers able to provide the following:
BASIC CARE
ENSURING SAFETY
EMOTIONAL WARMTH
STIMULATION
GUIDANCE AND BOUNDARIES
STABILITY
See Continuum Of Need Threshold for further information.
If there is concern about the mental health needs of a parent/carer, the adult’s Primary Cary Team/ GP should be contacted in the first instance and a request made for information to be shared regarding any existing or previous diagnosis of mental illness, and previous or current treatment or referrals.
In order for timely sharing of this information, the Primary Care Team will need to know why the information is needed, in what timescale it needs to be provided, with whom the information will be shared (within health professionals or with other agencies), what information is being asked and whether the patient has consented to this information being shared.
Practitioners should be aware that women in Buckinghamshire who are temporarily placed in refuges may be additionally vulnerable to their mental health needs not being met and patient information between systems may be limited.
If there is an imminent danger to the person or others, including a child, the police must be contacted. Staff must ensure that their decision and agreed course of action is fully and accurately documented.
Triggers that may indicate a referral to adult mental health services for initial assessment is needed are listed below. However, this is not an exhaustive list and is provided to assist professional decision-making.
Concerns should be discussed with the person’s Primary Care Team/GP in order to agree the most appropriate course of action. It would be usual practice for the Primary Care Team/GP to assess the client in the first instance and make a referral to mental health services if appropriate. However, in some circumstances another professional may make the referral, or the client may self-refer.
A past history of mental health problems will not necessarily mean a referral is required; this will depend on what the particular diagnosis was, current mental state, how long an individual has been stable and the level of support at home.
In any instance where there is a concern about the welfare of a child, professionals should consult the Continuum of Need Threshold.
A referral to Children’s Social Care for an initial assessment or pre-birth assessment should always be made if a parent, carer or pregnant woman is considered to have significant mental health problems, as indicated by the triggers given below. A referral should always be discussed with a manager.
If there is an imminent danger to the person or others, including a child, the police must be contacted.
Speak to the family to discuss the concerns and reasons for referral. Gain a better understanding of the situation and gain consent to refer if possible.
Think family – consider all family members including all the children. Risks may be relevant to some or all of the children in the family.
Consideration should be given to a referral to Early Help in order to provide additional support and safeguard children at an early stage. Early Help in Buckinghamshire is provided by the Family Support Service.
Consider schools involvement – what support is school offering? Are they aware of the family situation? Is the school counsellor involved? Is the child’s school attendance level a concern?
Triggers that indicate referral to Children’s Social Care are listed below. However, this is not an exhaustive list and is provided to assist professional decision-making.
Where a parent or carer expresses thoughts of self-harm, an assessment of risk to the child or unborn baby must be made and consideration given to a referral to Children’s Social Care based on the level of risk. Management of self-harm risk by adult mental health services staff must include in the plan actions to support the needs of the child/children/unborn baby and there should be discussion with the organisation’s lead for child safeguarding. Where necessary, advice should be sought from First Response. Consideration must always be given to the care arrangements for the children should the adult need to be admitted to hospital.
When a parent or carer has been receiving inpatient services, in whatever setting, consideration must be given to discharge arrangements to ensure provision for the children is appropriate, and their welfare and safety has been properly assessed. A formal meeting with Children’s Social Care should be held where they are already involved or if concerns are identified. If a parent or carer discharges themselves out of hours, a referral to the Emergency Duty Team should be made to ensure the children’s welfare is protected.
Newly identified risk or changes in the risk assessment in any agency must be communicated to other relevant agencies in order that they can consider if this new information impacts on their own risk assessments. Staff must always consider that a change for one member of the family might have impact on another member, and that a Think Family approach is essential.
Where the need for referral to Children’s Social Care is unclear, this must be discussed with a line manager and/or safeguarding lead. Children’s Social Care can be consulted for advice. Staff must ensure that all decisions and the agreed course of action are signed and dated. If a referral is not made, the reasons must also be clearly documented.
All information should be shared in line with Information Sharing Advice for Safeguarding Practitioners (Department for Education).
It is essential that staff working in adult mental health and children’s services work together to ensure the safety of the child and the management of the adult’s mental health.
Joint work will include mental health workers providing all information with regards to:
Parents/Carers with mental health issues entrust professionals with, or allow them to gather, sensitive information relating to their health and other matters as part of their seeking treatment. They do so in confidence, and they have legitimate expectation that staff will respect their privacy and act appropriately.
Where there are concerns about the wellbeing of a child, the need to share information will take precedence over the patient’s right to confidentiality. However, practitioners need to consider what information is and is not confidential, and the need in some circumstances to make a judgement about whether confidential information can be shared, in the public interest, without consent.
Sensitive information can be shared if there is a clear and justifiable purpose, and consideration has been made of the safety and wellbeing of the child and others who may be affected. The more sensitive the information, the greater the child focus needs to be in order to justify sharing.
The practitioner needs to be mindful that information may need to be shared with a number of agencies, therefore the ‘need to know’ and ‘proportionality to the risk of harm’ principles apply. Where a practitioner is considering the inclusion or exclusion of sensitive information, or consent has been refused, they must discuss this with their safeguarding lead within their organisation.
If an adult’s clinical information is shared without their consent, the adult should be notified of this.
Child protection workers must assess the individual needs of each child and, within this, incorporate information provided by mental health workers. They must assess the risk and impact on each child in accordance with information provided by mental health workers and the assessment framework.
Mental health professionals must attend and provide information to any meeting regarding the potential impact of parent/carer mental health concerns on the child. These will include:
Relevant professionals from Children’s Services and other agencies supporting the child should attend Care Programme Approach (CPA) and other meetings related to the management of the parent/carer’s mental health where concerns about capacity to parent have been raised.
All plans for a child, including Child Protection Plans, will identify the roles and responsibilities of mental health and other professionals. The plan will also identify the process of communication and liaison between professionals. All professionals should work in accordance with their own agency procedures/guidelines and seek advice and guidance from line management when necessary.
Key examples of good practice in joint working:
Consideration to be given to the adult’s accommodation history, have they always lived in Buckinghamshire, have the child/children been known in another local authority?
It is important to be aware that risk assessment in mental health work and risk assessment in child protection work are two different concepts, and it can be dangerous to confuse them.
The former is concerned with predicting the likelihood of a patient’s mental health deteriorating to the point where she/he poses a risk to self and/or others. The latter involves the analysis of information to consider whether or not the children’s likely experiences are acceptable, in terms of risk of physical or sexual assault, omission of care or neglect, or threat to emotional wellbeing.
Newly identified or changes in risk in one agency’s assessment must be communicated to other relevant agencies, so that they too can consider if this new information impacts on their own risk assessments. Staff must always consider that a change for one member of a family might have impact on the other member – a ‘think family’ approach is essential.
In the event of a dispute or disagreement arising between professionals, the procedure for Escalation, Challenge and Conflict Resolution should be followed.
Any disagreements or differences should be recorded on the case file, including the views of the other party.
RELATED GUIDANCE
Support for Parents and Carers to Keep Children Safe Online (gov.uk)
Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) – guidance on responding to incidents and safeguarding children and young people.
Guidance: Education for a Connected World (UK Council for Internet Safety) – a framework to equip children and young people for digital life
Guidance: Challenging Victim Blaming Language and Behaviours when Dealing with the Online Experiences of Children and Young People (UK Council on Internet Safety) – guidance for professionals on how to effectively challenge victim blaming language and behaviours and advice on best practice
Technology is a big part of everyday life, bringing educational and social benefits and opportunities for children and young people. However, there are potential harms which children and young people may encounter when online, including online child abuse, bullying, harassment or criminal exploitation. The consequences and impact of online child abuse can be just as severe as abuse experienced offline.
The term ‘victim’ has been used within this chapter to describe a child or young person who has experienced online abuse, in any form. This includes abuse from an adult, or another child or peer. In practice, different terms may be used, for example victim or survivor. Many children or young people who have experienced online abuse would not consider themselves a victim, and would not refer to themselves as such.
The breadth of issues classified within online safety is considerable and ever evolving. Keeping Children Safe in Education Part Two: The Management of Safeguarding (Department for Education, 2024) categorises them into four areas of risk (‘the 4Cs’):
The Sexual Offences Act 2003 and the Online Safety Act 2023 set out several criminal offences in relation to harmful online activity, and these should be reported to the police for investigation of possible criminal offences (alongside any safeguarding referral).
Some of the main categories of safeguarding risks are now considered in more detail.
See also Sexual Exploitation and Abuse (Including Organised Sexual Abuse) chapter.
Indecent images of children: Making, possessing, and distributing any imagery of someone under 18 which is ‘indecent’ is illegal.
Sending a photograph or film of genitals (‘cyberflashing’): It is a criminal offence to intentionally send a photograph or film of any person’s genitals to another person either with the intention that the recipient will see the genitals and be caused alarm, distress or humiliation, or for the purpose of obtaining sexual gratification (inserted into the Sexual Offences Act 2003 by the Online Safety Act 2023).
Threatening / blackmailing children into sending indecent images / carrying out indecent acts online: This is an offence under the Sexual Offences Act 2003.
Sharing or threatening to share intimate photograph or film: This is a criminal offence under the Online Safety Act 2023. A person would ‘share’ the film/image if they, by any means, give or show it to another person, or make it available to another person. This includes electronic sharing, for example by posting a photograph or film on a website or emailing to someone. ‘Film’ or ‘photograph’ covers data that can be converted into such an image – for instance data stored on a hard drive or disc.
Sharing nudes and semi-nudes: Children may be encouraged, or may choose, to share nude or semi-nude images online with other children and young people.
Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) uses the term ‘sharing nudes and semi-nudes’ to mean the sending or posting of nude or semi-nude images, videos, or live streams by young people under the age of 18 online.
For example:
This could be via social media, gaming platforms, chat apps or forums. It could also involve sharing between devices via services like Apple’s AirDrop which works offline.
The sharing of nudes and semi-nudes can happen publicly online, in 1:1 messaging or via group chats and closed social media accounts.
Nude or semi-nude images, videos or live streams may include more than one child or young person. The term ‘nudes’ is used as it is most commonly recognised by young people and more appropriately covers all types of image sharing incidents. Alternative terms used by children and young people may include ‘dick pics’ or ‘pics’.
See also Section 3.2, Information on avoiding unnecessary criminalisation of children and:
The risk of physical and / or emotional harm can include the following.
Children being exposed to online threats and harmful online ‘fake news’
The Online Safety Act 2023 introduced offences of threatening communications and false communications.
A person commits the false communications offence if they send a message conveying information that they know to be false, intending the message to cause non-trivial psychological or physical harm to a likely audience (that is, someone who could reasonably be foreseen to encounter the message or its content). It is not necessary to show that the sender intended to cause the harm to any of the likely audience in particular.
A person commits the threatening communications offence if they send a message conveying a threat of death, serious injury, rape, assault by penetration, or serious financial loss. This includes situations where the recipient fears that someone other than the sender of the message may carry out the threat. It does not matter if the content of the message is created by the person who sends it; a message can consist of or include a hyperlink to other content.
Children being exposed to content designed to cause them physical and / or psychological harm
The Online Safety Act 2023 introduced offences of sending or showing flashing images electronically with the intention of causing harm to a person with epilepsy. The offence may be committed by a person who forwards or shares the electronic communication, as well as by the person originally sending it.
The Act also introduced an offence of encouraging serious self-harm. It includes online communications capable of encouraging or assisting another person to seriously self-harm. It also includes an omission, such as encouraging or assisting a person to stop eating or taking required prescription medication. The person committing the offence need not know, or even be able to identify, the person or persons who receive the communication. So, a person who intends that a recipient or recipients of their communication will seriously harm themselves is guilty of an offence, even though they may never know the identity of those who receive the communication.
An offence can be committed whether or not serious self-harm occurs. In addition, a person who arranges for someone else to do an act capable of encouraging or assisting the serious self-harm of another person will also be committing an offence if the other person carries out that act.
This category would also include cyberbullying.
Preventing Bullying: Guidance for Schools on Preventing and Responding to Bullying (Department for Education, 2017) provides further information on tackling this form of online harm.
Under the Sexual Offences Act 2003 (as amended) it is an offence for a person (over 18 years) to engage in sexual communication with a child (under 16 years) (section 15A), or to meet a child (under 16 years) following sexual grooming (section 15).
See also chapters on Sexual Exploitation and Abuse (Including Organised Sexual Abuse) and Multi-Agency Child Exploitation Protocol.
For further information see Radicalisation and Violent Extremism chapter
Concerns about online radicalisation can be reported to the police on 101 and / or a Prevent referral can be made, so that the victim can get safeguarding support.
Any member of the public can report terrorist content they find online through the gov.uk referral tool – more information about what to report and what happens when you do can be found on the Action Counters Terrorism campaign.
Educate Against Hate Parents’ Hub provides resources and government advice for parents and carers on keeping young people safe from extremism, including online.
The prevalence of online activity by children and young people makes it increasingly likely that children may be both victims and perpetrators of harmful online activity, which may involve the commission of criminal offences. An appropriate multi-agency response including police and safeguarding will be required in respect of all children involved. Children can abuse other children online. This can take the form of abusive, harassing, and misogynistic / misandrist messages, the non-consensual sharing of indecent images, especially around chat groups and the sharing of abusive images and pornography to those who do not want to receive such content. Child-on-child abuse can include cyberbullying, online threats of physical abuse, online threats and/or encouragement of sexual violence, online sexual harassment.
The nature of online abuse means that it can very rapidly involve multiple children, for example children sharing images online / forwarding on content, sending links of content to others and / or posting things on online platforms such as social media.
See also Harmful Sexual Behaviour chapter
This is of particular relevance in relation to the sharing of nude / semi-nude images where both victim and perpetrator are under 18.
The law criminalising indecent images of children, for instance, was created to protect children and young people from adults seeking to sexually abuse them or gain pleasure from their sexual abuse. It was not intended to criminalise children and young people. The law was also developed long before mass adoption of the internet, mobiles and digital photography.
Despite this, children and young people who share nudes and semi-nudes of themselves, or peers, are breaking the law. Making, possessing, and distributing any imagery of someone under 18 which is ‘indecent’ is illegal. This includes imagery of the person making / sending the image if they are under 18.
Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) stresses the importance of avoiding unnecessary criminalisation of children. Situations should be considered on a case by case context, considering what is known about the children and young people involved and if there is an immediate risk of harm. Often, children and young people need education and support for example, on identifying healthy and unhealthy behaviours within relationships and understanding consent and how to give it. Safeguarding action will also be required in cases where there is risk of harm.
Investigation by police of an incident of sharing nudes and semi-nudes does not automatically mean that the child / young person involved will have a criminal record. Once an incident is reported to the police, they will investigate and decide on an appropriate outcome. If an incident is found to have abusive and / or aggravating factors, the child or young person may receive a caution or conviction.
To mitigate the risk of children and young people being negatively impacted, the police are able to record the outcome of an investigation using an ‘outcome 21’ code should an incident be found to be non-abusive and have no evidence of any of the following:
This means that even though a child or young person has broken the law, and the police could provide evidence that they have done so, the police can record that they chose not to take further action as it was not in the public interest.
It is possible for an incident of sharing nudes and semi-nudes recorded on police systems with outcome 21 to be disclosed on a DBS certificate. However, information falling short of conviction or caution can only be included on a DBS certificate when an individual has applied for an Enhanced Criminal Records Check. In such cases, it would be for a chief officer to consider what information (in addition to convictions and cautions held on the Police National Computer) should be provided for inclusion. That decision must be made on the basis that the chief officer reasonably believes the information to be relevant to the purpose of the disclosure (for example, someone taking up a position working with children) and considers that it ought to be included.
Keeping Children Safe in Education Part five: Child-on-child Sexual Violence and Sexual Harassment (Department for Education, 2024) provides information on managing harm between children, including online harm, and the importance of providing ongoing support for all affected children: victims, alleged perpetrators and other children who have been directly or indirectly affected.
If a child is convicted or receives a caution for an offence, risk assessments should be reviewed and updated to ensure relevant protections are in place for all the children affected.
Anyone concerned that a child / young person may be at risk of significant harm due to online activity should make a referral to children’s social care (see Referrals chapter) so that safeguarding procedures can be implemented (see Section 7, Safeguarding Response).
In addition, there are specific referral channels for specific concerns.
Contact the police via 999 (emergency number) where:
Report other non-emergency situations (that is, those that do not require an immediate police response) by dialling 101.
If you are concerned that a child has been a victim of online sexual abuse or you are worried about the way someone has been communicating with a child online, you can report it to NCA-CEOP.
If you see sexual images or videos of someone under 18 online, report it anonymously to the Internet Watch Foundation who can work to remove them from the web and help to identify victims and survivors.
To report other forms of harmful online content (other than online child sexual abuse imagery), see Report Harmful Content. This provides advice and resources on how to report a variety of different issues you may see online including:
It also offers advice on When you Should go to the Police.
Concerns about online radicalisation can be reported to the police on 101 and / or a Prevent referral can be made, so that the victim can get safeguarding support.
Any member of the public can report terrorist content they find online through the gov.uk referral tool – more information about what to report and what happens when you do can be found on the Action Counters Terrorism campaign.
Filtering and age-appropriate parental controls on digital devices can be used to restrict children’s access to age-inappropriate content. Filtering and Monitoring Standards for Schools and Colleges (Department for Education) provides further information.
Internet Matters has step-by-step guides on setting up parental controls to control what content children can access online.
The UK Safer Internet Centre has guidance on how to switch on family-friendly filters to prevent age-inappropriate content being accessed on devices.
The NSPCC has more information for parents or carers with concerns about their child seeking inappropriate or explicit content online.
Apps to help children stay safe online
The BBC has a website and app called Own It, to help children navigate their online lives.
The UKCIS Digital Passport is a resource for care-experienced children and young people and their carers. It is a communication tool created to support children and young people with care experience to talk with their carers about their online lives.
Other useful resources include:
It is also important to ensure that practitioners working with children and young people are aware of the risks posed to children by online activity and how children can be protected and encouraged to help protect themselves. This should include being able to recognise the additional risks that children with special educational needs and disabilities (SEND) face online, for example, from bullying, grooming and radicalisation, to enable practitioners to have the capability to support children with SEND to stay safe online. Agencies should provide suitable training for staff working with children and young people.
Useful resources include:
Victim blaming is any language or action that implies (whether intentionally or unintentionally) that a person is partially or wholly responsible for abuse that has happened to them. It is harmful and can wrongfully place responsibility, shame or blame onto a victim, making them feel that they are complicit or responsible for the harm they have experienced. For example:
Guidance: Challenging Victim Blaming Language and Behaviours when Dealing with the Online Experiences of Children and Young People helps practitioners to understand that the responsibility always lies with the person who abused the child or young person. The guidance also offers practical steps to help practitioners practice and advocate for an anti-victim blaming approach, in a constructive and supportive way.
One of the greatest barriers to a child or young person seeking help and reporting online abuse, is feeling they are to blame for something that has happened to them. When practitioners working with the child or young person speak or behave in such a way that reinforces this feeling of self-blame, the impact of the abuse the child or young person has already experienced may be greater, leading to a longer recovery. In contrast, positive responses can reduce feelings of post-traumatic stress which a young person may experience as a result of abuse occurring. They can also encourage other children and young people to report their online experiences.
When victim blaming occurs, there is a risk of diminishing the child or young person’s experiences, leading to a lack of, or an inappropriate, safeguarding response. This could be by practitioners initially dealing with an incident or by those involved subsequently. This can have a devastating impact for the child or young person who has experienced abuse and make it less likely that they, or their peers, will have the confidence to disclose abuse in the future. In addition, victim blaming attitudes can prevent families, friends and wider society from recognising certain behaviours as abuse.
Where practitioners have concerns that a child is a victim or perpetrator of online harm, they should discuss with their safeguarding lead. Where it is suspected that the child is at risk of significant harm, a referral should be made to children’s social care and safeguarding processes engaged which may include a multi-agency strategy discussion (see Referrals and Strategy Discussions chapters). Where there is an imminent risk of significant harm, steps must be taken to ensure the child’s immediate safety (see Immediate Protection chapter).
A referral should be made to children’s social care where the child is already known to them, for example, they are currently, or have in the past, been the subject of an early help or child protection plan.
A referral should also be made where there are believed to be wider safeguarding issues such as several children having been affected.
The police should be informed where there is a known or suspected criminal offence. This should take place as soon as possible to enable swift preservation of evidence.
See also Section 4, Who to Contact / How to Make a Report for additional notifications in response to particular types of online harm.
Where the harm involves indecent images, the images should not normally be viewed by practitioners but should be referred to the police. Practitioners may themselves commit a criminal offence by viewing any indecent images. Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) sets out the very limited circumstances where it may be necessary to view images, such as it being unavoidable because a child or young person has presented it directly to a staff member or nudes or semi-nudes have been found on an education setting’s device or network. Practitioners must never copy, print, share, store or save indecent images – this is illegal. If any devices need to be taken and passed onto the police, the device/s should be confiscated and the police should be called. The device should be disconnected from Wi-Fi and data, and turned off immediately to avoid imagery being removed from the device remotely through a cloud storage service. The device should be placed in a secure place, for example in a locked cupboard or safe until the police are able to come and collect it.
Viewing indecent images can be distressing for both children, young people, and adults and appropriate emotional support may be required.
Schools / colleges becoming aware of incidents involving nude / semi-nude images of children should hold an initial review meeting to establish:
An immediate referral to police and / or children’s social care should be made if at the initial stage:
Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) sets out the very limited circumstances where an education setting may decide to respond to an incident involving sharing of nude / semi-nude images between children without involving the police or children’s social care. They can still choose to escalate the incident at any time if further information / concerns are disclosed later.
The decision to respond to the incident without involving the police or children’s social care should only be made in cases where the designated safeguarding lead (or equivalent) is confident that they have enough information to assess the risks to any child or young person involved and the risks can be managed within the education setting’s pastoral support and disciplinary framework and, if appropriate, their local network of support. The reasons for not referring the incident should be recorded.
All incidents relating to nudes and semi-nudes being shared need to be recorded by education settings. This includes incidents that have been referred to external agencies and those that have not.
Many instances of online harm will involve possible criminal offences and so will necessitate a police response and safeguarding response. Educational establishments are often likely to be involved as guidance tell us that many of these events are likely to involve the child’s educational experience in some way, such as images of children being widely circulated between pupils.
Children accessing alternative educational settings, voluntary activities and specialist units should be considered with the context of this policy.
Multi-agency information sharing is important to enable effective assessment of risk and identification of other children who may be affected.
See also Tier 1 – Children Safeguarding Data Sharing Agreement (DSA) and Data Protection.
Unlike female genital mutilation, male circumcision is not an illegal act in itself and is not normally a child protection or safeguarding issue. This procedure provides practitioners in Buckinghamshire with an understanding of when male circumcision may raise safeguarding children concerns and how to respond if such concerns arise.
Male circumcision is the surgical removal of the foreskin on the penis. The procedure is usually requested for social, cultural or religious reasons (e.g. by families who practise Judaism or Islam). Additionally, there are parents who request circumcision for assumed medical benefits.
There is no requirement in law for professionals undertaking male circumcision to be medically trained or to have proven expertise. Traditionally, religious leaders or respected elders may conduct this practice.
Male circumcision is a non-reversible procedure.
It is rare for circumcision to be recommended for medical reasons in boys. This is because other less invasive and less risky treatments are usually available. See Circumcision in Boys (NHS). Doctors should be aware of this and reassure parents accordingly.
The medical harms or benefits of circumcision have not been unequivocally proven, except to the extent that there are clear risks of harm if the procedure is done inexpertly.
Doctors/health professionals should ensure that any parents seeking circumcision for their son in the belief that is confers health benefits are fully informed that there is a lack of professional consensus as to current evidence demonstrating any benefits. The risks/benefits to the child must be fully explained to the parents and to the child himself, if Gillick competent.
Where parents request circumcision for their son for assumed medical reasons, it is recommended that circumcision should be performed by or under the supervision of doctors trained in children’s surgery in premises suitable for surgical procedures.
Male circumcision that is performed for any reason other than physical clinical need is termed ‘non-therapeutic male circumcision’ or NTMC.
See also Section 7, Non-therapeutic Male Circumcision – Principles for Good Practice.
Practitioners may assume that the circumcision procedure (therapeutic or non-therapeutic) is lawful provided that:
If doctors or other professionals are in any doubt about the legality of their actions, they should seek legal advice.
Consent for circumcision is valid only where the people (or person) giving consent have the authority to do so and understand the risks and implications, including that it is a non-reversible procedure.
The British Medical Association (BMA) and General Medical Council (GMC) recommend that consent should be sought from both parents having parental responsibility. Non-therapeutic male circumcision has been described by the courts as an ‘important and irreversible’ decision that should not be taken against the wishes of a parent. It follows that where a child has two parents with parental responsibility, doctors considering circumcising a child must satisfy themselves that both have the necessary parental authority and have given valid consent. Where people with parental responsibility for a child disagree about whether the child should be circumcised, the child should not be circumcised without the leave of a court.
An assessment of best interests in relation to non-therapeutic male circumcision should include consideration of:
Doctors are under no obligation to comply with a request to circumcise a child and circumcision is not a service which is provided free of charge. Nevertheless, some doctors and hospitals are willing to provide circumcision without charge, rather than risk the procedure being carried out in unhygienic conditions.
Poorly performed circumcisions have legal implications for the doctor responsible. In responding to requests to perform male circumcision, doctors should follow the guidance issued by professional organisations:
Circumcision may constitute significant harm to a child if the procedure was carried out in such a way that :
Significant harm is defined in Section 31 Children Act 1989 and is referred to in accordance with the statutory guidance Working Together to Safeguard Children. Where it is believed that a child has suffered, or is likely to suffer, significant harm, concerns should be shared with Children’s Social Care as a referral (see Referrals).
Harm may stem from clinical practice being incompetent (including lack of anaesthesia) and/or clinical equipment and facilities being inadequate, not hygienic, etc. The professionals most likely to become aware that a boy is at risk of, or has already suffered from, harm from circumcision are health professionals (GPs, health visitors, A&E staff or school nurses), and childminding, day care and teaching staff. Others with responsibilities or roles within the wider community may also become aware, e.g. members of faith groups or sports/voluntary groups.
If anyone becomes aware, through something a child discloses, or another means, that the child has been, or may be, harmed through male circumcision, a referral must be made to children’s social care.
Children’s social care should assess the degree of harm and determine whether the likely or actual harm is significant for the child in question. Possible risks for other children in the family (including unborn babies) should also be considered
Where a criminal offence is suspected, e.g. sexual abuse or unjustified deliberate injury, the police must also be notified.
If any professional considers that their concerns are not being responded to appropriately, the Escalation, Challenge and Conflict Resolution Procedure should be followed.
If concerns relate to a professional or other person in a position of trust, concerns must be discussed with the Local Authority Designated Officer (LADO).
Community and religious leaders should take a lead in the absence of approved professionals and develop safeguards in practice. This could include setting standards around hygiene, advocating and promoting the practice in a medically controlled environment and outlining best practice if complications arise during the procedures.
Multi-Agency Public Protection Arrangements (MAPPA) was introduced in 2001 as the statutory arrangements for managing sexual and violent offenders. It is a process through which the police, probation and prison services work together, with other agencies, to help reduce the re-offending behaviour of violent and sexual offenders living in the community, in order to protect the public.
The purpose of MAPPA is to ensure that comprehensive risk assessments are undertaken and robust risk-management plans put in place. MAPPA takes advantage of coordinated information-sharing across the agencies on each MAPPA offender, and ensures that appropriate resources are directed in a way which enhances public protection.
MAPPA is not a statutory body in itself but is a mechanism through which agencies can better discharge their statutory responsibilities and protect the public in a coordinated way.
The Responsible Authority is the primary agency for MAPPA. This is the police, prison and probation service in each area, working together. The Responsible Authority has a duty to ensure that the risks posed by specified sexual and violent offenders are assessed and managed appropriately.
Other bodies have a duty to cooperate with the Responsible Authority in this task. These duty to cooperate agencies (DTC agencies) will need to work with the Responsible Authority on particular aspects of an offender’s life, for example education, employment, housing, social care. These agencies include:
The first stages of the process are to identify offenders who may be liable to management under MAPPA as a consequence of their caution or conviction and sentence. This responsibility falls to the agency that has the leading statutory responsibility for each offender. Offenders are placed into one of four MAPPA categories according to their offence and sentence:
MAPPA offenders are managed at one of three levels according to the extent of agency involvement needed and the number of different agencies involved.
Level 1: ordinary agency management – ordinary agency management level 1 is where the risks posed by the offender can be managed by the agency responsible for the supervision or case management of the offender. The majority of offenders are managed at level 1. This involves the sharing of information but does not require multi-agency meetings.
Level 2: active multi-agency management – cases should be managed at level 2 where the offender:
Level 3: active enhanced multi-agency management – level 3 management should be used for cases that meet the criteria for level 2 but where it is determined that the management issues require senior representation from the Responsible Authority and DTC agencies. This may be when there is a perceived need to commit significant resources at short notice or where, although not assessed as high or very high risk of serious harm, there is a high likelihood of media scrutiny or public interest in the management of the case and there is a need to ensure that public confidence in the criminal justice system is maintained.
The vast majority of MAPPA offenders will be managed through the ordinary management of one agency, although this will usually involve the sharing of information with other relevant agencies.
The structural basis for the discussion of MAPPA offenders who need active interagency management, including their risk assessment and risk management, is the MAPP meeting.
The Responsible Authority agencies and the MAPPA Coordinator are permanent members of these meetings. The DTC agencies should be invited to attend for any offender in respect of whom they can provide additional support and management. The frequency of meetings depends on the level of management deemed appropriate for each offender.
RELEVANT INFORMATION
Prevent Duty Guidance (Home Office)
Prevent Duty Training (Home Office)
Channel duty guidance: protecting people susceptible to radicalisation (Home Office)
Radicalisation is the process through which people come to hold increasingly extreme views or beliefs that support terrorist groups or activities. The most common types of terrorism in the UK are extreme right-wing terrorism and Islamist terrorism. Multi-agency working is key to supporting children who have been radicalised, or who are at risk of radicalisation.
Extremism is defined as the promotion or advancement of an ideology or beliefs based on violence, hatred or intolerance that aims to:
(See Definition of Extremism, gov.uk)
Exposure to extremism can lead to radicalisation and acts of terrorism
The national counter-terrorism strategy, CONTEST aims to reduce risks of terrorism in the UK and overseas.
Prevent is one of the key parts of CONTEST and aims to stop people becoming terrorists or supporting terrorism; it focuses on early intervention and safeguarding. Prevent is run locally by specialist staff who understand the risks and issues in the local area and know how best to support their communities. Through working together, organisations can identify people who are at risk of radicalisation and provide them with support. The objectives of Prevent are to:
The Prevent duty (Section 26, Counter-Terrorism and Security Act 2015 (CTSA) requires frontline staff working in specific organisations – including education, health, local authorities, police, prisons and probation – to work together to help prevent the risk of people becoming terrorists or supporting terrorism. It helps to make sure that people who are being radicalised are supported in the same way as they are under safeguarding processes.
Children and young people can be exposed to the messages of extremist groups or drawn into violence in different ways, including through family members, by direct contact with extremist groups or, most often, the internet.
Everyone is different and there is no single way of identifying who is at risk of being radicalised into terrorism or supporting terrorism. Signs that a child or young person is being radicalised include them:
Any child can be radicalised but there are some factors which may make a young person more vulnerable. These include them:
These factors will not always lead to radicalisation.
Children are exposed to news and information in lots of different ways and and they may see things which worry them or make them angry. Professionals and parents and carers can help them understand world events and issues in the news by:
Children should be encouraged to consider other viewpoints and to check the facts behind the information that they are looking at. Radicalisers will use conspiracy theories and fake news to draw people in.
As most radicalisation takes place on-line, make sure that devices have the appropriate parental controls in place, and monitor screen time.
Staff working in frontline roles such as education will often be the first to notice if a child displays concerning behaviour. If staff notice behaviours that are a cause for concern, they should consider whether the child is at risk of radicalisation.
There could be many different reasons for the behaviours, not just radicalisation. It is important to understand the context and try to find out why these changes are happening, before reaching conclusions too quickly.
Concerns about radicalisation or extremism should then be checked / shared with the designated safeguarding lead in the organisation. The Prevent lead in the local authority or local police can also be contacted for advice.
Before deciding whether to make a referral to Prevent, it is important to gather as much information as possible, to assess if the child or young person may be on a pathway that could lead to terrorism.
The Department for Education has a dedicated telephone helpline for schools in England who have non-emergency concerns about extremism; which can be contacted by telephoning: 020 7340 7264.
Where there are concerns about radicalisation and extremism, relevant information should be shared with children’s social care (see Referrals chapter). A multi-agency meeting will be held to discuss whether to make a referral to the police for support under Prevent. Referrals to Prevent are made using the Prevent national referral form (see Get help for radicalisation concerns , gov.uk).
Children who could be referred include those who:
REMEMBER – in an emergency, always ring 999.
Once a referral is submitted to the local Prevent team, specialist police staff will assess it. Firstly, they will check if the child is an immediate security threat. The police will then check if there is a risk of radicalisation which means that the child should be discussed at the local Channel panel to see if they are eligible for support through Prevent. This is called a ‘gateway assessment’. Referrals into Channel are made by the Police. If the child needs other support, this should continue unless there is a good reason not to do so.
Channel panels are chaired by the local authority, and attended by multi-agency partners such as police, education professionals, health services, education and children’s social care. They meet to discuss the referral, assess the risk, and, if appropriate, agree a package of support specific to the individual child. Channel is a voluntary process, and the child’s parents and carers must give their consent before a child receives support.
The type of activities that are included in a support package will depend on risk factors, vulnerabilities, and local resources, but might include:
family support contact – activities aimed at supporting family and personal relationships, including formal parenting programmes;
Where Channel is not considered suitable for the child, or their parents or carers do not consent, alternative options will be explored. If the risks cannot be managed in Channel, they will be kept under review by the police.
Where the Channel panel decides to close a case, the child and their parents and carers should be told that their case is being closed and that they will no longer receive support through Channel. They should also be told that ongoing support they are receiving through mainstream services (such as from the NHS, children’s social care, youth justice services, education) will continue.
Identifying a lead professional at the point of the case being closed provides reassurance that they can be brought back for discussion at the panel quickly, should concerns about them re-emerge.
The panel is best placed to identify which agencies will continue to engage with the child after their case with Channel has been closed and to identify a lead professional. Frontline practitioners involved in providing continuing support must be informed that Channel no longer has oversight of the child, and advised on how to re-refer them to Prevent if there are any future concerns.
When sharing personal data about children and young people at risk of radicalisation, it is important to adhere to the requirements of data protection legislation.
Data protection legislation is not intended to prevent the sharing of personal data, but to make sure that it is done lawfully and with appropriate safeguards in place. Under the Data Protection Act and UK GDPR, there must be a legal basis to share personal data. The Prevent Duty is a lawful basis on which to share data.
See also Data Protection and Tier 1 – Children Safeguarding Data Sharing Agreement (DSA)
RELEVANT CHAPTER
Multi Agency Child Exploitation Protocol
RELEVANT INFORMATION
Brook – the young people’s sexual health and well-being charity
Relationships and sex education (RSE) and health education (Department for Education)
Harmful sexual behaviour among children and young people (NICE)
Instances of underage sexual activity may raise difficult issues for practitioners and need to be handled with sensitivity. Agencies should ensure that all children and young people are given appropriate protection from sexual abuse. It is the responsibility of all professionals to accurately assess any risk of harm, including significant harm, when a child or young person is engaged in sexual activity. This is likely to require a multi-agency approach.
This guidance has also been formed within the context of government policy and therefore supports the principle that young people should be able to access sexual and reproductive health services, including advice about contraception and abortion.
This guidance applies to all sexual relationships. It is designed to assist staff in identifying where sexual relationships may be abusive and whether a child or young person may need the provision of protection or additional services in relation to sexual activity.
Where there are indications of actual or risk of sexual abuse of a child/young person, be it child sexual exploitation, interfamilial abuse or peer-on-peer abuse, also see the Multi Agency Child Exploitation Protocol.
The sexual behaviour of young people is conceptualised as laying on a continuum from mutual exploration to behaviours that are seriously harmful to them or to other children or young people.
 Where sexual behaviour is harmful, please refer to the Harmful Sexual Behaviour chapter.
Where sexual behaviour is harmful, please refer to the Harmful Sexual Behaviour chapter.
It is essential for agencies to clarify the age of the young person, as this will dictate the course of action to be taken. The Sexual Offences Act 2003 sets out the law in relation to children and young people under the age of 18 years old:
A child under 13 is not legally capable of consenting to sexual activity. Any offence under the Sexual Offences Act 2003 involving a child under 13 is very serious and offences committed by an adult may result in a significant prison sentence.
Where a professional is concerned that a child under 13 is involved in penetrative sex, or other intimate sexual activity, there will always be reasonable cause to suspect that a child, whether a girl or boy, is suffering or is likely to suffer significant harm. Professionals should make a referral to Children’s Social Care (see Referrals chapter).
Children’s Social Care will convene a strategy meeting which should include the professional making the referral as well as representatives from Children’s Social Care, police and other relevant agencies.
Where both parties involved in sexual activity are under 13, then both children should be considered at risk of significant harm. Thames Valley Police will seek to avoid any prosecution of a child where the children are age appropriate and there is no evidence of coercion, threat, force or other power imbalance.
Sexual activity with a child under 16 is also a criminal offence. Where it is consensual it may carry a less serious criminal penalty than under 13 but still attracts a significant prison sentence. It may nevertheless have serious consequences for the welfare of the child.
Consent is always based on choice and is active, not passive. Consent is possible only when there is equal power. Forcing someone to give in is not consent, and going along with something because of wanting to fit in with a group is not consent: ‘If you can’t say “no” comfortably then “yes” has no meaning. If you are unwilling to accept “no” then “yes” has no meaning.’
Consideration should be given in every case of sexual activity involving a child aged 13–15 as to whether there should be a discussion with other agencies and whether a referral should be made to Children’s Social Care. Professionals should use the risk indicators outlined in Section 4 to inform their decision making.
Cases of concern should be discussed with the nominated child protection lead for the agency and subsequently with other agencies if required. Where confidentiality needs to be preserved, the initial consultation can occur without identifying the child directly or indirectly.
Where there is reasonable cause to suspect that significant harm to a child has/might occur, a referral must be made to Children’s Social Care and a strategy discussion held.
Thames Valley Police will seek to avoid any prosecution of a child where the children are age appropriate and there is no evidence of coercion, threat, force or other power imbalance.
Although in most cases sexual activity in itself is not an offence when the young person is over the age of 16, young people aged 16 and 17 are still vulnerable to harm through an abusive sexual relationship and are still offered the protection of child protection procedures.
Professionals should still bear in mind the considerations outlined in this guidance, and in particular should be alert to:
The Sexual Offences Act 2003 makes provision for young people aged under 16 years to be offered confidential professional advice on contraception, condoms, pregnancy and abortion.
It is good practice to follow the Fraser guidelines when discussing personal or sexual matters with a young person under the age of 16 (Lord Fraser, House of Lords ruling in case of Victoria Gillick v West Norfolk and Wisbech Health Authority & Department of Health and Social Security 1985). These hold that sexual health services can be offered without parental consent providing that:
This exception, in statute, covers not only health professionals, but also anyone who acts to protect a child, e.g. teachers, school nurses, careers service personal advisers, youth offending service officers, youth workers, social workers and parents.
In offering such advice, a person is not guilty of aiding, abetting or counselling a sexual offence against a child where they are acting for the purpose of:
Promoting emotional wellbeing includes exploring the part that sexuality plays in the young person’s sense of identity, the emotional implications of entering into a sexual relationship, and the characteristics of healthy relationships. Where appropriate, the needs and concerns of lesbian, gay, bisexual and transgender young people should be recognised and approached sympathetically. Professionals should consider the particular needs of young people with disabilities. Young people who have been abused may need specialist support, for example where sexual feelings are regarded as shameful or where past relationships have been violent or exploitative.
The duty of confidentiality owed to a person under 16 in any setting is the same as that owed to any other person, but the right to confidentiality is not absolute.
Where there is a serious child protection risk to the health, safety or welfare of a young person or others, this outweighs the young person’s right to privacy.
Research and experience have shown repeatedly that keeping children safe from harm requires professionals and others to share information. Such information sharing must be in accordance with legal requirements and the Information Sharing Protocol.
All young people, regardless of gender or sexual orientation, who are believed to be engaged in or planning to be engaged in, sexual activity must have their needs for health education, support and/or protection assessed by the agency/agencies involved.
Consideration should be given to how the young person can access associated assessments and support, and where necessary agencies should signpost or make a referral to appropriate provision.
On each occasion that a young person is seen by an agency, consideration should be given as to whether her/his circumstances have changed or further information has been given which may lead to the need for a referral or re-referral to Children’s Social Care
Where the child is considered to be suffering or likely to suffer significant harm a referral must be made to Children’s Social Care (see Referrals chapter).
In assessing the nature of any particular behaviour, it is essential to look at the facts of the relationship between those involved.
The following considerations must be taken into account when assessing the extent to which the child (or other children) may be suffering, or are at risk of suffering, harm (this list is not exhaustive):
It is important that all decision-making is undertaken with full professional consultation and never taken by one person alone. All discussions must be recorded, giving reasons for action taken and who was involved.
In cases of concern, where sufficient information is known about the sexual partner(s), the agency should check with other agencies, including the police, to establish what, if any, information is known about them. The police should normally share the required information without beginning a full investigation.
Where a serious crime is suspected, advice should be sought from the police at the earliest opportunity to safeguard the child and minimise the risk of any evidence, such as emails or pictures, being destroyed prior to an investigation.
Sexual abuse and exploitation of a child or young person involves an imbalance of power. Any assessment should seek to identify possible power imbalances within a relationship. These can result from differences in size, age, material wealth and/or psychological, social and physical development. In addition, gender, sexuality, race and levels of sexual knowledge can be used to exert power.
Where a power imbalance results in coercion, manipulation and/or bribery and seduction, these pressures can be applied to a young person by one or two individuals, or through peer pressure (i.e. group bullying). Professionals assessing the nature of a child or young person’s relationship need to be aware of the possibility that either or both of these situations can exist for the child or young person, and they should conduct a holistic assessment of the young person’s needs.
There will be an imbalance of power, and the child or young person will not be deemed able to give consent, if the sexual partner is in a position of trust or is a family member, as defined by the Sexual Offences Act 2003, and/or any pre-existing legislation.
Disabled children and young people are more likely to be abused than non-disabled children, and they are especially at risk when they are living away from home (see Children Living Away from Home). They may be particularly vulnerable to coercion due to physical dependency or because a learning disability or a communication difficulty means that it is not easy for them to communicate their wishes to another person. This increases the risk that a sexual relationship may not be consensual.
Professionals should not, however, assume that because a young person has a disability that they are not Fraser competent. Although there is a duty to protect from abuse and exploitation, professionals also need to recognise that disabled children have the right to a full life, including a sexual life.
A child or young person with a disability could be vulnerable to harm from a sexual relationship developed through inclusive activities. This may be in mainstream schools, education colleges, leisure centres and other places where children and young people meet where supervision is at a minimum. Staff need to be alert to the different capabilities of the children and young people they supervise, and assess risks accordingly.
Where professionals in Children’s Social Care have concerns that a relationship may present a risk of harm to an older disabled young person, they should begin work with the Adult Social Care services at an early point in order for there to be a smooth transition from protection under the Children Act 1989 to protection for the young person, from their 18th birthday onwards.
Doctors and other health professionals should consider the following issues when providing advice or treatment to young people on contraception, and sexual and reproductive health.
If a request for contraception is made, doctors and other health professionals should establish rapport and give a young person support and time to make an informed choice. It is important to take account of the capacity of a young person to make informed decisions, even if they are over 16 years old.
If a young person has a learning difficulty or disability, they should be encouraged to speak to an advocate of their choice to help their voice be clearly heard.
When considering a termination of pregnancy, it is particularly important to ensure that the young person has fully understood what is happening.
The following items should be discussed when providing advice or treatment to young people on contraception, and sexual and reproductive health:
Young people need to be able to talk to a trusted adult about sex and relationship issues. Although it is desirable that this person is their parent or carer, this is not always possible. The law allows staff to respect young people’s rights to confidentiality when discussing sex and relationship issues, and a disclosure of under-age sex is not of itself a reason to break confidentiality.
Young people should be made aware that confidentiality might be breached if they or another young person is at risk. In these circumstances staff should consult the young person and endeavour to gain their cooperation to a child protection referral. If that is not possible, they should be advised that their confidentiality would be breached.
Staff in schools should consider the need to establish links with colleagues in health to facilitate the delivery of advice/support and guidance on matters of sexual health.
While police and Children’s Social Care staff may provide advice and guidance to a young person involved in under-age sexual activity, both agencies have specific responsibilities with regard to criminal activities.
Children’s Social Care staff should inform police of actual and suspected criminal offences at the earliest possible opportunity in order to consider jointly how to proceed in the best interests of the child. Any decisions not to do so must be made at a senior level and recorded on the child’s file.
Guidance for Children’s Social Care staff indicates that, as Working Together is issued under Section 7 of the Local Authority Social Services Act 1970, a decision not to inform the police where an offence has been committed against a child should only be made where ‘exceptional circumstances justify a variation’ (LASSL (2004) 21). This is likely to be where the sexual relationship is considered consensual and not abusive, and may be most relevant in respect of children in care where children’s social care is also acting as the ‘corporate parent’ for the child.
In these circumstances it may be more important that the child receives appropriate advice regarding sexual health and contraception. This may be difficult if the young person is concerned that the police will be involved. Such a decision should always be made following consultation with line managers and should be recorded.
The police will proportionately investigate all criminal activities and make appropriate decisions in relation to the need for prosecution or not. Such decisions should always be made following consultation with line managers and should be recorded.
The priority for the police is the identification and investigation of under-age sexual activity where the relationship is abusive, either by being intra-familial in nature, or where there is a significant age/power gap between the parties involved.
Where young people of a similar age are involved in consensual sexual activity, or in other sensitive cases, the police role may be confined to the undertaking of information checks only. In such cases the police will not become directly involved in an investigation unless enquiries by the police or other agencies indicate the relationship is in fact abusive.
Both police and Children’s Social Care staff together may decide that there is no need for prosecution, but young people should be advised that their confidentiality cannot be maintained if staff from these agencies are involved.
Decisions to share information with parents and carers should be taken using professional judgement, consideration of the Fraser guidelines and in consultation with the child protection procedures. Decisions should be based on the child’s age, maturity and ability to appreciate what is involved in terms of the implications and risks to themselves. This should be coupled with the parents’ and carers’ ability and commitment to protect the young person.
Given the responsibility that parents have for the conduct and welfare of their children, professionals should encourage the young person, at all points, to share information with their parents and carers wherever safe to do so.
Those working directly with young people should give consideration to the role they may have in facilitating information sharing with parents/carers, in a planned way, in partnership with the young person.
RELATED GUIDANCE
Parents with Alcohol and Drug Problems: Adult Treatment and Family Services (gov.uk) – a toolkit containing guidance, data and other resources to support professionals who are helping families affected by parental alcohol and drug problems.
Government guidance uses ‘parents with problem alcohol and drug use’ to refer to parents or carers of children whose alcohol or drug use causes, or has the potential to cause, harm to children. Dependent and non-dependent problematic use are both included in this definition.
Not all children of parents who use alcohol or drugs problematically will experience significant harm, but children growing up in these families are at a greater risk of adverse outcomes.
Research shows that problem alcohol and drug use can reduce parenting capacity and is a major factor in cases of child maltreatment. Department for Education (DfE) research on the characteristics of children in need has found parents using drugs to be a factor in around 17% of child in need cases, and parental alcohol use to be a factor in 16%. DfE analysis of serious case reviews also found that parental alcohol or drug use was recorded in over a third (36%) of reviews carried out when a child has died or been seriously harmed.
Families affected by parental alcohol and drug use typically have multiple support needs. In addition to alcohol and drug use, their support needs often include:
Parents’ dependent alcohol and drug use can negatively impact on children’s physical and emotional wellbeing, their development and their safety. The impacts on children include:
The harms children experience can cause problems in the short term and later in life. Evidence shows that this includes intergenerational patterns of:
Families affected by parental alcohol and drug use may need significant support to address the long-term effects of stigma and exclusion. Children and parents may need support and encouragement to get the courage to ask for and accept help and to talk openly about issues in the family.
Guidance – Parents with Alcohol and Drug Problems: Adult Treatment and Family Services (gov.uk) lists examples of how to overcome barriers to engagement:
There is consistent evidence of an association between parental alcohol and drug use and conflict. Parental conflict is defined in government guidance as ‘conflicts that occur between parents or carers that are frequent, intense and poorly resolved’. So, parental conflict can include a range of behaviours that fall short of domestic abuse.
Where parental alcohol and drug use and conflict coexist, the risk of poor outcomes for children is greater than when either is experienced alone. The nature of these outcomes derive from internalising (for example, anxiety and depression) and externalising (for example, aggression and hostility) behaviour. These are the same outcomes as for children who experience either parental substance misuse or conflict in isolation.
Few interventions exist to address parental substance misuse and conflict. But treatment services that integrate interventions to reduce parental conflict into the support they offer report that addressing the two problems together is effective at:
Effective safeguarding work between practitioners depends on collaborative working between all relevant local agencies, and that they recognise that no single professional has all of the required knowledge or skills for this work. This should include multi-agency training and evaluating and sharing good practice between agencies.
Adult and family services should be alert to potential problem alcohol and drug use by parents who they are providing help and support to. Staff in these services should understand the potential impact of problem alcohol and drug use on children and how that combines with other risk factors. Staff should also be clear what support their own service might be able to offer as well as what local pathways exist, so they can identify, assess and refer parents and affected children.
Guidance – Parents with Alcohol and Drug Problems: Adult Treatment and Family Services (gov.uk) recommends that alcohol and drugs services should have a ‘designated practitioner’ or ‘dedicated and named practitioner’ to:
Appropriate and timely information sharing between local partner agencies is essential to identify and support families.
Drug and alcohol treatment providers should (where relevant) ask adults who use their service if they or their partner are pregnant. Where they are known to have a child living with them (or may have a child live with them in the future), practitioners should make suitable enquiries as to the welfare of the children and share information with children’s social care and other agencies as appropriate.
The statutory guidance Working Together to Safeguard Children sets out the following principles in relation to information sharing:
For further information see Tier 1 – Children Safeguarding Data Sharing Agreement (DSA) and Data Protection chapters.
There should be a focus on early help and prevention for families affected by parental alcohol and drug use. This means providing support as soon as signs of a problem emerge, at any point in a child’s life or pre-birth. This relies on organisations working together to identify children and families who might benefit from early help, undertaking an assessment of need and providing targeted early help services to children and their families with a focus on improving outcomes for children. Support can come from a wide range of statutory, health and community services according to the level of need assessed. See also Early Help chapter.
Where there is a low level of assessed need, alcohol and drug treatment services should use referral pathways to local agencies and organisations which provide universal and targeted help to parents with alcohol and drug problems, and their children.
Local alcohol and drug treatment services can take steps to help prevent later harmful consequences for parents and children, including:
When alcohol and drug treatment and children and family services are considering the impact of parental alcohol and drug use on a child, they should jointly assess families using tools and guidance which factor in all the relevant information.
Collaborative assessment, information sharing and clear pathways between systems and services are vital to identifying families affected by drug and alcohol problems and ensuring they receive appropriate support early.
This can be strengthened locally by:
NICE Clinical Guideline ‘Pregnancy and Complex Social Factors: A Model for Service Provision for Pregnant Women with Complex Social Factors’ sets out that where a pregnant woman has substance misuse issues, antenatal services should work with local agencies, including social care and substance misuse services, to coordinate antenatal care by, for example:
The woman should be offered a named midwife or doctor who has specialised knowledge of, and experience in, the care of women who misuse substances, and provided with a direct line telephone number for the named midwife or doctor.
She should also be provided with information about the potential effects of substance misuse on her unborn baby, and what to expect when the baby is born, for example what medical care the baby may need and where the baby will be cared for.
Where a practitioner has concerns about a risk of significant harm to a child (including unborn children), they should make a referral to children’s social care (see Referrals chapter). If there is an imminent threat of serious harm, the police should be called and action taken to safeguard the child (see Immediate Protection chapter).
Substance misuse practitioners working with parents should be involved in, and provide relevant information to, processes and interventions such as early help, children in need and child protection enquiries, including attendance at strategy discussions and child protection conferences. Plans for parents and children should incorporate input from all relevant practitioners. See also Assessments chapter.
Assessment should take into account:
All practitioners working with parents / carers with substance misuse issues must maintain a focus on their children’s wellbeing and the parents’ ability to adequately care for and protect their children. They should monitor and review children’s progress throughout the period of intervention and respond appropriately to any change in the circumstances of the parents and / or the child.
Where parents are to be discharged from substance misuse services, practitioners must consider the potential impact for children and engage with children’s social care colleagues as appropriate. If the situation deteriorates such that a practitioner considers there to be a risk of significant harm to the child, a referral should be made to children’s social care.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
The Prison Service will make a child safeguarding enquiry with children’s social care for all newly sentenced prisoners, and will identify prisoners who present an ongoing risk to children from within custody. Prisons will also decide on the level of contact, if any, they will allow between a prisoner and a child based on a child contact risk assessment. A prisoner’s contact with a child will be prohibited or restricted where necessary.
When a child safeguarding enquiry is received from a prison, children’s social care should:
The Probation Service will:
Information exchange between probation and children’s social care help both agencies develop a better understanding of the children and families they work with and ensures risk assessments are accurate and well informed.
Under the UK GDPR and Data Protection Act 2018 sharing an offender’s personal information must be lawful and fair and must comply with Part 3 of the Data Protection Act 2018 and in particular the data protection principles.
See also Tier 1 – Children Safeguarding Data Sharing Agreement (DSA) and Data Protection.
Sharing of information for the purposes of law enforcement and keeping children and young people safe meets one of the requirements for lawful processing under the Data Protection Act 2018, as the data sharing is authorised by law (under section 325(3) and (4) of the Criminal Justice Act 2003) (or section 14 of the Offender Management Act 2007). It is therefore not necessary for Prison and Probation Service staff to obtain consent from the offender under the Data Protection Act 2018.
For information exchange to be effective, children’s social care should:
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
Any assessment of children in secure youth establishments should take account of their specific needs. In all cases, the responsibility for the welfare and safety of a child is located jointly with the home and host local authority. Any professional conduct issues should be dealt with by the local authority in which the establishment is located. Partners should work with the secure youth establishment and, where appropriate, the Youth Custody Service to ensure that the child has a single, comprehensive support plan.
Where a child becomes looked after, as a result of being remanded to youth detention accommodation (YDA), the local authority should visit the child and assess the child’s needs before taking a decision on how they should be supported. This information should be used to prepare the care plan, which should set out how the YDA and other practitioners will meet the child’s needs whilst the child remains remanded, and at any point of transition they will experience (either returning to the community or upon receiving a custodial sentence). The care plan must be reviewed in the same way as a care plan for any other looked after child.
RELEVANT GUIDANCE
Modern Slavery: statutory guidance for England and Wales (Home Office)
Safeguarding children who may have been trafficked (Department for Education and Home Office)
This chapter should be read in conjunction with the following government guidance: Care of unaccompanied migrant children and child victims of modern slavery: statutory guidance for local authorities (Department for Education) which sets out the steps which local authorities should take to plan for the provision of support for Looked After Children / Children in Care who are unaccompanied asylum seeking children, unaccompanied migrant children or child victims of modern slavery including trafficking. Elements of the guidance will also be relevant for the care of Looked After Children who are UK nationals and who may also be child victims of modern slavery.
The cohort of unaccompanied migrant children and child victims of modern slavery includes a wide range of children in a variety of circumstances that a local authority will need to be aware of in order to ensure that the child receives appropriate legal advice and support. Some will have been trafficked or persecuted and may have witnessed, or been subject to, horrific acts of violence. Other migrant children may have been sent to the UK in search of a better life, or may have been brought here for a private fostering arrangement and subsequently exploited or abandoned when the arrangement fails.
There are a wide range of status possibilities for migrant children that the local authority will need to be aware of. In brief, the following categories regarding status are the most likely to be encountered. However this list is not exhaustive and legal advice should be sought wherever there is uncertainty about a migrant child’s status.
Categories of unaccompanied children include:
Where it is established that a referral concerns a young unaccompanied child migrant, regardless of the category, this will always satisfy the criteria for services as a Child in Need.
An unaccompanied child will become a Looked After Child, after they have accommodated by the local authority under Section 20(1) of the Children Act 1989 for 24 hours. Once accommodated, they will be subject to the appropriate regulations and the same provision as any other Looked After Child.
The local authority should record any modern slavery concerns on the child’s care plan.
As part of the general duty to assess and meet the needs of an Unaccompanied Asylum Seeking Child, the local authority should ensure that the child has access to a legal representative.
Unaccompanied children are highly likely to require specialist support from a variety of organisations and agencies (see for example, the Independent Unaccompanied Asylum-Seeking Children Support Service (IUSS) provided by the Refugee Council).
All professionals involved in the care of unaccompanied children and child victims of modern slavery should be able to recognise indicators of trafficking, slavery, servitude and forced or compulsory labour and should have an understanding of the particular issues likely to be faced by these children.
This is a highly complex area of work, and professionals will need to have available to them a solid understanding of the asylum process or colleagues or other professionals with such expertise.
The kinds of issues that may need to be negotiated include:
For more information, see Processing children’s asylum claims (UK Visas and Immigration).
Social workers should also have a broad understanding of the immigration system – for example, the immigration application process, different types of leave, making further leave to remain applications and the appeals process. Social workers should also have an understanding of the trafficking referral process and the wider safeguarding system around child victims of modern slavery, including how and when to refer a child to the National Referral Mechanism (NRM).
Legal advice can only be provided by a registered immigration advisor, ideally one with expertise in working with children. Legal Aid is available for asylum cases and Looked After Children will generally be eligible.
Independent Reviewing Officers (IRO) should consider the child’s needs as an unaccompanied child or child victim of modern slavery, including trafficking, when planning and providing care. They should also have an awareness of the particular needs and issues children may face as a result of being an unaccompanied child or child victim of modern slavery so that they can provide appropriate challenge at review.
Service providers should ensure that foster carers and all other care staff in placement settings are aware of appropriate steps to reduce the risk of trafficked children returning to their traffickers.
Social workers should consider all unaccompanied migrant children as potential victims of modern slavery in the first instance until this possibility is either confirmed or discounted and they should also have an understanding of the trafficking referral process under the National Referral Mechanism.
The social worker must ensure that all unaccompanied children have access to specialist asylum and/or immigration legal advice and representation in their assessment so as to ensure the child can fully present their case for asylum or leave to remain.
The assessment will take account of:
Unaccompanied migrant children and child victims of modern slavery will need access to specialist legal advice and support. This will be in relation to immigration and asylum applications, and decisions and any associated legal proceedings. If they have been a victim of modern slavery, they will also need support in relation to criminal proceedings or compensation claims. The assessment should note that specialist legal support is required and how it will be provided. The child’s social worker should ensure that they are accompanied in all meetings, including meetings with legal professionals. The person accompanying the child does not have to be the child’s social worker.
In determining an unaccompanied young person’s accommodation needs, the assessment must have regard to their age and independent living skills and consider the intensity of service required. This may range between independent accommodation, semi-independent accommodation foster or residential placements, or in specific cases, a specialist residential therapeutic unit.
No assumptions should be made about the child’s language skills. An appropriately qualified and vetted interpreter must be used to assist in all assessments (see Interpreting, Signing and Communication Needs).
When completing cases records, it is important to pay particular attention to the detail of spelling names and of descriptions of family relationships.
Planning for the child should include planning for a variety of possible outcomes regarding the child’s immigration status – see Section 10, Asylum Process – Possible Outcomes.
Where the age of the child is uncertain and there are reasons to believe they are a child, they will be presumed to be a child in order to receive immediate assistance, support and protection in accordance with Section 51 Modern Slavery Act 2015. Assessments must be undertaken in accordance with standards established in case law and should only be carried out where there is reason to doubt that the child is the age they claim. For further guidance see: Age Assessment Guidance published by ADCS. In all cases where a referral is received concerning an unaccompanied child, the relevant Team will carry out an assessment in accordance with the Assessment Procedure, to determine whether they are a Child in Need.
Young unaccompanied child migrants should be provided with information about the services available to them from the local authority and other agencies.
The young person will also be given assistance to register with a GP and dentist, and enrol in a local school or college. The health professionals and the school should be aware of the child’s status and senior managers such as the Virtual School Head should be informed of the school placement. There will be a need to set out clearly any particular implications of the child’s status for non-specialist professionals such as GPs and teachers, including any urgency of involvement – particularly with health practitioners. An interpreter should be booked to accompany the young person to appointments with the GP or school, where necessary.
Where a young person’s needs are for independent or semi-independent accommodation, and the manager agrees, assistance should be given with completion of the necessary Housing Application.
Where the assessment identifies that an unaccompanied young child migrant needs to be Looked After, all the procedures in relation to Care Plans, Health Care Plans, Personal Education Plans and Placement Plans must be completed (see Decision to Look After, Buckinghamshire Children’s Social Care Procedures).
For unaccompanied migrant children who are Looked After, the placement decision will also need to be informed by careful consideration of the wider support needs of the child, including their cultural and social needs. It may be that the accommodation setting or carers cannot meet those needs on their own so other more creative ways, such as mentors or links to diaspora groups, could be used. As with all Looked After Children, an unaccompanied child’s ethnicity, cultural and linguistic background should be taken into account when placing the child with foster carers. However, these are not overriding considerations and should be taken into account alongside all of the child’s needs. Nevertheless, the placement should meet the child’s needs as a whole and be consistent with their wishes and feelings.
Where there are safeguarding concerns relating to the care and welfare of any unaccompanied child, including where modern slavery is suspected or has been identified, these should be investigated in line with the statutory provisions contained in Working Together to Safeguard Children. The opportunity to intervene to prevent any further exploitation might be very narrow, so the entry local authority should convene a Strategy Meeting/Discussion as soon as possible and take any necessary immediate action to safeguard and promote the child’s welfare. This Strategy Meeting/Discussion should involve the police, Immigration officials and any other relevant agencies and plan rapid further action if concerns are substantiated.
Provision may need to be made for the child to be in a safe place before any further assessment takes place and for the possibility that they may not be able to disclose full information about their circumstances immediately. The location of the child should not be divulged to any enquirers until their identity and relationship with the child have been established and the local authority is assured of their motives, if necessary, with the help of police and Immigration officials. The installation of police installed alarms should be considered and the child or young person advised about the safe use of mobile phones, so they cannot be traced etc.
All unaccompanied young asylum-seekers who are eligible for a service will be entitled to financial assistance which must first be authorised by the manager. The social worker should arrange for payment of the relevant amounts in accordance with the local authority procedures.
Travel cards or warrants will be issued to young unaccompanied asylum-seekers in relation to appointments at the Home Office.
Where an assessment identifies that an unaccompanied child migrant does not meet the criteria for a service from Children’s Social care but appears to be in need of services from elsewhere, the social worker will refer the young person to the appropriate agency which may be a different local authority Children’s Social Care department, the Refugee Council, UK Visas and Immigration and/or an appropriate voluntary agency.
In such circumstances, the duty social worker should make an appointment for the young person and advise them of the name, address (including a map where necessary) and contact number of the person with whom the appointment has been made. In addition, the duty worker must send a copy of the referral and assessment to the relevant office.
In all cases where a service is to be refused, the social worker must consult their manager before the decision is made and the letter confirming the decision is sent. Any correspondence received in relation to the decision should be referred to the manager.
The provision of a service is dependent on the young person continuing to qualify for the service.
Services to an unaccompanied child migrant may be withdrawn, for example, where another adult wishes to assume Parental Responsibility and this is assessed as appropriate.
The service must not be withdrawn without a Child in Need Plan Review (see Child in Need Plans and Reviews Procedure, Buckinghamshire Children’s Services) and the agreement of the social worker’s manager. Any such decision must be clearly recorded, with reasons. In all such cases, legal advice should usually be obtained before a final decision is made.
Where a service is withdrawn, the social worker should inform the Finance Office, if appropriate, immediately.
Planning transition to adulthood for unaccompanied children is a particularly complex process that needs to address their developing care needs in the context of their immigration status.
Pathway Planning to support an unaccompanied child’s transition to adulthood must cover the areas that would be addressed within any care leaver’s plan as well as any additional needs arising from their immigration status and the action required to resolve this. (See Leaving Care and Transition Procedure, Buckinghamshire Children’s Services.)
Former unaccompanied children who qualify as care leavers and who have been granted leave to remain, or who have an outstanding asylum or other human rights claim or appeal, are entitled to the same level of care and support from the local authority as any other care leaver.
The extent of any care leaver duties on local authorities to provide support to former unaccompanied children who have turned 18, exhausted their appeal rights, established no lawful basis to remain in the UK and should return to their home country is subject to a Human Rights Assessment by the local authority. This is set out under the restrictions on local authority support for adults without immigration status.
For former unaccompanied children whose long-term future is in the UK, transition planning will need to consider the challenges and issues facing any care leaver, such as education or preparing for independent living. Planning for children and young adults who have been granted refugee status or humanitarian protection should also consider when they may be required to make a further application for leave to remain.
Where an unaccompanied child or child victim of modern slavery qualifies for local authority care leaving support, a personal adviser must be appointed to support them.
Pathway plans should always consider and reflect the implications for the child or young adult if their asylum claim is refused without a grant of leave, if their application to extend their leave is refused or if their appeal against a refusal is dismissed. In such circumstances, the person will become unlawfully present in the UK and be expected to make plans for a return to their home country. A plan for a return to their home country may also need to be made at any other point, should the care leaver decide to leave the UK.
Planning may have to be based around short-term achievable goals whilst entitlement to remain in the UK is being determined. For the majority of unaccompanied children who do not have permanent immigration status, transition planning should initially take a dual or triple planning perspective, which, over time should be refined as the young person’s immigration status is resolved.
Planning cannot pre-empt the outcome of any immigration decision and may be based on:
Assistance should be given in advance of their 18th birthday with the necessary applications for housing, Housing Benefit and any other relevant benefits. The social worker must ensure that the young person has accommodation to which to move on their 18th birthday. The provider of the young person’s present accommodation and the Finance Office should be informed when the accommodation arrangement will end.
Financial support for care leavers who are former unaccompanied child migrants should reflect their needs and their immigration status. Financial policies should highlight any entitlements and how their immigration status may affect these. Pathway plans should address employment opportunities and funding arrangements for education and training, taking account of the young person’s immigration status.
If a young person has No Recourse to Public Funds (NRPF), they will be unable to access a number of welfare benefits and social housing. Subject to the Human Rights Assessment by the Local Authority under Schedule 3 Nationality, Immigration and Asylum Act 2002 (as amended), the provision of accommodation may form part of the Leaving Care support provided to a young person who has NRPF. For further information please go to Families with No Recourse to Public Funds Procedure, Buckinghamshire Children’s Services.
Having NRPF does not prevent a person from accessing other publicly funded services, but many of these will have eligibility criteria based on immigration status which will need to be considered. (See NRPF Network – What are public funds?)
Where a young person is Looked After, their circumstances will be reviewed in accordance with the Looked After Reviews Procedure.
Any other services provided should be reviewed at least every 6 months as set out in the Child in Need Plans and Reviews Procedure.
In advance of each review, the social worker will send the young person a checklist setting out the documents which are required to be produced at the Review, such as confirmation of registration with a GP, enrolment at schools/college and updated information concerning their asylum status.
The young person should be invited to the Review and an interpreter should be booked as necessary.
Independent Reviewing Officers (IRO) should have regard to the child’s needs as an unaccompanied child or child victim of modern slavery, including trafficking, when planning and providing care. They should also have an awareness of the particular needs and issues children may face as a result of being an unaccompanied child or child victim of modern slavery so that they can provide appropriate challenge at review. Service providers should ensure that foster carers and all other care staff in placement settings are aware of appropriate steps to reduce the risk of trafficked children returning to their traffickers.
Guidance for cases where the child has been the subject of sexual exploitation can be found in the Multi Agency Child Exploitation Protocol.
Where a Review confirms the service, the Financial Assessment Form should be updated. Where additional support services are identified as necessary, the Plan should be updated to reflect this.
Where services are withdrawn as a result of the Review, the relevant teams should be notified immediately.
There are four main possible outcomes of the asylum process for an unaccompanied child, which will determine what the long term solution might be:
Granted refugee status (i.e. granted asylum), with limited leave to remain for five years, after which time they can normally apply for settlement (i.e. indefinite leave to remain);
Refused asylum but granted humanitarian protection, with limited leave to remain for five years, after which time they can normally apply for settlement (i.e. indefinite leave to remain). This is most commonly granted where the person is at risk of a form of ‘ill treatment’ in their country of origin but which does not meet the criteria of the Refugee Convention. As it is very likely that those granted refugee status or humanitarian protection will qualify for indefinite leave to remain, their care and pathway planning should primarily focus on their long-term future in the UK, in the same way as for any other Care Leaver;
Refused asylum but granted Unaccompanied Asylum Seeking Child (UASC) Leave. This is normally for 30 months or until the age of 17½, whichever is the shorter period. This form of leave is granted to unaccompanied children where they do not qualify for refugee status or humanitarian protection, but where the Home Office cannot return them to their home country because it is not satisfied that safe and adequate reception arrangements are in place in that country. It is a form of temporary leave to remain and is not a route to settlement. It is important to note that this decision is a refusal of the child’s asylum claim and will attract a right of appeal. The child should be assisted to obtain legal advice on appealing against such a refusal. Before the child’s UASC Leave expires, they can submit an application for further leave to remain and/or a fresh claim for asylum, which will be considered. It is essential that they are assisted to access legal advice and make any such further application or claim before their UASC Leave expires. In such cases, care and pathway planning should therefore consider the possibility that the child may have to return to their home country once their UASC Leave expires or that they may become legally resident in the UK long-term (if a subsequent application or appeal is successful). Planning should also cover the possibility that they reach the age of 18 with an outstanding application or appeal and are entitled to remain in the UK until its outcome is known;
Refused asylum and granted no leave to remain. In this case the unaccompanied child is expected to return to their home country and their care plan should address the relevant actions and the support required. The Home Office will not return an unaccompanied child to their home country unless it is satisfied that safe and adequate reception arrangements are in place in that country. Any appeal or further application should be submitted where appropriate by the child’s legal adviser.
Although the above are the four main types of outcomes for an unaccompanied child, there may be others. For example, a child may be granted discretionary leave depending on whether they meet other criteria such as needing to stay in the UK to help police with their enquires after being conclusively identified as a victim of trafficking. Other examples include: leave as a stateless person; limited or discretionary leave for compassionate reasons; and limited leave on the basis of family or private life.
Local Government Association – Council Support: Refugees, Asylum Seekers and Unaccompanied Children – resource for council staff, designed to answer questions about supporting refugees, asylum seekers and unaccompanied children.
National Referral Mechanism: Guidance for Child First Responders – provides details on how to refer a child into the NRM and complete the referral form, reviews of decisions and the benefits of referral.
Guidance on Processing Children’s Asylum Claims – Case worker guidance – sets out the process which immigration officials follow in determining an asylum claim from a child and the possible outcomes for the child
Modern Slavery and Exploitation Helpline (Unseen)
National Transfer Protocol for Unaccompanied Asylum Seeking Children – interim national transfer procedure and transfer flow chart for the safe transfer of UASC from one UK Local Authority to another.
Child Protection: Working with Foreign Authorities (Department for Education) – guidance on child protection cases and care orders where the child has links to a foreign country
Modern Slavery: How to identify and support victims (Home Office)
RELEVANT CHAPTERS
Safer Recruitment and Employment
See also: Buckinghamshire Safeguarding Children Partnership website for information on how to book multi agency safeguarding children training
Buckingham Safeguarding Children Partnership (BSCP) provides multi agency training for staff and volunteers on the local safeguarding children policies and procedures. Training is provided at different levels, to reflect the different roles and responsibilities staff may have in relation to safeguarding arrangements. Employers, student bodies and voluntary organisations should also ensure training is provided to all relevant staff members to reflect the role they have in safeguarding children and promoting their welfare. This should include:
Training should take place at all levels in an organisation and be updated regularly to reflect best practice. To ensure that practice is consistent – no staff group should be excluded.
Training is an ongoing responsibility and should be provided as a rolling programme. Whilst training may be undertaken on a joint basis and BSCP has an overview of standards and content, it is the responsibility of each organisation to train its own staff.
Regular face to face supervision from skilled managers and reflective practice is also essential to enable staff to work confidently and competently with difficult and sensitive situations.
RELEVANT INFORMATION
Speak Up – free, independent, confidential advice on the speaking up process
Whistleblowing, or raising a concern, is where a worker (an employee, former employee, trainee, volunteer, agency worker or member of an organisation) reports a wrongdoing to their employer or another relevant organisation. Any wrongdoing reported in this way must be in the public interest. This means it must affect others, for example the general public.
Such wrongdoing may relate to:
There is a difference between a member of staff raising a concern / whistleblowing and making a complaint or grievance. A grievance or private complaint is about a person’s own employment position, and there is no public interest element in this. For example, a worker may raise a grievance against a colleague for breaching their confidentiality. Organisations will have a specific grievance procedure to cover such situations. This is not whistleblowing.
People outside the employing organisation, such as children and families or members of the public can also make complaints about staff or services. They can do so by making a complaint to the organisation using their complaints procedure, or something to another body such as Ofsted for example (see Section 2.1 How to raise a concern). This is not whistleblowing.
Any concerns relating to a child who is experiencing or at risk of abuse or neglect must be reported as a safeguarding concern. This is not whistleblowing.
Legal protections for whistleblowers mean no one acting in good faith when raising a concern will be penalised for doing so (see Section 4, Protection and Support for Whistleblowers). Any attempt to victimise employees for raising genuine concerns or attempts to prevent such concerns being raised should be regarded as a disciplinary matter.
However, knowingly and intentionally raising malicious, unfounded allegations should also be regarded as a disciplinary matter.
Whistleblowing does not:
A worker can blow the whistle to their employer following the guidance in their local whistleblowing policy or a ‘prescribed person or body’. Employers should investigate concerns reported to them thoroughly, promptly and confidentially. The person who has raised the concern should be told how the concern will be dealt with and provided with a timescale for a response.
A prescribed person or body provides staff with a way to raise their concern with an independent body when they do not feel able to disclose directly to their employer. When reporting concerns to a prescribed body, it must be the one which deals with the type of issue being raised, for example a concern about possible wrongdoing in a children’s home should be made to Ofsted. See Whistleblowing: list of prescribed people and bodies (gov.uk) for further information.
Workers can also report concerns to a third party such as a professional body or a member of the press. This is known as a ‘wider disclosure’. This type of disclosure must meet tougher tests in order for it to be protected, than a disclosure made to an employer or prescribed person or body.
Concerns can be raised anonymously, but the employer or prescribed body may not be able to take the concern further if they have not been provided with all the information they need.
Whistleblowers can give their name but request confidentiality – in this situation, the person or body you tell should make every effort to protect the person’s identity.
This will depend largely on the nature of the concerns raised; the most likely outcome is that the concern will be investigated by staff within the organisation.
Where appropriate, concerns that are raised may:
Where possible, within 10 working days, the member of staff raising the concern should receive in writing:
If, during the investigation, the staff member is concerned about what progress is being made, requires support or reassurance, or feels they may be being victimised or harassed as a result of making the disclosure, they should raise this with the designated contact / supporting organisation.
The designated contact should inform the staff member in writing of the outcome of their concern. However, this will not include details of any disciplinary action that may result, as this will remain confidential to the individual/s concerned.
Please note: due to the likely sensitive nature of raising concerns at work, the member of staff should discuss the matter with as few people as possible.
If the member of staff does not agree with the way their concerns have been dealt with by local management, they may choose to escalate their concerns to senior management.
The staff member may otherwise feel it necessary to report their concerns to an external body, however this must be appropriate for the issue concerned. See Appendix 2, Useful Organisations for a list of prescribed persons.
A record of concerns raised together with a record of action taken in response should be provided to the staff member who raised the concern.
The Public Interest Disclosure Act 1998 provides legal protection against detriment for workers who raise concerns in the public interest.
Bullying, harassment or victimisation (including informal pressures) by other members of staff towards someone who raises a concern will not be tolerated.
Senior management should be vigilant and may need to take appropriate action to protect staff who raise a concern in good faith.
Staff must not threaten or take retaliatory action against whistleblowers. Anyone involved in such conduct will be subject to disciplinary procedures.
If a staff member believes they have suffered any such treatment, they should inform their manager – or suitable other person – immediately. If the matter is not remedied they should raise it formally through the organisation’s grievance procedure.
Whistleblowing: list of prescribed people and bodies – contains a list of the prescribed persons and bodies.
Protect; Speak up, Stop harm – a UK Whistleblowing charity which provides free independent legal advice to staff and others who wish to raise concerns about the workplace.
Speak Up – Whistleblowing Helpline
Who is this Guidance for?
This practice guidance should be read by local Safeguarding Partners, and all agencies involved in the Multi-Agency Safeguarding Arrangements. The guidance is particularly aimed at those involved in undertaking or contributing to Local Child Safeguarding Practice Reviews (LCSPRs), such as Reviewers, Case Review Panel members, those providing information reports on behalf of their agency/organisation as well as those responsible for quality assuring and embedding the learning from the review process.
About this Guidance
This guidance provides Buckinghamshire Children Partnership Multi-Agency Safeguarding Arrangements with a framework for the commissioning and dissemination of learning from Local Child Safeguarding Practice Reviews. It should be read alongside the statutory guidance Working Together to Safeguard Children 2023.
The Children and Social Work Act 2017 introduced a legal framework in respect of local safeguarding arrangements for children. Responsibility for how a system learns lessons from serious child safeguarding incidents rests at a national level with the Child Safeguarding Practice Review Panel and at a local level with the three Safeguarding Partners (Integrated Care Boards, Police and Local Authorities) and other partner agencies. They will need to consider whether to conduct a Local Child Safeguarding Practice Review in cases where abuse or neglect of a child is known or suspected, and the child has died or been seriously harmed.
This guidance outlines the process for deciding on and commissioning Local Child Safeguarding Practice Reviews in Buckinghamshire. This makes real the local commitment to an improving and learning system, determined to make best use of resources (human and financial) in the best interests of children and families.
This guidance provides practitioners with a step-by-step guide to follow when undertaking or participating in a Local Child Safeguarding Practice Review. It describes the approach, order of events and related timescales whilst also highlighting the key statutory elements outlined in Working Together to Safeguard Children 2023. It also outlines responsibilities for key people at every stage of the process and references template documents and letters available for use.
The purpose of a Local Child Safeguarding Practice Review is to explore how practice can be improved through changes to the system itself. Reviews should seek to understand both why mistakes were made and to comprehend whether mistakes made on one case frequently happen elsewhere and to understand why.
Holding organisations and their leaders to account for the quality of services, and individuals to account for not meeting professional standards, are essential pre-requisites for public confidence in the national safeguarding system. Regulatory bodies for the professions hold this key role. Reviews are not designed for this purpose and will not be used in this way. Nevertheless, where reviews identify any actual or potential errors or violations, they should ensure that proper lines of accountability are followed to ensure that those responsible are held to account.
Working Together to Safeguard Children 2023 defines “Serious child safeguarding cases as those in which:
Serious harm includes (but is not limited to) serious and/or long-term impairment of a child’s mental health or intellectual, emotional, social, or behavioural development. This is not an exhaustive list.”
Working Together to Safeguard Children 2023 advises that “When making decisions, judgement should be exercised in cases where impairment is likely to be long-term, even if this is not immediately certain. Even if a child recovers, including from a one-off incident, serious harm may still have occurred.”
Child perpetrators may be the subject of a review, if the definition of a serious child safeguarding case is met.
Working Together to Safeguard Children 2023 states that “The local authority must notify the Secretary of State for Education, and Ofsted of the death of a looked after child. The local authority should also notify the Secretary of State for Education and Ofsted of the death of a care leaver up to and including the age of 24. This should be notified via the Child Safeguarding Online Notification System. The death of a care leaver does not require a rapid review or local child safeguarding practice review. However, safeguarding partners must consider whether the criteria for a serious incident have been met and respond accordingly, in the event the deceased care leaver was under the age of 18. If local partners think that learning can be gained from the death of a looked after child or care leaver in circumstances where those criteria do not apply, they may wish to undertake a local child safeguarding practice review.”
Safeguarding Partners and other partner agencies, as part of the Case Review Group, are required to consider certain criteria and guidance when determining whether to carry out a Local Child Safeguarding Practice Review. They must take into account whether the case:
They should also have regard to circumstances where:
Working Together 2023 highlights that meeting the criteria does not mean a Local Child Safeguarding Practice Review must automatically be undertaken. Instead, the process outlined in this document will be followed to determine whether a review is appropriate (i.e. whether there is potential to identify improvements).
Buckinghamshire Safeguarding Partners and other partner agencies should make sure there is a clear rationale for completing a Local Child Safeguarding Practice Review. Where a Rapid Review has been undertaken (see Section 4.2), it is important that Safeguarding Partners and other partner agencies ensure that the process for undertaking a Local Child Safeguarding Practice Review is a clear ‘step higher’ than a Rapid Review, building on a Rapid Review, and that the learning for practice is more distinctive.
Local Child Safeguarding Practice Reviews may also be undertaken for cases which do not meet the definition of a ‘serious child safeguarding case’ if they raise issues of importance that could generate learning. Working Together 2023, for example, suggests they might take place “where there has been good practice, poor practice or where there have been ‘near miss’ incidents”.
Where the decision made is not to proceed with a Local Child Safeguarding Practice Review, the Safeguarding Partners and other partner agencies will consider whether there are other learning processes that will bring forward improvements.
Buckinghamshire Safeguarding Partners have agreed that the approach will be ‘systems based’. Each case will, however, be examined individually to determine the most appropriate methodology to identify and maximise learning.
BSCP will conduct Local Child Safeguarding Practice Reviews in line with good practice and the principles of the systems methodology recommended by the Munro Report. This includes the advice outlined in Working Together to Safeguard Children 2023 and its predecessor documents as well as the good practice principles described in the Social Care Institute for Excellence (SCIE) / NSPCC ‘Quality Markers’.
Decisions on whether to undertake a review will be made transparently and the rationale shared with all relevant partners, including families as appropriate.
The child will always be placed at the centre of the process.
All reviews will be proportionate to the circumstances of the case and focus on the potential learning. Specifically, all reviews will be conducted in a way which:
Families, including surviving children, will be invited to contribute to reviews unless there is a strong reason not to. Steps will be taken to sensitively manage their expectations and ensure they understand how they are going to be involved.
Practitioners will be fully involved in reviews and invited to contribute their perspectives without fear of being blamed for actions they took in good faith.
All participants in the review process will be asked to declare any potential conflicts of interest and will be expected to adhere to confidentiality. This will be a standard agenda item at all case specific meetings.
The decision to proceed to a Local Child Safeguarding Practice Review is always a local decision, for which local Safeguarding Partners are accountable. This includes the identification of cases, commissioning and supervising of reviews, and the publication of reports and embedding learning. Safeguarding Partners should take into consideration advice and guidance provided by the national Child Safeguarding Practice Review Panel.
Buckinghamshire Safeguarding Children Partnerships have Local Child Safeguarding Practice Review Group (LCSPR) which is made up of representatives from the Safeguarding Partners in the area, along with any relevant safeguarding experts from partner agencies. This Group will undertake a Rapid Review when Local Authority notifications of serious incidents are made to the national Child Safeguarding Practice Review Panel. They will also consider other cases referred to them by partner agencies and will take responsibility for commissioning and overseeing any resulting Local Child Safeguarding Practice Reviews. This will include monitoring case progression, quality assurance and publication of final reports, and ensuring effective oversight of the implementation of learning.
All decisions related to the commissioning and publication of Local Child Safeguarding Practice Reviews will be notified to the national Child Safeguarding Practice Review Panel.
Information sharing is essential to safeguard and promote the welfare of children and young people. Effective Local Child Safeguarding Practice Reviews are equally dependent on all relevant partners sharing the information they hold about the case and associated professional practice.
The Safeguarding Partners have the formal authority to request information to support both National and Local Child Safeguarding Practice Reviews and the power to take legal action if information is withheld without good reason.
All agencies will be expected to share relevant information within the timescales requested. This may, when necessary, include sharing information without consent. This includes information about parents, guardians and other family members as well as the child(ren) who are subject of the review.
Where a request is for health records, this applies to all records of NHS commissioned care whether provided under the NHS or in the independent or voluntary sector.
When making requests for information, the Safeguarding Partners and other partner agencies will consider their responsibilities under the relevant legislation and have regard to guidance provided by the Information Commissioner’s Office.
Good practice principles around information sharing will always be followed, particularly around ‘how’ information is shared. For example, when responding to requests for information, agencies should:
In the case of any disagreement or failure to comply with a formal information request, the Reviewer or a Case Review Panel member will refer the issue to the LCSPR Group who will seek to resolve this with the strategic Safeguarding Lead for the agency concerned. If a prompt resolution cannot be found, the issue will be escalated to the Safeguarding Partners for formal action.
Reviews will vary in their breadth and complexity but, in all cases, learning should be identified and acted upon as quickly as possible. This includes before the review has formally commenced and while it is in progress.
A Rapid Review and decision on all referrals should be made within the timescales outlined in guidance from the national Child Safeguarding Practice Review Panel (currently within 15 working days) and Local Child Safeguarding Practice Reviews should be completed no later than six months from the date of the decision to initiate a review and more quickly if possible.
Sometimes the complexity of a case does not become apparent until the review is in progress. For example, the Police undertaking a criminal investigation may in some instances request the review delay involving specific key individuals. Any delays need to be considered by the relevant Case Review Group as soon as they arise. If the delay will prevent the publication of the final report within six months, the national Child Safeguarding Practice Review Panel and Secretary of State should be informed and provided with the reason for the delay.
Agencies should inform the Buckinghamshire Safeguarding Partnerships Business Unit of any serious incident which they think should be considered for a Local Child Safeguarding Practice Review, using the Referral Form (see Appendices).
Buckinghamshire Council (Children Service) have a separate duty to:
Where Buckinghamshire Children Services makes a formal notification to the national Child Safeguarding Practice Review Panel, it must always share this with the Partnership Business Office.
A notification by Buckinghamshire Council to the national Child Safeguarding Practice Review Panel will result in a Rapid Review (see Section 4.2).
There will be instances when a referral is made to the LCSPR subgroup by an agency which does not result in a Rapid Review. For example, in a situation where an agency believes a case should be considered by the LCSPR subgroup for a potential Local Child Safeguarding Practice Review, but it does not meet the criteria for a Local Authority Notification to the national Child Safeguarding Practice Review Panel. The formal Referral Form (see Appendices) should be used to make a referral to the LCSPR subgroup in these circumstances.
Where a referral is made by another agency, the Local Authority representative that sits on the LCSPR subgroup will be informed so that they can consider if a notification is required. If it is, the Rapid Review process will be initiated.
The BSCP Business Manager will inform the Partnership Chair of the BSCP and the Chair of the LCSPR Subgroup that a notification has been received.
Where there is no requirement for a Rapid Review, due to the circumstances described above, the following documents can then be used to assist the LCSPR subgroup with obtaining agency information:
The LCSPR Subgroup will discuss the case and make a decision if the criteria for a Local Child Safeguarding Practice Review are met. If they are, the national Child Safeguarding Practice Review Panel will be informed, and the Local Child Safeguarding Practice Review process will be followed.
Rapid Reviews should assemble the facts of the case as quickly as possible in order to establish whether there is any immediate action needed to ensure a child’s safety and the potential for practice learning.
The Rapid Review must be completed within the timescales outlined in guidance from the national Child Safeguarding Practice Review Panel (currently 15 working days of becoming aware of the incident).
See also Local Authority Rapid Review Triage Process (opens as a PDF).
All agencies who have had involvement with the subject child or family will be required to contribute to a Rapid Review. An initial scoping of agencies’ intervention will, therefore, need to be completed and other relevant information will need to be rapidly gathered. To support this, an Information Request Reply Template will be sent out, accompanied by an Information Request Letter. This will be done by the business unit.
The purpose of the initial scoping and information sharing is to gather the basic facts about the case, including determining the extent of agency involvement with the child and family. More detailed information will be sought if the Rapid Review concludes the case has the potential to identify national or local learning and a decision is made to progress to a formal Local Child Safeguarding Practice Review
The Information Request Reply Template should be sent out to all relevant agencies as soon as possible along with an accompanying letter that briefly outlines the notification and explains the purpose of this initial scoping. This should be within 2 working days of receiving the notification.
Agencies should prioritise completion of the template and return it by the deadline included in the letter.
All agencies should consider if they need to secure all records/files in relation to the case, ensuring they are removed to a secure place where they are not accessible to agency personnel other than through a nominated representative.
The Partnership Safeguarding manager will convene a Rapid Review meeting, which will be chaired by the LCSPR subgroup chair.
The date of the Rapid Review meeting should be set as soon as the Information Request has been sent out (see flowchart). The Rapid Review meeting should be scheduled between 7 and 13 working days of receiving the notification. This will allow for analysis of the submitted agency information to establish the key events in the child’s life and inform the Rapid Review whilst also allowing sufficient time to prepare the necessary documents for the national Child Safeguarding Practice Review Panel.
The following documents may be shared with those attending the Rapid Review meeting:
Wherever possible the documentation will be shared with participants in advance of the meeting. However, it is recognised that it may on occasion be necessary to share documentation at the meeting.
The meeting should include representatives from each of the Safeguarding Partners (the Integrated Care Board, Police and Local Authority) and any other relevant agencies. It will only be quorate if at least three representatives from partner agencies, including at least two of the Safeguarding Partners are present.
The Rapid Review meeting should:
If the LCSPR Subgroup feels that information is missing, it may defer a recommendation and adjourn until further information is available and all the facts established. Such a delay may impact on the required timescales for making a decision. Therefore, agencies should ensure they provide full and comprehensive information at the earliest possible opportunity.
The Partnership Chair of the Safeguarding Children Partnership will be sent the information regarding the Rapid Review.
The Chair of the LCSPR Sub Group will put the Sub Group’s recommendation in writing to the Partnership Chair of the BSCP within one month of the notification of the incident using section 2 of the LCSPR Referral Form (see Appendices). Dependent on the outcome of discussions, the recommendation will be one of the following:
This allows the Partnership Chair to provide independent advice, being aware of the discussion that has taken place, but not unduly influencing the main meeting
The Partnership Chair of the BSCP will make his/her decision upon receipt of this recommendation and reply in writing to the Chair of the LCSPR Sub Group using Section 3 of the LCSPR Referral Form (see Appendices).
The Chair of the LCSPR Subgroup will inform the referrer of the Partnership Chair’s decision.
Although the final decision rests with the Chair of the BSCP, the Chair may seek peer challenge from another LSCP Chair when considering this decision and also at other stages in the LCSPR process.
The Business Office will send a Rapid Review Report to the national Child Safeguarding Practice Review Panel ([email protected]).
The Partnership Chair of the BSCP will notify Board members of his/her decision. If the decision is not to initiate a LCSPR or any other type of learning review, Board members will be advised that associated records no longer need to be kept secure
Other agencies (including the agency who made the referral) should also be informed of the outcome of the Rapid Review.
Individual agencies should notify their own inspectorate bodies as required
In cases where the BSCP Chair has decided to initiate a LCSPR, the Chair should provide the National Panel with the names(s) of the reviewer(s) appointed to conduct the LCSPR and the methodology that will be used for the review.
In cases where the BSCP Chair has decided not to initiate a LCSPR, the decision will be subject to scrutiny by the National Panel. The BSCP should provide information to the National Panel on request to inform its deliberations and the Chair of the BSCP should be prepared to attend in person to give evidence to the National Panel.
The LCSPR Subgroup should consider an alternative form of learning review where the criteria for an LCSPR are not met. A relevant and proportionate methodology should be selected on a case-by-case basis. Examples include:
As with LCSPRs, the BSCP through the LCSPR subgroup will monitor the implementation of actions resulting from these reviews and reflect on progress in its annual report.
The process will vary depending on the methodology being used.
The LCSPR Panel should aim for completion of an LCSPR within six months of initiating. If this is not possible (for example because of potential prejudice to related court proceedings), every effort should be made to ensure this does not prevent any learning being captured and any corrective action being taken.
Dependent on the methodology used to undertake a Local Child Safeguarding Practice Review, a Reviewer may be appointed to manage the review process, chair meetings of the Case Review Panel, facilitate the Learning Workshops and author the final report.
Where an LCSPR is being conducted, the reviewer must be independent of the BSCP, of partner organisations involved in the case and from professionals and LCSPR Panel members involved in the case.
The reviewer must have demonstrated that they are qualified to conduct reviews using the principles set out in Working Together to Safeguard Children 2023 and in line with the agreed review methodology.
The reviewer will be commissioned by the BSCP Business Manager in accordance with the BSCP’s standard contract for Independent Authors.
The reviewer is responsible for:
In producing the overview report, the reviewer should:
In producing the final draft, the reviewer should satisfy the LCSPR Panel that all issues raised by the Panel have been addressed.
The LCSPR Subgroup should recommend a suitable person to act as Chair for the LCSPR Panel. This can be someone from a local agency as long as that agency was not involved in the case. The Chair should have relevant skills taking into account the specific issues in the case.
The LCSPR Panel Chair is responsible for:
The LCSPR Panel Chair and BSCP Business Manager should ensure that:
Where appropriate a small, multi-agency Case Review Panel will be established to oversee each review. This will include a representative from each of the Safeguarding Partners along with representatives of any other multi-agency partners. Other relevant subject matter experts may be included depending on the case.
The Case Review Panel will support the Reviewer in quality assuring agency Information Reports and facilitating Learning Workshops. The Panel will also provide local context and challenge to the analysis of professional practice and the identification of learning.
The Police representative will be responsible for liaising with the Senior Investigating Officer, Crown Prosecution Service, and for co-ordination of family liaison.
The LCSPR Subgroup will identify initial panel members. Panels should include senior representatives of the agencies involved in the case or specialists in the professions involved. These representatives should be independent of the case under review, having had no direct management involvement and must have sufficient seniority to be able to comment on their agency’s practice. The panel may also include representatives from other non-involved partner agencies to ensure further independence and support for the LCSPR process. Legal advice should be available to the Panel via the BSCP legal adviser, who may sit as a member of the Panel or, where appropriate, provide advice to the Panel where required. The panel may also co-opt additional members in relation to specific issues that arise during the LCSPR process.
Panel members should not also be responsible for writing agency reports as this could lead to a conflict of interest and prejudice their independence.
The expectation is that membership of the Panel will remain constant. Agencies should ensure that sufficient time is allocated to enable the representative to effectively undertake the work of the LCSPR Panel.
The membership of the Panel may need to be extended, once the terms of reference have been established.
The LCSPR Panel is collectively responsible for the quality, effectiveness and timeliness of the review. The specific functions of the panel are:
For more information see, Child Safeguarding Practice Review Panel Guidance for Partners (Publishing Services .Gov.uk)
The development of the Terms of Reference (TORs) will be dependent on the specific methodology employed to review an individual case. The LCSPR subgroup should have an early input into the Terms of Reference.
If a Case Review Panel is set up to manage the specific review, they will have the responsibility of completing the Terms of Reference at an early stage of their first meeting. If a Reviewer is commissioned, they will also be involved in the development of the Terms of Reference. Any issues raised by the Case Review Panel or Reviewer that cannot be resolved will be referred to the LCSPR subgroup for a decision.
The initial scope and terms of reference for the review may need to be revised if significant new information emerges during the review, e.g. they might identify other key agencies/organisations involved or they might indicate that the timeframe for the review needs to be adjusted to allow focus on a particular period.
The LCSPR subgroup will formally agree the scope and Terms of Reference for the review.
The scoping period covered by the review should reflect the potential learning likely to be achieved. (There is little value in identifying weaknesses in professional practice or procedures that have already changed). It should, therefore, be as short and as recent as possible. This, however, needs to be balanced against the need to understand the pattern of child abuse or neglect and whether early help interventions could have been beneficial.
The Rapid Review is likely to identify the key lines of enquiry to be explored as part of the review. These will be confirmed and formally identified in the Terms of Reference. These may, however, be revised as more information becomes available. Any significant changes should be formally approved by the Case Review Group.
Each case will be examined individually, and the methodology will be adapted to meet the specific needs of the case.
The Terms of Reference will specify the methods of information collection and collation tools that will be used in the review. This may include Chronologies (of key events and/or organisational changes), Information Reports or a combination of these (see Section 15, Methodology for more information).
Using the information available, and the genogram where available, consideration will be given to which family members are relevant to the review and how the family, siblings and the child (where the review does not involve a death) should be invited to contribute.
The information and support that children and family members are likely to require to effectively engage will also be identified.
Plans to engage children and family members will need to take into account any parallel investigations. For more information see Section 14, Engaging with Children and Families.
The case may also be subject to a criminal or coroner’s investigation, individual agency or professional body disciplinary procedures, and/or another type of formal review. It is anticipated that a Local Child Safeguarding Practice Review will go ahead unless there are clear reasons not to. Identifying and responding to learning in a timely manner is important and supports a more effective review.
Under Working Together to Safeguard Children 2023 there is greater discretion as to when a Local Child Safeguarding Practice Review should take place and who does it. This enables greater flexibility in designing the right review methodology whilst meeting statutory obligations. Where there are parallel investigations, this is best considered at the scoping stage to reduce duplication and the impact on children and families and maximise learning.
Consideration will be given to whether legal advice will be required at the outset or during the review.
Taking into account the factors summarised above, the timetable for the review will be agreed. This will include the timing of Case Review Panel meetings, Learning Events and engagement with families.
Working Together to Safeguard Children 2023 highlights the crucial importance of inviting families, including surviving children, to contribute to reviews. This will help ensure that the review reflects the child’s perspective and the family context.
In line with good practice, consideration will be given to how family members can be supported to engage. This may include interpretation and translation support if English is not a first language, additional support for disabled parents, specialist support where there are issues of domestic abuse, and drawing on expertise to facilitate the appropriate involvement of children.
Family engagement will be included as a standing item at all Case Review Panel meetings. The Panel will also identify an individual who will take responsibility for co-ordinating communication with family members.
The lead agency working with the child/family will usually be asked to prepare a full and accurate genogram to assist the clarification of family relationships and dynamics. This will be shared with other agencies at Panel meetings and in the Reflective Learning Workshop (see Section 15.9) and will be updated based on any additional information on the family provided by these agencies. The genogram will not be in the final published report with any names included.
Family members, including surviving children, will be informed of the review and invited to contribute unless there is a strong reason not to do so. The Case Review Panel will discuss family involvement and agree an approach that will sensitively manage their expectations and ensure they understand the process.
Personal contact should be made whenever possible by the most appropriate practitioner and the family provided with a letter (where required, signed for or hand delivered by an appropriate practitioner such as the social worker) and/or leaflet to explain and introduce the process and Reviewer.
Family engagement will normally be led by the Reviewer and conversations should ideally take place before the Learning Event (see Section 15.9) so that the family’s views can be included alongside the analysis of practice.
It is recognised that family members may decide not to take part in the review. All reasons for non-involvement of family members (for example, parallel investigations or the choice of the individual) will be documented in the final report.
Working Together to Safeguard Children 2023 does not specify the methodology that should be used in Local Child Safeguarding Practice Reviews but there is an explicit expectation that “principles of the systems methodology recommended by the Munro Report” will be “taken into account” by the Safeguarding Partners and other partner agencies when agreeing the method by which the review will be conducted.
This section describes the systems-based approach. This is consistent with both the guidance in Working Together to Safeguard Children 2023, and the principles of the systems methodology recommended by the Munro Report.
Each case will be examined individually, and the methodology may be adapted to meet the specific needs of the case, to ensure a proportionate response, and to maximise learning to improve both frontline safeguarding practice and organisational structures. For some cases, the Safeguarding Partners and other partner agencies may agree to use a different methodology.
All agencies which provided services to the family during the time period specified in the Terms of Reference will be formally requested to participate in the review process. The extent of agency engagement will be dependent on the type of review commissioned, the specific Terms of Reference and methodology chosen.
Each organisation should have an identified Safeguarding Lead to act as a single point of contact for the co-ordination and support of the review process.
Agencies should ensure that all requests for information are acted upon in a timely fashion and practitioners are released to participate in the review. Agencies should also provide support to their staff who are affected by the case where required.
The Terms of Reference will specify the information collection and collation tools that will be used in the review. Information will usually be collected using chronologies and Information Reports.
Where chronologies are used, all relevant agencies will be asked to complete a chronology of their agency’s involvement in relation to significant events that are relevant to the case. They may also be asked to produce a chronology of any organisational changes which may have impacted on frontline practice during the same period. If required, chronologies can include columns to provide analysis of individual events, including if an agency’s response to an event was expected practice.
Agencies will be sent a Chronology Template and Accompanying Letter, along with Guidance on Completing the Chronologies.
Individual agency chronologies will be collated to produce a Multi-Agency Chronology.
Information Reports will be requested from agencies where required in order to analyse the agency’s involvement with the child and family and any themes that have emerged. The report should be focused on systems learning and outline any potential learning for the agency and for multi-agency arrangements and should include information about actions already undertaken.
Agencies will be sent an Information Report Template and Accompanying Letter, along with Guidance on Completing an Information Report.
If an agency / organisation has had contact with a subject of a Local Child Safeguarding Practice Review or their family, but their involvement was limited, and no significant incidents have taken place during their contact or as a result of their contact, they may be asked to complete a Factual Summary. This sets out their agency / organisation’s involvement without requiring any analysis of the agency’s involvement.
The Case Review Panel, chaired by the Reviewer, needs to be satisfied that the appropriate level of information has been provided by each agency and that the analysis provides sufficient insight into the actions undertaken by the agency and possible learning.
If necessary, the Panel may decide to either request more information from an individual agency or invite them to attend a meeting if further clarity is needed about their agency’s role with the child and/or family.
Using the chronologies and/or analysis in the Information Reports, the Panel will discuss the case in detail and develop the key themes for analysis. These should be as few as practicable and focus on core learning. The key themes should identify issues of practice that have emerged within the case which can (i) be transposed into working with families more generally and (ii) give insight into the systems which operate formally or informally within safeguarding practice. Some examples might be “making space and time for children” or “the use of assessments to inform future interventions”.
The key themes for analysis may be shared with participants prior to their attendance at the Reflective Learning Workshop.
Reflective Learning Workshops provide a forum for practitioners involved in the case and their Line Managers to come together in a respectful, positive and supportive environment to consider the circumstances surrounding the case and the reasons why actions were taken. This enables the Reviewer and Panel to explore factors influencing workers working with the family at the time, their decisions and identify important multi-agency learning.
A Reflective Learning Workshop will not be suitable for all reviews. In some cases, the key individuals who had worked with children and families will have left the agencies that they had been employed by at the time of their involvement with a case.
The Panel will need to ensure it has a list of appropriate practitioners and their Line Managers to invite to the Learning Workshop. This will usually be requested alongside the chronology and/or Information Report.
To maximise learning all agencies are expected to ensure that appropriate staff attend the workshop. However, only those who have had some form of direct operational involvement with the child and family should attend.
An Invitation to the Reflective Learning Workshop will be sent to all participants giving plenty of notice. This will be accompanied by a short briefing which explains the purpose of the event and the importance of attending.
The Reflective Learning Workshop will normally be undertaken over half a day, although a more complex case may require an additional half day.
The Reviewer will normally facilitate the Reflective Learning Workshop, supported by members of the Panel.
The structure of the Workshop will vary depending on the case but is likely to include a discussion of:
Within these discussions it is essential that all actions and decisions (or lack of them) by professionals are viewed within the context of the information available at the time and system in which they were working.
The Reviewer will assist the group to avoid hindsight bias in their consideration of what took place.
Where an individual with important information to contribute to the review is unable to participate in a Reflective Learning Workshop, arrangements may be made to facilitate a conversation with the Reviewer to enable them to contribute to the learning.
It is expected that reports will be published so the Reviewer should draft the formal report with publication of the report in mind.
Reports should meet any requirements specified in the agreed Terms of Reference for the review and, as a minimum, should also succinctly include:
Reports should be written in a way that avoids harming the welfare of any children or vulnerable adults in the case. Information should be appropriately anonymised and very intimate and personal detail of the family’s life should be kept to a minimum to reduce the sensitivity of publication.
The Case Review Panel will be responsible for ensuring the quality of the draft report has met the agreed Terms of Reference, is succinct and focused on improving local safeguarding arrangements.
The final report must be formally approved by the relevant Case Review Group followed by the Safeguarding Children Partnership.
The analysis of the information collected during the review, coupled with the feedback from a Reflective Learning Workshop, should lead to the identification of key learning in the form of specific findings in the report.
These findings may be developed into formal recommendations that will form part of the final report. Buckinghamshire Safeguarding Children Partnership may choose to convene a dedicated group to consider the learning and how this can be developed into meaningful actions.
In some cases, Buckinghamshire Safeguarding Children Partnership may decide at the outset of a review that the identified findings in the report will be considered by a separate group who will identify what action needs to be taken to address a specific finding.
Whichever approach is taken; Buckinghamshire Safeguarding Children Partnership will be able to engage key strategic stakeholders and consider the potential learning in the context of wider operational and strategic developments. This will ensure that actions are focused on the issues that will make a real difference and, therefore, maximise the opportunity to deliver meaningful change.
In all cases, learning will be focused on improving outcomes for children and should be clear about what is required of relevant agencies and others collectively and individually, and by when.
The Safeguarding Partnership is required to publish the reports of Local Child Safeguarding Practice Reviews, unless they consider it inappropriate to do so.
Working Together to Safeguard Children 2023 states that all reviews of cases meeting the LCSPR criteria should result in a report which is published and readily accessible on the BSCP’s website for a minimum of 12 months. Thereafter, the report should be made available on request. This is important to support national sharing of lessons learnt and good practice in writing and publishing LCSPRs.
If an LSCP considers that a LCSPR report should not be published, it should inform Ofsted, the Department for Education and the national Child Safeguarding Practice Review Panel, which will provide advice to the LSCP. The LSCP should provide all relevant information to the National Panel on request to inform its deliberations.
Publication of SMART multi-agency action plans, arising from the recommendations of the review (or a clear statement of why the partnership does not accept them), should also be considered. These should be published alongside the Local Child Safeguarding Practice Review, for accountability and as a sign of the partnership’s commitment to learning and improvement.
Publication will be considered throughout the review process and media planning will commence as soon as the final draft report has been formally endorsed by the Case Review Group and Safeguarding Children Partnership. Publication planning will include strategic leads from all the agencies involved in the review and their media/communication leads.
Buckinghamshire Safeguarding Children Partnership should publish, either as part of the LCSPR report or in a separate document, information about:
LSCPs must comply with the Data Protection Act 2018 in relation to LCSPRs, including when compiling or publishing the report, and must comply also with any other restrictions on publication of information, such as court orders.
Consideration will be given to how best to manage the impact of the publication on children, family members, practitioners and others closely affected by the case.
The wishes of the child’s family will be considered as part of the publication and media planning. The proposed publication arrangements will then be discussed with the family and appropriate steps will be taken to minimise the disruption and distress that any media attention surrounding the publication may cause to family and friends.
The arrangements for informing practitioners will also be considered. It is likely that the senior managers from each agency will take responsibility for informing frontline staff of the date of publication and ensuring they have appropriate support.
All media enquiries regarding LCSPRs must be referred to the Independent Chair of the BSCP via the BSCP Business Manager.
A central point of contact for media enquiries should be identified. This individual can coordinate media enquiries during the publication phase and ensure effective liaison is maintained with each organisation’s strategic and media leads.
The BSCP will ensure that a media strategy is developed in advance of publishing an LCSPR, including, where appropriate, an agreed statement which will be shared with relevant partners. The BSCP will liaise with the local authority’s Communications Team and nominated media contacts of relevant partner agencies prior to publication to ensure all relevant parties are fully briefed.
Any media enquiries relating to services or individuals associated with an LCSPR should also be discussed with the BSCP Partnership Chair to ensure that consistent and clear messages are provided in a co-ordinated response.
Working Together to Safeguard Children 2023 states that “Safeguarding partners must send a copy of the full report to the panel and to the Secretary of State no later than seven working days before the date of publication. Where the safeguarding partners decide only to publish information relating to the improvements to be made following the review, they must also provide a copy of that information to the panel and the Secretary of State within the same timescale. They should also provide the report, or information about improvements, to Ofsted within the same timescale.”
The Safeguarding Children Partnership must send a copy of the full report to the National Panel, Ofsted and to the Department of Education no later than seven working days before the date of publication. Reports should be submitted electronically to:
Published reports will always include the name of the reviewer(s) and will be made available to read and download from the appropriate Safeguarding Children Partnership website, unless these are published anonymously. Reports will be publicly available for at least one year. Archived reports will be available on request from the Safeguarding Children Partnership, through the relevant Business Office.
On a case-by-case basis, it will be considered if published reports will also be submitted for inclusion in the NSPCC National Repository of Safeguarding Case Reviews. Reports will be submitted by email to: [email protected]
The purpose of a Local Child Safeguarding Practice Review is to identify improvements that can be made to safeguard and promote the welfare of children. Disseminating and embedding the learning is, therefore, crucial.
The Panel will consider at every meeting whether any immediate single or multi-agency action is required to respond to emerging issues identified through the review process. They may wish to deliver swift messages to the workforce in specific agencies or disseminate multi-agency learning to a wider workforce. In so doing, the Panel will consider what information is shared and whether this will have an impact on family members or any parallel investigations.
Buckinghamshire Safeguarding Children Partnership will be responsible for ensuring the identified improvements are implemented locally, including the way in which organisations and agencies work together.
A clear plan for disseminating and sharing the learning from the review with all relevant agencies will be developed. This may include organising single or multi-agency meetings or producing briefing notes on the lessons learned for use in agency team meetings and/or supervision sessions.
It is the responsibility of the agencies who have participated in the review to ensure their agency recommendations are fully implemented and used to make improvements to their safeguarding children arrangements and information on this and the impact of improvement is reported o the Safeguarding Children Partnership.
Methods for sharing LCSPR learning include:
The Quality Assurance Subgroup will regularly audit progress on the implementation of recommended improvements and will regularly monitor and follow up actions to ensure improvement is sustained. This will be via the Buckinghamshire Safeguarding Children Partnership Multiagency Safeguarding Arrangements.
The BSCP section 11 audit will allow the BSCP to gain assurance around how individual agencies disseminate learning from LCSPRs and other forms of review within their own agency. Where necessary, the LCSPR Sub Group may also ask agencies to provide additional information.
The LSCPR Subgroup will also review the learning from all national reviews and consider how it can be applied at a local level.
The Child Safeguarding Practice Review Panel decides whether it is appropriate to commission a National Child Safeguarding Practice Review, as set out in Working Together to Safeguard Children 2023. They state that “The national reviews we commission may be thematic reviews based on types of cases or systemic issues that we see frequently or are identified as important national issues, or they may be individual case reviews where a particular case is significant in terms of its complexity or implications for national learning.”
The Child Safeguarding Practice Review Panel also states: “An important part of setting up the review process is a dialogue between the Panel and the local areas affected. This helps make sure the scope and methodology of the review maximises the learning potential and the most efficient of resources, including the time of those involved at a local level. Where the Safeguarding Children Partnership receives a request around a National Child Safeguarding Practice Review, the Statutory Partners and, subsequently, the Case Review Group will be informed about the request and the parameters. The Chair of the Case Review Group will be the main point of contact, and the Business Office will help facilitate any information required / local agency attendance at meetings.
Referral Form – to share serious incidents for consideration by the Rapid Review Panel (opens in Word)
Action Plan Template (opens in Word)
RELATED POLICIES
Child Safeguarding Practice Reviews
RELEVANT GUIDANCE
Working Together to Safeguard Children (Department for Education)
Resuscitation Guidelines (UK Resuscitation Council)
Sudden Unexpected Death in Infancy and Childhood (Royal College of Pathologists and Royal College of Paediatrics and Child Heath)
The majority of sudden child deaths are the result of natural causes and are a tragedy for any family. Every child who dies deserves to have their sudden and unexplained death fully investigated so that a cause of death can be identified.
This procedure sets a minimum standard for a rapid response service for unexpected deaths in infancy and childhood, as outlined in Working Together to Safeguard Children.
This procedure applies when a child dies unexpectedly (from birth up to the 18th birthday, excluding stillborn babies), or where there is a lack of clarity about whether a death of a child is unexpected.
It is acknowledged that each death has unique circumstances and professionals involved have their own experience and expertise, which is drawn upon in handling individual cases.
This procedure provides guidance on capturing immediate information about an unexpected child death, while also giving support to the bereaved family. This ensures that early opportunities for information-gathering are not lost.
Throughout this procedure, the term ‘parent’ is used to refer to any parent or carer, including the person with a Special Guardianship Order or Child Arrangements Order, foster parents and the local authority for those in care.
An unexpected death is defined as the death of an infant or child which was not anticipated as a significant possibility, for example 24 hours before the death; or where there was an unexpected collapse or incident leading to, or precipitating, the events which lead to the death.
Children dying at home, or in a hospice or other setting, who had been undergoing end-of-life care will not normally be considered to have died unexpectedly, and a rapid response to such deaths is rarely necessary.
When a child with a known life-limiting and or life-threatening condition dies in a manner or at a time that was not anticipated, the rapid response team should liaise closely and promptly with a member of the medical, palliative or end-of-life care team who knows the child and family, to jointly determine how best to respond to the child’s death.
The ‘Designated Paediatrician’ responsible for child death should be consulted where professionals are uncertain about whether the death was unexpected. If in doubt, the processes for unexpected child deaths should be followed until the available evidence enables a different decision to be made (i.e. until it becomes clear that the death was expected).
Professionals need to strike a balance between the sensitivities of handling the bereaved parents and securing and preserving evidence which may aid them in arriving at an understanding of why a child has died.
When dealing with an unexplained child death, all agencies need to follow these common principles:
The service response to an unexpected child death should be safe, consistent and sensitive to those concerned. Bereaved parents and siblings should receive a similar response across Buckinghamshire.
Professionals should be aware that, in certain circumstances, separate investigative processes may be taking place alongside those described in this procedure (e.g. murder investigations, Sudden Unexpected Death in Infancy [SUDI] processes). Professionals and agencies should liaise across processes to avoid duplication.
The purpose of a rapid response service is to ensure that the appropriate agencies are engaged and work together to:
Rapid response begins at the point of death and ends when the final meeting has been convened and chaired by the designated paediatrician or equivalent. Any records of the meeting (i.e. statutory child death reporting form, meeting notes) should be forwarded to the CDOP at the time of the review.
The area in which the death of a child has been declared must take initial responsibility for convening and co-ordinating the rapid response process, until agreement for handover can be secured with the area where the child was normally resident.
Where notified of a death abroad, the professionals responsible for child death in the local authority where the child is normally resident must consider implementing this procedure as far as is practically possible, and fully record any decisions made.
The Designated Paediatrician has responsibility for ensuring a rapid response team is formed in response to each unexpected child death and that the rapid response process is carried out by them.
In the absence of the Designated Paediatrician, the on-call senior attending doctor will take on these duties and report progress to the Designated Paediatrician at the earliest opportunity. The Designated Paediatrician therefore maintains senior oversight of all cases requiring a rapid response.
In Buckinghamshire, young people aged 16 to 18 do not normally come under the remit of paediatricians. Where there is an unexpected death in a young person aged between 16 and 18, the Accident and Emergency Consultant or other medical consultant will initiate the rapid response process, whilst consulting the Designated Paediatrician.
The Designated Paediatrician is responsible for ensuring all actions relating to the rapid response process are completed. The rapid response timeline involves three phases:
The police will begin an investigation into the unexpected death of a child on behalf of the coroner. They will carry this out in accordance with College of Policing guidelines.
A case discussion should take place as soon as practicable and, in any case, within one week of the child’s death, in order to:
Prior to this meeting, the Designated Paediatrician should discuss the case with the pathologist (when a post-mortem has taken place and consent obtained from the coroner) and the police senior investigating officer, where appropriate.
A further case discussion meeting should be convened and chaired by the Designated Paediatrician (or other relevant professional where negotiated) following the final results of the post-mortem examination becoming available. This should involve those who knew the child and family, and those involved in investigating the death – the GP, health visitors, school nurse, paediatricians, pathologist (or pathologist report), police senior investigating officers, coroner or coroner’s office, and, where relevant, education and social workers.
At this stage, the collection of the Child Death Core dataset should be completed: Form D – Audit tool for Rapid Response and Form B13 – Summary of autopsy findings.
The discussion meeting should explicitly address the possibility of abuse or neglect as causes or contributory factors in the death, and the outcomes of this should be recorded.
The meeting should agree how and by whom the parents will be informed about the post-mortem results and the outcome of the meeting. This meeting should also agree how and by whom the parents will be offered ongoing support and given the opportunity to have their views taken into account by the CDOP review.
Where other investigations are ongoing, the meeting should conclude with a record of the current situation.
An agreed record of the case discussion meeting and all reports should be sent to the coroner, to take into consideration in the conduct of the inquest and, in the cause of death, notified to the Registrar of Births and Deaths.
The record of the case discussion and the record of the core data set should also be made available to the BSCP’s CDOP Panel.
When a child dies away from their normal place of residence, a joint decision will need to be made by the rapid response teams in both areas as to which team will lead the investigation and in which Local Safeguarding Children Partnership (LSCP) area the case review meeting should be held. On occasions, separate meetings may be appropriate in both LSCP areas, but good communication between the teams is essential.