Neglect Strategy (2026 – 2028) opens as a PDF, in a new window.
Was this helpful?
Thanks for your feedback!
Neglect Strategy (2026 – 2028) opens as a PDF, in a new window.
RELEVANT GUIDANCE
Bullying and Cyberbullying – Advice for Parents and Carers (NSPCC)
“Back me up” – Video and Lesson Plan on Peer Pressure (Childnet)
CONTENTS
Bullying may be defined as behaviour by an individual or a group, repeated over time, which intentionally hurts another individual or group, either physically or emotionally. It can take many forms, including:
Bullying can happen face to face or virtually, for example online through social networking sites, online forums or gaming or mobile phones. The use of information communications technology (ICT) to bully impacts on the way bullying takes place – meaning it can happen at any time of day or night, and can be much more subtle or hidden, including taking place when a child is alone in their room. It also potentially involves a much larger audience, including a large number of bystanders and can spread very quickly to become ‘viral’.
It is important to recognise that in some instances bullying will raise safeguarding concerns and/or involve a criminal offence. Bullying behaviour may result in a criminal investigation where there is physical assault, damage, threats or harassment.
Bullying often involves an imbalance of power between the victim and the perpetrator which gives the perpetrator control over the relationship and makes it difficult for the victim to defend themselves. This imbalance can take a number of forms. For example, it may be physical, psychological, intellectual, derive from having the support of a group or the capacity to socially isolate.
While bullying often involves children as both victim and perpetrator, it can occur at any age. Professionals should be just as alert to cases of bullying which might involve an adult perpetrator bullying a child, or a child perpetrator bullying an adult.
Bullying should be defined by the impact on the victim rather than the intention of the perpetrator.
Prejudice-related incidents involve the nine protected characteristics as set out in the Equality Act 2010:
Prejudice-related incidents can take many forms, including prejudicial language, ridicule and jokes, verbal abuse and graffiti. There is a crossover between prejudice-related incidents and bullying. However, they are also distinct; not all incidents of bullying will be prejudice-related, and not all prejudice-related incidents will involve bullying.
When dealing with prejudice-related incidents, professionals should be particularly aware that they do not just impact on the individual involved, but are an attack on someone who is a representative of a community or group, which means the impact is felt more widely. This has the potential to spread fear and/or create a hostile environment.
Buckinghamshire Council has developed guidance for schools around prejudice-related incidents. This includes further exploration of the similarities and differences between prejudice-related incidents and bullying. The guidance also covers how schools should respond to and record prejudice-related incidents. The guidance can be found in the Appendix.
There is no statutory duty to report such incidents to the local authority, however schools must keep their own internal records of discriminatory incidents as Ofsted could ask for any such records as part of an inspection.
A hate crime is a crime committed against someone because of their disability, gender-identity, race, religion or belief, or sexual orientation. A hate crime must involve a criminal offence.
Hate crimes can include threatening behaviour, assault, robbery, damage to property, inciting others to commit hate crime and harassment.
Professionals should be aware that there may be a crossover between bullying and hate crime in cases where bullying behaviour relates to disability, gender-identity, race, religion or belief, or sexual orientation and a criminal offence has taken place.
Because a criminal offence is involved, all incidents of hate crime should be reported to the police.
The damage inflicted on children by bullying can frequently be underestimated. It can cause considerable distress to children, to the extent that it affects their health and development or, in extreme cases, causes them significant harm (including self-harm).
Children are often held back from telling anyone about their experience for a number of reasons, including:
Bullying is often motivated by prejudice, difference or vulnerability, whether actual or perceived. For example, a perpetrator may pick on someone because they are adopted, have caring responsibilities or because of the way they look. Children Living Away from home are particularly vulnerable to bullying and abuse by their peers (see BSCP guidance on Children Living Away from home). Bullying may relate to characteristics that are protected under the Equality Act 2010 including disability, race, religion or belief, gender and sexual orientation.
Consideration should always be given to the underlying reason for the bullying so that prejudices and assumptions can be challenged and addressed appropriately.
Bullying often starts with small events such as teasing or name calling, which if left unchallenged can lead to more serious bulling and abuse.
Children who bully have often been bullied themselves. There may also be underlying circumstances which are contributing to the bullying behaviour, such as a disrupted home life, exposure to violence or a lack of self-confidence. While these reasons do not justify the bullying behaviour, professionals should recognise that in some cases the perpetrator may need support to deal with the underlying circumstances that are leading to their behaviour.
Changes in behaviour which indicate fear or anxiety may be a potential indicator of bullying. The behaviours listed below are ones which can be associated with bullying, although it is important to recognise that bullying will not always be the reason why a child is displaying these behaviours.
All settings in which children are provided with services, or are living away from home should have rigorously enforced anti-bullying strategies in place and clear procedures on how to refer to Children’s Social Care if safeguarding concerns are identified (see Referrals chapter).
Clear messages must be given that bullying is not acceptable and children must be reassured that the adults they are in contact with will take bullying seriously.
Schools have a legal duty to put measures in place to promote good behaviour, respect for others and to prevent all forms of bullying among pupils. In practice, schools need to draw up an anti-bullying policy linked to the behaviour policy.
Bullying may become a safeguarding issue and, particularly in cases of sexist, sexual and transphobic bullying, schools must consider whether safeguarding processes need to be followed. This is because of the potential for this form of bullying to be characterised by inappropriate sexual behaviour and the risk of serious violence (including sexual violence).
It is important for professionals to consider whether to apply safeguarding procedures both to the young people being bullied, and to the perpetrators. Victims of bullying may need to be protected from the child or young person engaging in bullying behaviour using safeguarding processes. Safeguarding processes may need to be applied to perpetrators in cases where their behaviour is an indication they are experiencing or impacted by abuse.
In all cases, where bullying is taking place, action should be taken to address the needs of the victims and the perpetrator and to provide appropriate support and services.
If the bullying involves physical assault, as well as seeking medical attention where necessary, consideration should be given as to whether there are any safeguarding children issues and whether the police should be informed if a criminal offence may have been committed.
Where appropriate, parents and carers of both victims and perpetrators should be kept informed and updated on a regular basis. Where possible they should also be involved in supporting the strategies that are being put in place to manage the bullying.
It is important when addressing bullying behaviour by another child to avoid accusations, threats or any responses that will only lead to the child being uncooperative, and silent.
The focus should be on the bullying behaviour rather than the child and, where possible, the reasons for the behaviour should be explored and dealt with. A clear explanation of the extent of the upset the bullying has caused should be given and encouragement to see the bullied child’s points of view.
A restorative approach and the use of restorative enquiry and subsequent mediation between those involved can provide an opportunity to meet the needs of all concerned. The child who has been bullied has the chance to say how they have been affected. The opportunity is provided for the child doing the bullying to understand the impact of their actions and to make amends.
Both the child engaged in bullying behaviour and those who are the target of bullying should then be closely monitored. The times, places and circumstances in which the risk of bullying is greatest should be ascertained and action taken to reduce the risk of recurrence.
Whatever plan of action is implemented, it must be reviewed at regular intervals to ascertain whether actions have been successful by consideration of whether the target of bullying now feels safe and whether the bullying behaviour has now ceased. Consideration should also be given to lessons learned in order to constantly review and improve practice.
Schools can contact Yvette Thomas, Equalities and School Improvement Manager at Buckinghamshire Council, for further advice and support around bullying. Guidance for schools on dealing with prejudice-related incidents and disability bullying can be found in the Appendix.
Buckinghamshire Council Schoolsweb has up to date information on all Equalities Issues which include resources for school, children and young people and professionals.
The Department for Education have published guidance on Preventing and Tackling Bullying. Materials include advice on supporting children and young people who are bullied, and advice for both teachers and parents on cyberbullying.
Ofsted has a challenge role with schools in looking at how children and young people are being kept safe from bullying as part of their inspections, and gathers views from parents and children and young people as part of this process. If weaknesses are identified these will be flagged up in the Ofsted report.
The Anti-Bullying Alliance (ABA): Founded in 2002 by NSPCC and National Children’s Bureau, the ABA brings together over 100 organisations into one network to develop and share good practice across the whole range of bullying issues.
Kidscape: A charity established to prevent bullying and promote child protection. Provides advice to young people, professionals and parents about different types of bullying and how to tackle it. They also offer specialist training and support for school staff, and assertiveness training for young people.
The Diana Award: An anti-bullying ambassadors programme to empower young people to take responsibility for changing the attitudes and behaviour of their peers towards bullying. It aims to achieve this by identifying, training and supporting school anti-bullying ambassadors.
The BIG Award: The Bullying Intervention Group (BIG) offer a national scheme and award for schools to tackle bullying effectively.
Childnet – Cyberbullying Guidance
UK Safer Internet Centre – Online Bullying
EACH: A training agency for employers and organisations seeking to tackle discrimination on the grounds of gender and sexual orientation.
Schools Out: Offers practical advice, resources (including lesson plans) and training to schools on LGBT+ equality in education.
Stonewall: An LGBT+ equality organisation with considerable expertise in LGBT+ bullying in schools, a dedicated youth site, resources for schools, and specialist training for teachers.
Mencap: Represents people with learning disabilities, with specific advice and information for people who work with children and young people.
Changing Faces: Provide online resources and training to schools on bullying because of physical difference.
Cyberbullying and Children and Young People with SEND: Advice provided by the Anti-Bullying Alliance on developing effective anti-bullying practice.
Show Racism the Red Card: Provides resources and workshops for schools to educate young people, often using the high profile of football, about racism.
Kick it Out: Uses the appeal of football to educate young people about racism and provides education packs for schools.
Anne Frank Trust: Runs a schools project to teach young people about Anne Frank and the Holocaust, the consequences of unchecked prejudice and discrimination, and cultural diversity.
Dealing with Prejudice Related Incidents: Guidance for Schools (Buckinghamshire Council)
All Inclusive: Tackling Disability-Related Bullying in Primary Schools (Buckinghamshire Council)
RELATED GUIDANCE
CONTENTS
Child abuse linked to faith or belief can include:
This is not an exhaustive list.
Not all those who believe in witchcraft or spirit possession harm children. Data on numbers of known cases suggest that only a small minority of people with such beliefs go on to abuse children, although under-reporting is likely. The number of cases of child abuse linked to faith or belief in spirits, possession and witchcraft is believed to be small, but where it occurs it causes much distress and suffering to the child.
There are some common features where faith or belief is a factor in abuse.
Firstly, there is sometimes a wider social or community consensus that witchcraft, for example, actually exists. Sometimes a faith leader or other influential figure is at the centre, promoting the belief and methods of resolving the supposed problem by harming children. Parents or carers have also been key perpetrators in many of the known cases. This can make the abuse harder to find out about, harder to get evidence to prosecute and harder to prevent in future.
There is also the internal logic of the belief, which in the case of spirit possession, for example, is that the child is the victim of a supernatural force and the abuse is therefore understood by perpetrators as a means of saving the child – driving out the devil – in other words perpetrators may perversely believe that they are doing the right thing. Even where there is no intention to save the child, the belief that the child can harm others can generate a real fear in those who would normally be expected to protect the child, including parents or close family. This fear that a child may cause harm to, or kill, siblings, parents and other family or friends can be a critical factor in the abuse.
In some cases, there are also real-world factors underlying the abuse. This is sometimes described as the scapegoating of children to reconcile misfortune that has occurred to the family or community, such as an adult family member becoming unemployed or being in poverty. In these situations, those who are different because they have some special traits (such as being particularly bright, having difficult behaviour, having a disability or children living away from their parents) are the target of scapegoating, being accused of having caused the misfortune by supernatural means. The most vulnerable people within a group offer the least ability to resist being scapegoated, and children are a group who are inherently vulnerable, needing protection from adults around them.
Standard safeguarding procedures apply in all cases where abuse or neglect is suspected to be related to particular belief systems.
Where there is a risk of significant harm to a child, a referral should be made to children’s social care and safeguarding processes engaged (see Referrals chapter). The police should also be notified in order to engage with multi-agency safeguarding procedures and to investigate possible criminal offences.
Action must be taken to assess and address the child’s health needs as this form of abuse can involve physical abuse such as physical restraint and assault and less visible abuse such as forcing the child to drink harmful ‘potions’.
Victims of this crime are left scarred (often mentally and physically) by their experiences. Often young and vulnerable to start with, victims suffer from abuse at the hands of those they may be expected to trust. Those children may also share a belief in the supernatural with their abuser including that they are, or are possessed by, an evil force.
They are likely to require ongoing support to help them to make sense of and recover from their experiences.
RELATED GUIDANCE
Independent Sexual Violence Adviser Statutory Guidance (Ministry of Justice)
National Audit on Group-based Child Sexual Exploitation and Abuse (Casey, 2025)
Responding to Child Sexual Exploitation (College of Policing)
Key Messages from Research (Centre of Expertise on Child Sexual Abuse)
January 2026:
Information has been added on Independent Sexual Violence Advisers and a link added to Independent Sexual Violence Adviser Statutory Guidance. See Section 9.
CONTENTS
Guidance – Child Sexual Exploitation: Definition and Guide for Practitioners (Department for Education) and Working Together to Safeguard Children (Department for Education) define child sexual exploitation (CSE) as a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity:
The victim may have been sexually exploited even if the sexual activity appears consensual. CSE does not always involve physical contact; it can also occur through the use of technology, including artificial intelligence (‘AI’). See also Internet Safety / Online Safety.
Like all forms of child sexual abuse, CSE:
Even where a young person is old enough to legally consent to sexual activity, the law states that consent is only valid where they make a choice and have the freedom and capacity to make that choice. If a child feels they have no other meaningful choice, are under the influence of harmful substances or fearful of what might happen if they do not comply (all of which are common features in cases of child sexual exploitation) consent cannot legally be given whatever the age of the child.
One of the key factors found in most cases of CSE is the presence of some form of exchange (sexual activity in return for something) for the victim and / or perpetrator or facilitator.
Where it is the victim who is offered, promised or given something they need or want, the exchange can include both physical rewards (such as money, drugs or alcohol) and psychological rewards (such as status, protection or perceived receipt of love or affection). It is important to remember the unequal power dynamic within which this exchange occurs and to remember that the receipt of something by a child / young person does not make them any less of a victim. It is also important to note that the prevention of something negative can also fulfil the requirement for exchange, for example a child who engages in sexual activity to stop someone carrying out a threat to harm their family.
Many children who are sexually exploited may have been victims of other forms of abuse; the grooming methods that may be used can mean that children who are sexually exploited do not always recognise they are being abused, which can also affect detection rates. What is clear is that child sexual exploitation can occur in all communities and amongst all social groups and can affect girls and boys. All practitioners should work on the basis that it is happening in their area.
Any child, in any community: All practitioners should be open to the possibility that the children they work with might be affected.
Age: Children aged 12-15 years of age are most at risk of CSE although victims may be much younger, particularly in relation to online concerns. Equally, those aged 16 or above can also experience CSE, and it is important that such abuse is not overlooked due to assumed capacity to consent. Account should be taken of heightened risks amongst this age group, particularly those without adequate economic or systemic support.
Gender: Though CSE may be most frequently observed amongst young females, boys are also at risk. Practitioners should be alert to the fact that boys may be less likely than females to disclose experiences of child sexual exploitation and less likely to have these identified by others.
Ethnicity: CSE affects all ethnic groups.
CSE is often linked to other issues in the life of a child or young person, or in the wider community context. Practitioners should be alert to the fact that CSE is complex and rarely presents in isolation of other needs and risks of harm (although this may not always be the case, particularly in relation to online abuse). CSE may be linked to other crimes and practitioners should be mindful that a child who may present as being involved in criminal activity is actually being exploited.
CSE can have links to other types of crime. These include:
The following vulnerabilities are examples of the types of things children can experience that might make them more susceptible to CSE:
Not all children and young people with these vulnerabilities will experience child sexual exploitation. CSE can also occur without any of these vulnerabilities being present.
The vulnerability of many victims makes them particularly susceptible to the grooming tactics used by offenders. Most victims are groomed to a certain extent by their exploiter, who will use various persuasive methods to control them and keep them in exploitative situations. This may include encouraging the victim to play a participatory role in the production of indecent images and / or to recruit other victims to participate in the activity.
Offenders exploit their victims further by creating or exacerbating vulnerabilities that they have in order to retain control over them. Vulnerabilities include disengagement from friends and family, detachment from services and challenging or criminal behaviour.
The following methods can also be used to coerce a victim:
This is not an exhaustive list and not all the methods listed will be used or occur in the order above.
Children are often reluctant to disclose experiences of exploitation for a variety of reasons including:
It is important that practitioners are aware of potential indicators of risk, as categorised in responding to Child Sexual Exploitation (College of Policing), summarised in Section 5.
Signs include:
Signs include:
Signs include:
Signs include:
Signs include:
Practitioners should also remain open to the fact that CSE can occur without any of these risk indicators being obviously present.
The first step for practitioners is to be alert to the potential signs of abuse and neglect. Those working with children and families should access training to support them in identifying vulnerability, risk and harm.
Child sexual exploitation can take place in a variety of ways. Responding to Child Sexual Exploitation (College of Policing) lists examples, but practitioners should note that this is not intended to be exhaustive and should be aware of this form of exploitation.
The act of CSE is generally a hidden activity and is much more likely to occur in private dwellings than in public venues. Technology can be used to facilitate sexual exploitation of children. This can include social networking tools and platforms, chat rooms, dating sites, online gaming, GPS technology to track locations and sharing of abusive images online. See also Internet Safety / Online Safety chapter.
The following examples describe different types of exploitation which offenders use and how children can be coerced.
Inappropriate relationships: These usually involve one offender who has inappropriate power or control over a young person (physical, emotional or financial). One indicator may be a significant age gap. The young person may believe they are in a loving relationship.
Boyfriend / girlfriend model: Here the offender befriends and grooms a young person into a ‘relationship’ and then coerces or forces them to have sex with friends or associates. The boyfriend/girlfriend may be significantly older than the victim, but not always.
Gang-associated CSE: A child or young person can be sexually exploited by a gang, but this is not necessarily the reason why gangs are formed. Types of exploitation may include using sex as a weapon between rival gangs, as a form of punishment to fellow gang members and / or a means of gaining status within the hierarchy of the gang. Where abuse takes place in a gang environment, female members may perceive the abuse as normal, as well as accepting it as a way of achieving a respected status / title within the gang.
Organised / networked sexual exploitation or trafficking: Involves people who come together in person or online for the purpose of setting up, co-ordinating and / or taking part in the sexual exploitation of children in either an organised or opportunistic way. Young people (often connected) may be passed through networks, possibly over geographical distances, between towns and cities where they may be forced / coerced into sexual activity with multiple men. Often this occurs at ‘parties’, and young people who are involved may recruit others into the network. Some of this activity is described as serious organised crime and can involve the organised ‘buying and selling’ of young people by offenders. Organised exploitation varies from spontaneous networking between groups of offenders, to more serious organised crime where young people are effectively ‘sold’. Organised sexual exploitation and / or trafficking by groups is a sophisticated and complex area of CSE.
Peer-on-peer abuse: When a young person is exploited by their peer/s, the abuser is the same age, or close in age to them. At the very least, everyone directly involved in the abuse is under 18 years of age. They are forced or coerced into sexual activity by their peers or associates. Sometimes this can be associated with gang activity but not always. Many of the warning signs and indicators of CSE tend to refer to adult perpetrators, for example, associations with older boyfriends / girlfriends, relationships or associations with risky adults and / or entering or leaving vehicles driven by unknown adults. In peer-on-peer exploitation, schools and youth clubs are also locations where children and young people can be exploited. To help disrupt cases of peer-on-peer exploitation, consideration may need to be given to:
Repeat victimisation: There are some features of repeat victimisation of CSE victims which are distinctive. CSE victims may return to perpetrators for a range of reasons, for example, as a result of grooming, out of fear, drug addiction, needing accommodation, out of a sense of loyalty or perceived affection towards their perpetrators.
Children can be both experiencing child sexual exploitation and perpetrating it at the same time. Examples might include a child who is forced to take part in the exploitation of another child under duress, or a child who is forced to introduce other children to their abuser under threats to their family’s safety. These situations require a nuanced approach that recognises and engages with the young person’s perpetration within the context of their own victimisation.
Children who perpetrate child sexual exploitation require a different response to adult perpetrators. Responses may involve criminal justice pathways at times, however every child who displays harmful sexual behaviour should also have their safeguarding and welfare needs actively considered.
Different agencies should work together to:
Where practitioners have concerns that a child is a victim of sexual exploitation, they should discuss with their safeguarding lead. Where it is suspected that the child is at risk of significant harm, a referral should be made to children’s social care and safeguarding processes engaged which may include a multi-agency strategy discussion (see Referrals and Strategy Discussions chapters). Where there is an imminent risk of significant harm, steps must be taken to ensure the child’s immediate safety (see Immediate Protection chapter).
The police should be informed where there is a known or suspected criminal offence. They will be able to advise on issues such as:
In addition to the usual safeguarding processes set out in the Providing Help, Support and Protection section of this site, the following points should be considered in relation to situations involving CSE.
The exploitation of children cannot be addressed by a single agency working alone. Effective collaboration between partners, particularly around information sharing, is essential to the protection of children and stopping offenders. There is a wide range of behaviours and scenarios that may not initially appear related to CSE, but pieced together and put into context, form a bigger picture. Agencies hold different pieces of information and will possess different legislative powers that together help to identify the most appropriate tool for keeping children safe.
The safeguarding response should be collaborative and multi-agency and be underpinned by effective information-sharing. It should encompass preventative, protective (immediate safeguarding) and responsive approaches, and should provide help and ongoing support that is responsive to individual need, strengths-based in approach and available over the longer-term (recognising that disclosure, resilience-building and recovery can take time).
It is important that continued contact by the victim with the perpetrator(s) is not misinterpreted as informed choice or an indication of absence of harm. Practitioners should maintain their relationships with children and young people, and continue to exercise professional curiosity and create safe spaces for disclosure. Continued contact with perpetrators should be seen as part of the complex power dynamic of the abusive relationship, similar to that in some situations of domestic abuse. Practitioners should continue to reach out to victims and not make the offer of services dependent on formal disclosure. Many victims are only able to disclose after the provision of support, often months or even years down the line.
It is vital that people working in frontline roles effectively identify exploitation of children and work together proactively with other agencies to disrupt offending and safeguard victims. This can only be achieved by effective joined-up working and consistent, proactive, sharing of information held by different services. Criminal investigation and prosecution of perpetrators should always be pursued alongside actions to support safeguarding of children and young people exposed to this kind of harm.
Cases of child sexual exploitation frequently cross local authority, police force and even country boundaries in terms of the movement of both perpetrators and victims.
The timely and effective sharing of information can assist in early identification of sexually exploited young people. Concerns which initially appear to be of a low level when viewed in isolation may be escalated when considered alongside what is known by other agencies. For instance, visits to sexual health services or school nurses may coincide with young people going missing or returning from being missing. Sharing information can enhance decision making by professionals and more holistic needs assessments. At the same time, sharing information in multi-agency contexts cannot be viewed as an intervention in and of itself; it must be linked to protective and / or preventative action. See also Tier 1 – Children Safeguarding Data Sharing Agreement (DSA) and Data Protection chapter.
Practitioners should not rely on ‘checklists’ alone but should make a holistic assessment of vulnerability, examining risk and protective factors. Risk assessments should cover different types of sexual exploitation including face-to-face perpetration by adults and also other scenarios such as online or peer perpetrated forms of harm. It is also important to remember that risk assessments only capture risk at the point of assessment and that levels of risk vary over time. See also Assessments chapter.
Orders such as Sexual Harm Prevention Orders and Sexual Risk Orders can be used to help disrupt the exploitation of children and young people, as outlined below.
Sexual Harm Prevention Orders (SHPOs) can be made in respect of a person convicted of or cautioned for a sexual or violent offence, including where offences are committed overseas. The court must be satisfied that the order is necessary for protecting the public (or any particular members of the public) from sexual harm or protecting children from sexual harm from the defendant outside the United Kingdom.
The Order prohibits the defendant from doing anything described in the order and can include a ban on foreign travel.
An Order can have effect for a fixed period (specified in the order) of at least five years, or until further order. Failure to comply with an Order is an offence punishable by a fine and / or imprisonment.
7.5.2 Sexual Risk Order
Sexual Risk Orders (SROs) can be made where a person has done an act of a sexual nature as a result of which there is reasonable cause to believe that it is necessary for such an order to be made, whether or not they have been convicted. (This is different to a SHPO). The court must be satisfied that the order is necessary for protecting the public, or any particular members of the public, from sexual harm from the defendant; or protecting children or vulnerable adults generally, or any particular children or vulnerable adults, from sexual harm from the defendant outside the United Kingdom.
The Orders prohibit the defendant from doing anything described in the order, and can include a ban on foreign travel. An Order has effect for a fixed period, specified in the order, of not less than two years, or until further order. Failure to comply with an Order is an offence punishable by a fine and / or imprisonment.
See also Guidance: Child Exploitation Disruption Toolkit (Home Office)
The harmful effects of child sexual exploitation are serious and far reaching for victims, their families and wider communities. Local multi-agency work should be undertaken aimed at prevention and protecting children and young people through awareness raising, including:
Local multi-agency work should aim to:
Although messages and methods of delivery will vary according to the nature and needs of the audience, all education and awareness raising initiatives should:
Independent Sexual Violence Advisers (ISVAs) provide independent support to victims / survivors of sexual offences.
Children and Young Persons ISVAs (CHISVAs) support children and young people who have experienced sexual violence and sexual abuse.
They can:
They provide support regardless of whether a victim / survivor has chosen to report an offence to the police, whether a criminal case has ended or whether they are victims of multiple offences.
A victim / survivor can be referred into the ISVA service at any time, by any professional engaging with them. Some ISVA services accept self-referrals by victims themselves.
See also Independent Sexual Violence Adviser Statutory Guidance (Ministry of Justice)
CONTENTS
Revelations of widespread abuse and neglect of children living away from home have done much to raise awareness of the particular vulnerability of children in these circumstances. It is important for agencies and professionals not to be complacent and to be vigilant at all times so that children in these circumstances do not suffer.
Everywhere that children live should provide the same basic safeguards against abuse, founded on an approach that promotes their general welfare, protects them from harm, and treats them with dignity and respect.
Settings where children are living away from home include: boarding schools, children’s homes and foster homes, hospitals, prisons, young offender institutions, secure training centres, secure units and army bases. This guidance is also relevant in relation to private fostering and foreign exchange visits. The same consideration should be given to children from other local authorities who may be temporarily living in Buckinghamshire, as well as children from Buckinghamshire who are temporarily living in a different local authority.
The Buckinghamshire Safeguarding Children Partnership (BSCP) Safeguarding Children Procedures apply in every situation and to all settings, including those where children are living away from home.
Individual agencies that provide care for children living away from home should implement clear and unambiguous procedures to respond to potential matters of concern about children’s welfare, in line with the relevant legal requirements.
Children living away from home are particularly vulnerable to being abused by adults and peers. With limited and sometimes controlled contact with family and carers, they may not be able to disclose what is happening to them. Many young people live away from home because of concerns of abuse and/or exploitation. It is particularly important therefore that their welfare is protected when they are being cared for by another agency, institution or family.
Disabled children are particularly vulnerable when living/staying away from home.
All settings must ensure that:
There should be clear procedures and support systems in place for dealing with expressions of concern about staff or volunteers (see Allegations against those Working with Children / People in Positions of Trust). Organisations should have a whistleblowing policy and code of conduct instructing staff and volunteers on their duty to their employer and their professional obligation to raise legitimate concerns about the conduct of colleagues or managers. There should be a guarantee that procedures can be invoked in ways that do not prejudice the whistleblower’s own position and prospects (see also Whistleblowing).
Complaints procedures and safeguarding children policies should be kept up to date. These must be clear, effective, user-friendly and readily accessible to children and young people, including those with disabilities and those for whom English is not their preferred language.
Children should genuinely be able to raise concerns and make suggestions for changes and improvements, which should be taken seriously. Procedures should address informal as well as formal complaints. Systems that do not promote open communication about ‘minor’ complaints will not be responsive to major ones, and a pattern of minor complaints may indicate more deeply rooted problems in management and culture that need to be addressed.
When there are concerns about significant harm to a child, the same safeguarding children procedures apply as for those children who live with their own families.
Children and young people living in foster care or residential settings are among the most socially excluded groups. They are vulnerable to abuse, and may be in care due to abuse. or neglect they have experienced.
BCSP expects there to be a strong working partnership between all key people and agencies involved in the child’s life, to enable clarification and allocation of the different roles and responsibilities as ‘public’ parents, to ensure the child is kept safe. This includes the child/young person and their family, as well as the day-to-day carers and others who have a role to play.
Where there is reasonable cause to believe that a Child Looked After has suffered, or is likely to suffer, significant harm in their placement, Children’s Social Care will convene a strategy meeting involving all relevant partners.
In these circumstances, enquiries should consider the safety of any other children living in the foster home/residential setting, including the foster carers’ own children, grandchildren or any children cared for by the foster carers in their home, as well as any children whom the foster carers may be caring for or working with outside their home in a voluntary or paid capacity, e.g. teaching, faith or youth work, scouts or other groups.
Social workers are required to see Children Looked After on their own and evidence of this should be recorded on the child’s records. The role of the Independent Reviewing Officer (IRO) includes ensuring they have the opportunity to see the child prior to reviews, and speak to them on their own, when age and developmentally appropriate. This is in addition to seeing them at other times, and to ensuring the child has contact information for their IRO.
Children Looked After who have learning and/or behavioural difficulties and/or sensory/physical impairment are particularly vulnerable to abuse. Staff working with these children must be alert to any signs that a child might be in need of protection.
Throughout any period of being looked after, the child must be made aware of their rights under the Children Act 1989 and 2004. Children and young people have a right to be heard. They can best describe how it is for them because they know how it feel. Children and young people have a right to free expression on matters that affect them. Their views should be respected and should be given due weight in accordance to their age and maturity.
On becoming looked after, children and young people must be provided with information about the services provided in Buckinghamshire. All staff and social workers should also be briefed about these services during their induction.
Private fostering is when a child or young person under 16 (or under 18 if disabled) is living with someone who is not a close relative (i.e. grandparent, aunt, uncle, brother or sister) for 28 days or more. This may include children sent from abroad, asylum-seeking and refugee children, teenagers with short-term arrangements with friends or other non-relatives, and language students with host families.
There are procedures in relation to private fostering which must be followed (see Buckinghamshire County Council’s Private Fostering Procedures). Any professional who becomes aware that a child is in a private fostering arrangement should notify Buckinghamshire County Council Children’s Social Care.
Under the Children Act 1989, private foster carers and those with parental responsibility are required to notify Buckinghamshire County Council of their intention to privately foster or have a child fostered.
Children’s Social Care must satisfy themselves as to the suitability of the private foster carer, their household and accommodation.
Children on foreign exchange visits/homestays typically stay with a family selected by the school in the host country. Where this is for a period of less than 28 days, they are not classed as being ‘privately fostered’. In these circumstances, the only agency involved is education, with the school making arrangements to select host families and to negotiate the provision of families abroad. Where the stay exceeds 28 days, for children staying in the UK this will be considered a private fostering arrangement and the guidance in Section 3.2 should be followed.
In the event that any child in a household is subject to a Child Protection Plan or is the subject of a Section 47 Enquiry, the household should (until there is a satisfactory resolution of concerns) be regarded by the school as unsuitable to receive a pupil from an overseas school.
Disclosure and Barring Service (DBS) regulations do not apply to UK-based exchange visits of less than 28 days, but overseas parents should indicate that they consent to the suitability of the selection process that places their child with the volunteer host family.
A DBS check in itself is no guarantee as to the suitability of an adult to work with any given group of young or vulnerable people. The placement of an adult within a situation of professional trust (where young people could be vulnerable to physical or mental exploitation, abuse or grooming) should be based on a common-sense assessment of the risk-benefit.
Visit leaders should ensure that parents/carers understand that DBS checks are unlikely to be available in countries visited by young people from the UK. They therefore must ensure that the overseas host school or agency is aware of the need to plan for appropriate home placements. In practical terms, this will mean schools are guided by the host teacher’s knowledge of their pupils and their families. There is thus an understanding/mutual trust between families sending pupils to stay with an overseas host family.
The visit leader should ensure that:
The National Service Framework for Children, Young People and Maternity Services (NSF) sets out standards for hospital services. Hospitals should be child-friendly, safe and healthy places for children, with care in an appropriate location and environment.
Children under 16 should not usually be cared for on an adult ward, although if they are aged 14 or over they may be given a choice as to whether they wish to be cared for on an adult ward. Hospital admission data should include the age of children so that hospitals can monitor whether children are being given appropriate care on appropriate wards. For further information refer to the National Institute for Health and Care Excellence (NICE) recommendations.
Children’s Social Care must be notified by the hospital if a child is in hospital for more than 12 weeks. Children’s Social Care must then carry out an assessment of the child’s welfare and safety (as per Section 85 of the Children Act 1989).
The hospital should inform the parents/carers of the child that the information will be shared with Children’s Social Care and the reasons for this.
Best practice is that notifications should be received at least three weeks before a child has been away from home for the statutory period of 12 weeks so that the Children’s Social Care assessment remains within timescales.
There will be occasions when children are staying in a hospital outside of the local authority where they normally live, especially where they are receiving treatment from specialist units. In such cases, hospital staff should ensure there is relevant communication and liaison with professionals in the child’s home authority, including with Children’s Social Care where a notification under Section 85 of the Children Act needs to be made.
The local authority has the same responsibilities towards children in custody as it does for other children in the local authority area.
Under the Legal Aid Sentencing and Punishing of Offenders Act 2012, children are remanded to the care of the local authority and are managed within Children Act Statutory Guidance; Care planning, placement and case review.
Young Offenders Institutions which accommodate juveniles (16–18-year-olds) must have policies and procedures in place which set out their duties to safeguard and promote the welfare of the children and young people in their care.
Specific institutions in an area must ensure that there are links in place with the local Safeguarding Children Partnership and local authorities.
There are currently no Young Offender Institutions in Buckinghamshire which accommodate juveniles.
The age of criminal responsibility in England and Wales is 10 years old. This means that any person over this age can be arrested and detained if they commit a criminal offence. There are strict and complex rules governing the arrest of children set out in the code of practice in the Police and Criminal Evidence Act 1984. The police should generally only arrest children where they need to do so to preserve and secure evidence.
The police recognise that the custody environment is not usually the most appropriate place for young people to be dealt with. However, where it is necessary for a young person to be held in custody, they should generally be held for the shortest time possible.
There is a presumption in favour of bail in all cases, and this is even stronger in the case of young people. However, sometimes young people commit extremely serious offences and there will be occasions where it is necessary to remand a young person in custody. When a young person has been remanded, arrangements must be made for their transfer to local authority accommodation, unless the custody officer produces a certificate stating why this was impracticable, or in certain cases where secure accommodation was required but was not available.
Children may be at risk of harm when they are living in temporary accommodation that also houses adults, for example B&Bs, hostels or refuges.
Placement in temporary accommodation, often at a distance from previous support networks or involving frequent moves, can lead to individuals and families falling through the net and becoming disengaged from health, education, social care and welfare support systems. Some families who have experienced homelessness and are placed in temporary accommodation by local authorities under the main homeless duty can have very transient lifestyles. See Local Transfer Protocol.
It is important that effective communication and systems are in place to ensure that children from homeless families receive services from health and education, as well as any other relevant services.
There will be additional challenges where temporary accommodation is provided in another local authority. In such cases the services involved with the family should take extra care to ensure there is good communication and that relevant services are continued.
There is statutory guidance on making arrangements under section 11 of the Children Act 2004 to safeguard and promote the welfare of children, which sets out local authorities’ responsibilities for homeless families.
In relation to homeless 16 and 17 year olds, the Joint Protocol for Homeless 16 and 17 Year Olds (opens as a PDF) should be followed. This sets out the responsibilities for Buckinghamshire Council.
RELATED GUIDANCE
CONTENTS
Where the local authority plan to return a child to the care of their family, an assessment should be carried out while the child is looked after as part of the care planning process (under regulation 39 of the Care Planning Regulations 2010).
This assessment should consider what services and support the child and their family might need once the child ceases to be looked after. Family group decision-making, such as family group conferences, can be used to establish how the family network will support the child to return home. The outcome of this assessment should be included in the child’s care plan.
The decision to cease to look after a child will, in most cases, require approval under regulation 39 of the Care Planning Regulations 2010. Practitioners must carry out an assessment of need for eligible children to consider their eligibility for independence and transition into adulthood.
There should be a clear plan for all children who return home that reflects the current and previous assessments, focuses on outcomes, and includes details of services and support required. Following the child’s return home:
The impact of services and support should be monitored and recorded, and where a child is remanded to local authority or youth detention accommodation, consideration must be given to what ongoing support and accommodation the child may need after their period of remand. This should be included in their care plan.
Where a child who is accommodated under section 20 of the Children Act 1989 returns home in an unplanned way, (for example, the decision is not made as part of the care planning process, but the parent removes the child, or the child decides to leave), the local authority should work with partner agencies to consider whether there are any immediate concerns about the safety and wellbeing of the child. This could include harm from outside the home. The local authority should take appropriate action, including considering making enquiries under section 47 of the Children Act 1989, if there is concern that the child is suffering or likely to suffer significant harm (see Section 47 Enquiries chapter).
RELEVANT CHAPTERS
Unaccompanied Asylum Seeking Children
Multi-Agency Child Exploitation Protocol
RELATED GUIDANCE
CONTENTS
Evidence from research demonstrates that a significant proportion of children who go missing are at risk of serious harm. There are links between going missing and a number of different risk factors. For example, there are particular concerns about the links between children going missing and the risks of exploitation (criminal and sexual), especially for looked after children (LAC) who go missing from their placements. Other risks and vulnerabilities include, but are not limited to, trafficking, forced marriage, radicalisation and involvement in gangs.
This guidance is relevant for all agencies working in Buckinghamshire in cases where children go missing from either home, care or education. It is designed to ensure that when a child goes missing there is an effective and coordinated safeguarding response from all agencies involved. In particular:
This guidance should be read in conjunction with the Statutory guidance on children who run away or go missing from home or care (Department for Education).
The following safeguarding principles should be adhered to in relation to identifying and locating children who go missing:
All practitioners working with children at risk of going missing should discuss the dangers relating to this with the child and, if appropriate, their family. They should be told about support services and this should include information about helplines.
Anyone whose whereabouts cannot be established will be considered as missing until located and their well-being or otherwise confirmed.
All reports of missing people sit within a continuum of risk from ‘no apparent risk (absent)’ through to high-risk cases that require immediate, intensive action.
| No apparent risk (absent) | |
| There is no apparent risk of harm to either the subject or the public. | Actions to locate the subject and/or gather further information should be agreed with the informant and a latest review time set to reassess the risk. |
| Low risk | |
| The risk of harm to the subject or the public is assessed as possible but minimal. | Proportionate enquiries should be carried out to ensure that the individual has not come to harm. |
| Medium risk | |
| The risk of harm to the subject or the public is assessed as likely but not serious. | This category requires an active and measured response by the police and other agencies in order to trace the missing person and support the person reporting. |
| High risk | |
| The risk of serious harm to the subject or the public is assessed as very likely. | This category almost always requires the immediate deployment of police resources – action may be delayed in exceptional circumstances, such as searching water or forested areas during hours of darkness.
There should be a press/media strategy and/or close contact with outside agencies. Although please note that caution must be exercised when making decisions on whether to use media appeals, as sometimes children who are the victims of exploitation may be at increased risk in relation to gang involvement. Children’s services must also be notified immediately if the person is under 18. |
Thames Valley Police will not categorise the following as ‘no apparent risk’; they will always be the subject of a missing person investigation:
Professionals or others reporting a child missing to the police should not make a judgement about the level of risk. This decision will be made by the police on the basis of the information provided.
Children of compulsory school age who are not registered pupils at a school and are not receiving suitable education otherwise than at a school. Children missing education are at significant risk of underachieving, being victims of harm, exploitation or radicalisation, and becoming NEET (not in education, employment or training) later in life.
Children missing education should not be confused with children missing from. These are children who run away from school, or have missing episodes during the time they should be at school.
Parents and those with parental responsibility are normally expected to have undertaken the following basic measures to try to locate the missing child, if considered safe to do so. Anyone else who has care of a child without parental responsibility should take all reasonable steps to locate the child and ascertain their safety. Professionals working with families should support parents and carers in taking the following necessary steps;
At the point where a parent / person with parental responsibility consider the child to be missing, they should inform the police without delay.
When reporting a child missing to the police any relevant information that might help find or support the child should be shared, including;
Anyone who has care of a child without parental knowledge or agreement should do what is reasonable to safeguard and promote the child’s welfare. In these circumstances, they should inform the police, Children’s Social Care and the parents of their whereabouts and safety. If this is not complied with, the police should consider advice or warning under the Child Abduction Act (1984), if appropriate.
The police are the lead agency for investigating and finding missing children. However, some missing children who have not been reported to the police may come to the attention of agencies. Agencies should work with families to help them recognise the risks associated with a child going missing and the importance of reporting this to the police.
When Thames Valley Police receives a report that a child is missing, they will determine the level of risk based on the answers to 10 standard risk assessment questions:
The person reporting a missing child to the police should provide the police with up-to-date information to inform decision making, as well as details of any action they have taken to trace the missing child.
When accepting a missing person report, the police will advise the caller that they will share information about the missing child and seek assistance from partner agencies to find the child. They will presume that all missing children are vulnerable unless a risk assessment determines otherwise. The police have the ultimate responsibility for determining the action that needs to be taken and when it needs to be escalated.
The continued response and classification of a child as missing is based on on-going risk assessment and undertaken in line with current police guidance.
If a child is risk assessed to be recorded as ‘no apparent risk’, their details will be added to the Police National Computer (PNC) and an appropriate call-back time agreed with the caller. This will be dependent upon the risk assessment, and will remain subject to constant review in light of new information and changing circumstances. When the call back time is reached, the police will call the reporting person and review the 10 questions. If at that time, or earlier, there is information to indicate a higher or increased level of risk, the police will change the status of the missing child and officers will be deployed to commence a missing person investigation.
Where the police have risk assessed a missing child to be ‘no apparent risk, it will be the responsibility of the reporting person to collect the child and establish the reasons behind their absence once they are located. The police will not conduct a safe and well check unless crimes or other safeguarding issues are suspected.
Where risk is identified, either to the missing child or to the public, as a result of responses to the standard risk assessment questions, the police response will be determined by the identified level of risk (see risk assessment table above). A police officer will visit the reporting person and commence a missing person investigation.
A missing child would be prioritised as ‘high risk’ where:
All high risk cases will be led by a senior police officer.
Police officers will:
The police will undertake a secondary investigation to identify any incidents or issues which may inform the risk assessment or help locate the child more quickly, e.g. domestic violence, child protection reports, the child is in care, potentially at risk from child exploitation or another crime, or particularly vulnerable for any reason. Police should consider contacting Children’s Social Care and the risk assessment must be continually reviewed.
In some cases, the police may feel it is necessary to publicise information relating to a missing chid via the media. They may also utilise the website facility of the UK Missing Person’s Unit.
The police may also utilise ‘Text Safe’ as this provides a way of proactively texting a missing person’s mobile phone with a message from Missing People about the service. This lets the missing person know that we care for their safety and want to help, and encourages them to get in touch.
The police are responsible for liaising with the family as well as with other agencies and force areas. If the child is in care, it may be more appropriate for Children’s Social Care to undertake enquiries with the family and other agencies, and report their findings back to the police. This approach should be decided on a case-by-case basis.
The local Police Missing Person Co-ordinator is the single point of contact for all agencies. Out of weekday office hours the local Duty Inspector is the contact. Both can be contacted via 101.
A missing child would be prioritised as ‘medium risk’ where the risk of harm to the subject or the public is assessed as likely but not serious. This category requires an active and measured response by the police and other agencies in order to trace the missing person and support the person reporting. This will involve a proactive investigation and search in accordance with the circumstances to locate the missing child as soon as possible.
In cases where the report is initially made to Children’s Social Care the child of concern should still be referred to the police on 101. In cases where the report to Children’s Social Care was from a third party, there should be agreement, informed by risk assessment, about who makes this report.
All missing persons are reviewed by the Duty Shift Inspector during their tour of duty. Any child who is missing will be referred by the police to Children’s Social Care within 24 hours.
Children’s Social Care must be notified immediately in the case of any high risk missing children.
Where a child discloses a safeguarding issue, there are concerns about a child’s vulnerability or that the child may be at risk of significant harm, the police should make a referral to Children’s Social Care as soon as this becomes evident.
If the child has been missing for more than 24 hours, the case will be reviewed at the police daily management meeting.
In all high-risk cases, or once a child has been missing for over 24 hours, the police, in consultation with partner agencies, must consider a media strategy, although as stated previously, caution must be exercised as in some cases a media appeal could increase the risk to the child. Each case to be treated on its own merits. Such an approach is not routine but is usually a response to very serious concerns for the child’s safety. Either carers or the police may suggest such an approach. Normally, such decisions to publicise will be made jointly, and where appropriate, in consultation with parents and Children’s Social Care. However, for operational reasons primacy over such decisions must lie with the police.
When a child deemed to be medium risk has been missing for more than 48 hours, the case will be reviewed by a Detective Inspector.
All missing persons are notified to the UK Missing Person’s Unit (National Crime Agency) after 48 hours, or earlier if the child is at high risk of harm.
When a child has been missing for over three days, Children’s Social Care will convene a strategy meeting. Children’s Social Care will call a strategy meeting sooner if they consider the child is likely to suffer significant harm. The meeting will review:
Further reviews will take place at least every five days thereafter or earlier, if deemed appropriate.
If the child has been missing for more than 10 weeks, the Missing Person Co-ordinator will ask for the PNC entry to remain in place for up to a year.
Section 13 Children Act 2004 requires local authorities and other named statutory partners to make arrangements to ensure that their functions are discharged with a view to safeguarding and promoting the welfare of children. This includes planning to prevent children from going missing and to do everything possible to ensure their safe return when they do go missing.
The Local Authority should have a named senior manager within Children’s Services who is responsible for monitoring policies and performance relating to children who go missing from home or care.
The Local Authority must ensure that all incidents where children go missing are appropriately risk assessed, and should record all incidents of looked after children who are missing or away from placement without authorisation.
Children who are looked after should have information about and easy access to help lines and support services including emergency accommodation. Support should also be made available to families to help them understand why the child has gone missing and how they can support them on their return.
The local authority should consult with the police regarding what action should be taken to share information about a missing child who is looked after, subject to a child protection plan or a child in need. This should include an assessment of whether to release information to the media. The local authority should also notify other local authorities according to the degree of concern. Consideration should also be given to whether the child or their family has links to other areas either within the UK or abroad.
On receipt of a notification from another local authority, a flag should be added to the electronic record system for Children’s Social Care and consideration should be given to notifying health and other relevant partners.
In all circumstances where a child goes missing, local safeguarding procedures should be followed. If there is concern that the child may be at risk of significant harm if returned home, a referral should be made to Children’s Social Care so that an assessment can be undertaken and where necessary arrangements made for accommodation.
MACE is a multi-agency risk management meeting that seeks to ensure that children living in Buckinghamshire are effectively safeguarded and protected from harm in cases where:
High risk means the risk posed is immediate and there are substantial grounds for believing that the subject is in danger through their own vulnerability; or may have been the victim of a serious crime; or the risk posed is immediate and there are substantial grounds for believing that the public is in danger.
Repeat missing person means someone who is reported missing three times or more in a 90 day period.
Information is shared between agencies and actions set with the intention of reducing the risk to children, providing early intervention and considering how harmful activities can be disrupted.
MACE does not replace the provisions of Section 17 (Child in Need) or 47 (Child in need of protection) of the Children Act. It compliments statutory processes by helping to ensure that the bigger picture is considered, that action to safeguard is being completed and the appropriate multi-agency response is in place.
See also Multi-Agency Child Exploitation Protocol.
When a 16 or 17 year old goes missing they are no less vulnerable than younger children and are equally at risk, particularly of sexual exploitation or involvement with gangs.
When a 16 or 17 year old presents as homeless, Children’s Social Care must assess their needs as for any other child. Where this assessment indicates that the young person is in need and requires accommodation under Section 20 of the Children Act 1989, they will usually become looked after.
The accommodation provided must be suitable, risk assessed and meet the full range of the young person’s needs. The sustainability of the placement must be considered. Children aged 16 or 17 who have gone missing and are at risk of homelessness may be placed in supported accommodation, with the provision of relevant specialist support. For example, a specialist service might be provided for those who have been sexually exploited, or at risk of sexual exploitation.
Local authorities should have regard to:
Professionals should be aware of the ‘hidden missing’. These are children who have not been reported missing to the police, but have come to an agency’s attention after accessing other services. There may also be trafficked children who have not previously come to the attention of children’s services or the police. Research demonstrates that children from black and minority ethnic groups, and children that go missing from education are less likely to be reported as missing.
Some of the children looked after by the Local Authority may be unaccompanied asylum seeking children or other migrant children. Some children in this group may have been trafficked into the UK and may remain under the influence of their traffickers even while they are looked after. Trafficked children are at high risk of going missing, with most going missing within one week of becoming looked after and many within 48 hours. Unaccompanied migrant or asylum seeking children who go missing immediately after becoming looked after should be treated as children who may be victims of trafficking. See also, Unaccompanied Asylum Seeking Children.
Children who have been trafficked may be exploited for sexual purposes and the possible link to sexual exploitation should be considered. Professionals should also refer to the Multi Agency Child Exploitation Protocol.
The assessment of need to inform the care plan will be particularly critical in these circumstances and should be done immediately, as the window for intervention is very narrow. The assessment must seek to establish
In conducting this assessment, it will be necessary for the Local Authority to work in close co-operation with the UK Human Trafficking Centre and immigration staff who will be familiar with patterns of trafficking into the UK. Immigration staff should be able to provide advice on whether information about the individual child suggests that they fit the profile of a potentially trafficked child.
Provision may need to be made for the child to be in a safe place before any assessment takes place, and for the possibility that the child may not be able to disclose full information about their circumstances immediately. The location of the child should not be divulged to any enquirers until their identity and relationship with the child has been established, if necessary with the help of the police and immigration services. In these situations the roles and responsibilities of care providers must be fully understood and recorded in the placement plan. Proportionate safety measures that keep the child safe and take into account their best interests should also be put in place to safeguard the child from going missing from care or from being re-trafficked.
It will be essential that the local authority continues to share information with the police and immigration staff concerning potential crimes against the child, the risk to other children, or other relevant immigration matters.
Safeguarding Children Who May Have Been Trafficked: Practice Guidance (gov.uk) contains practical guidance for agencies that are likely to encounter children who may have been trafficked.
The NSPCC can provide advice and information to professionals who have concerns that a child may have been trafficked. They can be contacted by telephone on: 0808 800 5000, Monday to Friday 9.30am to 4.30pm or email [email protected].
The National Referral Mechanism (NRM) is the UK’s system for identifying victims of modern slavery and human trafficking. If a first responder has concerns that a child may be a potential victim of modern slavery or human trafficking (including through child criminal exploitation such as county lines and/or child sexual exploitation) then a referral should be made to the NRM, as soon as possible. Specified public authorities (including the police and local authorities) must notify the Home Office about all potential victims of modern slavery in England and Wales. A child’s consent is not needed for a referral to the NRM to be made. In addition to a NRM referral, first responders should also make a referral to children’s social care.
Independent Child Trafficking Guardians (ICTG) are an independent source of advice for children who have been trafficked and somebody who can speak up on their behalf. Where the ICTG service has been implemented, if the first responder considers a child to be a potential victim of modern slavery or human trafficking, they should refer them to the ICTG service. This is in addition to following usual safeguarding routes and NRM referrals. The NRM referral and ICTG referral should be made in parallel.
For further guidance and the online referral forms see: Modern Slavery Victims: Referral and Assessment Forms (gov.uk)
Grooming is when someone builds an emotional connection with a child to gain their trust for the purposes of abuse or exploitation. Children can be groomed online or in the real world, by a stranger or by someone they know – for example a family member, friend or professional. Groomers may be male or female. They could be any age. Many children don’t understand that they have been groomed, or that what has happened is abuse.
Children can be groomed for the purpose of sexual abuse as well as other forms of exploitation including involvement in criminal and extremist activity. Children who are missing are more vulnerable to being groomed and may also go missing as a result of being groomed.
Children can suffer harm when exposed to extremist ideology. This harm can range from a child adopting or complying with extreme views which limit their social interaction and full engagement with their education, to children being groomed for involvement in violent attacks.
Children can by exposed to harmful, extremist ideology in the immediate or extended family, or relatives/family friends who live outside the family home but have influence over the child’s life. Older children might self-radicalise over the internet or through the influence of their peer network – in this instance their parents might not know about this or feel powerless to stop their child’s radicalisation.
Going missing is a risk factor in relation to radicalisation:
CSE is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child under the age of 18 into sexual activity in exchange for something the victim needs or wants, and/or for the financial advantage or increased status of the perpetrator or facilitator.
The victim may have been sexually exploited even if the sexual activity appears consensual. CSE does not always involve physical contact; it can also occur through the use of technology.
Involvement in exploitative relationships is characterised by the limited availability of choice as a result of their social, economic or emotional vulnerability.
A common feature of CSE is that the child does not recognise the coercive nature of the relationship and does not see themselves as a victim of exploitation.
Going missing is a significant risk factor in relation to CSE:
Because there is such a strong link between children going missing and risk of sexual exploitation, professionals should always assess whether a child who has gone missing is being sexually exploited or at risk of being sexually exploited.
Professionals should also refer to Child Sexual Exploitation and Abuse (including Organised Abuse), and can also contact the First Response Team for advice.
Children who go missing from care, home and education also need safeguarding against the risk of being criminally exploited by organised crime groups (OCGs) in relation to the supply of drugs. For example, some children have become involved in what has become known as the ‘county lines’ issue. This involves children being used by gangs to transport and distribute drugs outside of London and other major cities as drug sales operations are expanded into the home-counties and beyond. Involvement in county lines and criminal exploitation places children at increased risk of serious violence.
When a child in care goes missing it is the responsibility of the carer to undertake the basic measures as outlined to try and locate the missing child. When the child is established as missing and the carer contacts the police, it is important that they make it clear that they are reporting the child as missing. In addition to sharing all the relevant information, they should inform the police that the child is in care and under what legal orders. The carer should always ask for, and record, the Police Incident Number.
If a child goes missing out of office hours, the carer should inform the Buckinghamshire Out of Hours Emergency Duty Team (see Local Contacts) and follow their agency’s policies and procedures.
It is important to note that local authorities have very similar duties and responsibilities towards 16 and 17 year old care leavers as they do to children in care and for the purposes of this guidance, the response to a missing care leaver age 16 and 17 year old should be the same.
Local authorities continue to have a range of responsibilities towards children leaving care until the young person’s 21st birthday and in some instances their 25th birthday. It is good practice to follow the guidance set out below whilst a young person remains ‘leaving care’.
Care leavers, particularly 16 and 17 year olds, are vulnerable to sexual exploitation and may go missing from their home or accommodation. Local authorities must ensure that care leavers live in “suitable accommodation” as defined in Section 23B (10) of the Children Act 1989 and Regulations 9(2) of the Care Leavers Regulations. In particular young people should feel safe in their accommodation and the areas where it is located. Local authorities should ensure that pathway plans set out where a young person may be vulnerable to exploitation, trafficking or going missing, and put in place support services to minimise this risk.
When a child is placed out of their local authority area, the host Local Authority must be notified by the allocated social worker in advance of the placement. The responsible authority should seek to ensure that the child has access to the services they need. Any missing report whilst the child is out of county must still be recorded on LCS by the allocated social worker.
It is possible that during a missing episode the child will return to the area of the responsible authority. It is therefore essential that liaison between the police and professionals in both authorities is well managed and coordinated.
This procedure should be followed with additional reference to policies and procedures that apply in the host authority.
Sometimes a looked after child may be away from their placement without authorisation. While they are not missing because their whereabouts is known, they may still be at risk. The carer or social worker should take reasonable steps to ascertain the wellbeing of the child including, when appropriate, visiting the location. However, if there is a concern the child may be at significant risk of harm to themselves or to others then the police should also be notified in order that appropriate safeguarding measures can be taken. This should not be confused with reporting a child missing. Where appropriate, the social worker should consider whether a strategy meeting is required.
Local authorities have a duty to place a looked after child in the most appropriate placement to safeguard the child and minimise the risk of the child going missing. The care plan and the placement plan should include details of the arrangements that will need to be in place to keep the child safe and minimise the risk of the child going missing from their placement.
Where a child already has an established pattern of going missing, the care plan should include a strategy to keep the child safe and minimising the likelihood of the child running away in the future. This should be discussed and agreed as far as possible with the child and with the child’s carers and should include detailed information about the responsibilities of all services, the child’s parents and other adults involved in the family network.
Independent Reviewing Officers (IROs) should be informed about missing episodes and they should address these in statutory reviews.
Designated health professionals for Looked After Children should be informed by the allocated social worker of children missing from care who are deemed to be ‘high risk’. They should be included in any multiagency strategy meetings or activity to manage the child’s retrieval and any subsequent health needs.
Whenever the whereabouts of a looked after child is not known, the foster carer or the manager on duty in the children’s home is responsible for carrying out initial checks to see if the child can be found. For example, if a child was supposed to have returned home from school but has not arrived within the normal journey time, checks could include finding out if there are transport delays, phone calls to the child, phone calls to the school to see if the child has been delayed etc. If these initial checks do not succeed in locating the child or there are still concerns that, despite contact being made with the child they are at risk, the individuals and agencies listed below should be informed.
It is important that a deadline is set at the outset of initial checks so that they don’t continue beyond a reasonable timeframe. What timeframe is reasonable should be based on an assessment of the risks relating to the individual child. In some cases, there might be particular reasons to be worried for the child’s safety immediately and the agencies listed below should be contacted straight away alongside continued attempts to contact the child.
The following individuals and agencies should be contacted when a looked after child is missing:
The carer/s should take all reasonable steps, which a good parent would take, to secure the safe and speedy return of the child based on their own knowledge of the child and the information in the child’s placement plan. If there is suspected risk of harm to the child the carer/s should liaise immediately with the police.
Initial discussions between the allocated children’s social worker and the police should include agreement on an immediate strategy for locating the child. The strategy should incorporate a range of actions to locate and ensure the safe return of the child, and clarity around who will undertake these actions. Aspects to cover in the strategy include:
Within 3 days, a strategy meeting between relevant parties should take place. This should include the police, the child’s social worker and the care provider and other relevant parties. The action plan and risk assessment should be reviewed and updated.
Regular multi-agency meetings should be held at least monthly to update the action plan and share information.
Details of all missing children are shared with senior managers in children’s social care, including the Director of Children’s Social Care, who may request a ‘Need to Know’ form to be completed which is sent to the Corporate Director and used to notify the Lead Member.
Any publicity will be led by the police. The use of harbouring notices etc. will be agreed at the missing from care meeting. Recovery Orders may be used where the child is Looked After.
During the investigation to find the child, regular liaison and communication should take place between the police, Children’s Social Care and any other agencies involved. In the case of a child placed out of area, both the responsible local authority and the host local authority should be involved.
The authority responsible for the child should ensure that plans are in place to respond promptly once the child is found and for determining if the placement remains appropriate.
When a looked after child / care leaver has been located, care staff/ foster carers should promptly inform the child’s social worker and the Independent Reviewing Officer. If the child was not located by the police, then they should also be informed. The police will then arrange a safe and well check and trigger a return home interview.
The attitude of all practitioners towards a child which has been missing can have a big impact on how they will engage with any subsequent investigations and planning. A supportive approach, actively listening and responding to a child’s needs will have a greater chance of preventing the child from going missing again and safeguarding them against any risks.
Children missing from home are subject to risks and vulnerabilities similar to those for children who are looked after.
If the whereabouts of the child are known or suspected, it is the responsibility of the parents or carers to arrange for the child’s return. In exceptional circumstances, in the interests of the safe and speedy return of the child, the police may agree to requests from parents or carers to assist. All agencies need to work together to agree the most appropriate and safe return for the child.
The police will respond to any notifications of children missing from home in line with this procedure and their own procedures.
The usual child protection procedures must be initiated whenever there are concerns that a child who is missing may be suffering or likely to suffer, significant harm. For example:
Where the child meets the criteria for referral to Children’s Social Care, the Local Authority will ensure that an assessment takes place to determine the best course of action.
Where the child is already known to Children’s Social Care (for example they are subject of a child protection plan, or the subject of a Section 47 enquiry) a strategy meeting should be arranged as soon as practicable and within no more than 3 days. Representatives from the Police Missing Persons Unit and the Child Abuse Investigation Unit (CAIU) should attend the strategy meeting, as well as other practitioners involved with the child. If the child has returned prior to the date of the strategy meeting, it is not a requirement for the meeting to go ahead.
A safe and well check will be undertaken by the police as soon as possible and within 24 hours of a child returning from a missing episode. A safe and well check will not be conducted over the telephone. The purpose is to check for any indications that the child has suffered harm; where and with whom they have been; and to give them an opportunity to disclose any offending by, or against them.
Where a child goes missing frequently, it may not be practicable to see them every time they return. In these cases, a reasonable decision should be taken in agreement between the police and their child’s parent or carer, or their Social Worker with regard to the frequency of such checks. Consideration must be given to the link between frequent missing episodes and serious harm.
The assessment of whether a child might go missing again should be based on information about:
If further information comes to light as a result of the safe and well check, where relevant the police will share this information with Children’s Social Care.
If the child makes an allegation of crime that occurred whilst they were missing or that contributed to them going missing, the police will record this allegation and take appropriate action. If it is apparent, upon return, that a child has been the victim of a crime whilst missing, or that there is risk or a crime in relation to the circumstances involved in the missing episode, the police will instigate further enquiries.
In any situation which indicates that the child may have been subject to, or at risk of, significant harm, a referral must be made to Children’s Social Care in accordance with these safeguarding procedures.
Consideration must be given to securing evidence by police including by forensic examination. For sexual offences, professionals should consider an urgent referral to the SARC.
When a child is found they must be offered a return home interview to talk about going missing. Providing children with an opportunity to talk is key to safeguarding them. Return home interviews are designed to support a child in exploring his or her feelings and concerns; it should be gentle and inquisitive, not adversarial or seeking to attribute blame.
Return interviews should be completed by someone independent of their parents or carers. In Buckinghamshire they are usually conducted by staff from Barnardos R U Safe? but on some occasions may also be completed by other agencies. It is important to acknowledge that a returning child may well share different parts of their experience with different people. It is the responsibility of all agencies therefore, to attend to issues of immediate safety, future support and safeguarding needs, and to share relevant information in a way which respects and safeguards children.
The return home interview will be carried out within 72 hours of the child returning to their home or care setting, unless there are exceptional circumstances. The child should be seen on their own unless they specifically request to have someone with them. The child should be offered the option of speaking to an independent representative or advocate.
Where a child is placed out of area, the responsible local authority should ensure the return home review interview takes place, working closely with the host authority where appropriate.
The return home interview and actions that follow from it should:
Where appropriate the return home interview may also gather the views of the parents / carers. Parents and/or carers are sent a letter by R U Safe? following notification of their child going missing. This gives them the opportunity to provide any relevant information and intelligence they may be aware of. This should help to prevent further instances of the child going missing and identify early the support needed for them.
The interview may result in a referral being made to other services that can provide support to meet the assessed needs of the child.
Following a missing episode, Children’s Social Care, the police and other relevant agencies should continue to work together to understand and meet the ongoing needs of the child.
There is a strong link between repeat missing episodes and a risk of significant harm. If a child continually runs away, the actions undertaken following earlier missing episodes need reviewing and alternative strategies considered. This will include a referral to the Missing and Exploitation Hub for high risk missing children or those that go missing more than 3 times in 90 days (see above for further detail).
In the case of children looked after, children’s homes staff and foster carers should be supported to offer a consistent approach to the care of children, including being proactive about strategies to prevent children from running away; and to understand the procedures that must be followed if a child goes missing. There is evidence to show that children in care do not respond to one off or reactive return home interviews as well as children who go missing from home. A more consistent, relationship based approach is often required.
Where a child is, or has been, persistently absent without permission from a children’s home; or is at risk of harm, the children’s home should ask the local authority that looks after the child to review that child’s care plan.
Difficulties can arise when missing children are found but do not want to return. Under the Children Act 1989, where there is reasonable cause to believe that the child could suffer significant harm the police can take the child into Police Protection, and remove to suitable accommodation which could include the home from which the child originally went missing. The police are not given the power to use force to take children into Police Protection. There will be occasions when a child is found in a location that may be considered unsuitable, but where there would not be legal grounds for taking them into Police Protection. In such cases, the police and the accountable manager from the responsible Children’s Social Care will need to liaise to discuss what steps may be necessary in order to safeguard the child’s welfare. Consideration may need to be given to location and recovery orders.
This section should be read in conjunction with the Government’s statutory guidance for children missing education.
Statutory guidance defines children absent from education as those who are not on a school roll or receiving suitable education otherwise than at school. Those who are regularly absent or have missed 10 school days or more without permission may be at risk of becoming ‘children absent from education’. This should be distinguished from children who are missing from school or another form of education.
The Local Authority has a duty under section 436A of the Education Act 1996 to establish (so far as it is possible to do so) the identities of children in our area who are of compulsory school age but who are not registered pupils at a school or receiving some other form of suitable education.
The Children’s Services Protocol for Children Missing Education sets out local arrangements for ensuring all children not receiving a suitable education are identified quickly and effective tracking systems and support arrangements are put in place.
In line with the above Protocol, the Children Absent from Education Officer must be notified after 10 days of any children thought to be absent from education through the following routes:
As a result of daily registration, schools are particularly well placed to notice when a child has gone missing. This section provides guidance for schools where they are concerned that a child has gone missing.
If a member of school/educational establishment/college staff becomes aware that a child may have run away or gone missing, they should try to establish with the parents/ carers, what has happened. If this is not possible, or the child is missing, the designated safeguarding teacher/advisor should, together with the class teacher, assess the child’s vulnerability.
From the first day that a child does not attend school and there is no explanation or authorisation of the absence, the following steps should be taken:
In the following circumstances a referral to Children’s Social Care and /or the police should always be made promptly:
The following questions may assist a judgement on whether or not to inform Children’s Social Care and the police:
If the judgement reached on day one is that there is no reason to believe that the child is suffering, or likely to suffer, significant harm, then the school may delay making a referral to Children’s Social Care. They should continue to make reasonable enquiries to establish what has happened, for example checking with all members of staff the child may have had contact with, checking with the pupil’s friends and their parents, siblings and known relatives.
The length of time that a child remains out of school could, of itself, be an alerting factor of risk of harm to the child. Accordingly the assessment of risk should be ongoing and a referral to Children’s Social Care should be made at any point where there is reasonable cause to believe that the child is suffering or is likely to suffer significant harm. If there is no reasonable cause to believe that the threshold for significant harm has been met, the school should continue to take reasonable action to ascertain the whereabouts of the child, and in line with the Local Authority Protocol for Children Missing Education (CME), a referral should be made to the Children Missing Education Officer after 10 days.
Extended leave of absence can be authorised by the head teacher, at which point a return date is set. In these cases the time line for enquiries starts from when the child does not attend school on the expected return date, not from the day the extended leave started.
The CME team will make enquiries by visiting the child’s home. They should also check databases within the local authority, use agreed protocols to check other relevant local databases, check with agencies known to be involved with the family and with any other local authorities where the family has previously lived or to which the family may have moved.
The child’s circumstances and vulnerability should be regularly and jointly reviewed and reassessed by the school’s designated safeguarding lead and the local authority’s CME Officer. Other agencies should be involved in the discussions as appropriate.
This section applies to children who are ‘subject to restriction’ i.e. who have:
Where the whereabouts of a child subject to restrictions is not known, a missing person’s referral must be made by Home Office staff to the police, the UK Missing Person’s Unit and Children’s Social Care in a number of circumstances including:
If it is believed by Home Office staff that a child is being coerced to abscond or go missing, this must be reported as a concern that the child has suffered or is likely to suffer significant harm to the local police and children’s social care services.
Notifications will also be made where a missing child is found by Home Office staff.
The local authority and health are responsible for:
The police are responsible for:
The local authority will also notify the Home Office Evidence and Enquiry Unit when a child in their care goes missing or when a missing child returns or is found. The Home Office must maintain regular weekly contact with the local authority and the police until the child is found and record all contact with the police and local authority.
When a child subject to restrictions is found by Home Office Staff, the local police and local authority must be informed immediately. In consultation with the local police and Children’s Social Care, a decision will be made as to where the child is to be taken, if they are not to be left at the address where they are encountered. The Home Office must follow up enquires with the local police and children/adult services in order to identify if there are any safeguarding issues.
When a child subject to restrictions is found by the police or local authority, the Home Office must be notified.
RELATED CHAPTER
Tier 1 – Children Safeguarding Data Sharing Agreement (DSA)
RELATED INFORMATION
Sarah’s Law (Child Sex Offender Disclosure Scheme) Thames Valley Police
CONTENTS
The aim of the Child Sex Offender Disclosure Scheme is to provide parents, guardians, and carers with information that will enable them to better safeguard their children’s safety and welfare. It introduced the principle of a two-way disclosure by enabling the public to ask about the history of a person who has access to their child. It enables limited public access to information about registered sex offenders.
Under the Scheme, there is a ‘right to ask’ for information, whereby a person can make an application to the police for information about a person (subject) who has some form of contact with a named child or children. This could include any third party, such as a grandparent, neighbour, or friend; it does not need to be a relative of the child.
‘Contact’ means the person has enough access to a specific child to pose a real risk of harm. For example:
In the event that a subject has convictions for sexual offences against children, poses a risk of causing harm to the child concerned, and disclosure is necessary to protect the child and is a proportionate response to manage that risk, there is a presumption that this information will be disclosed. However, any disclosure under the Scheme will only be made to the person best placed to protect the child. This may not be the individual that made the application.
Each request for information will be dealt with on a case-by-case basis and, while there may not be information that can be disclosed in accordance with the Scheme, disclosure of other relevant information may still be possible
You can:
When you ask for a check, you’ll need to:
It can take up to 28 days for the police to finish a check. If the child is in immediate danger, then the police will act right away before the check is finished.
In the first 24 hours after you ask for a check, the police will work with you to find a safe way to keep in touch.
Within 10 days of asking for a check, you’ll need to attend a meeting or have a call with the police to:
If the police cannot confirm your identity, you cannot be told the results of the check. The police will still act to keep the child safe.
If the police have found any relevant information, they’ll decide who needs to be told. This might not be you.
It will usually be the people best placed to protect the child, such as the child’s parent, guardian or carer.
The police will normally tell the person who was checked that they’re sharing this information, if they decide it’s safe to do that. This might include telling the person that you asked for the check. The police will talk to you when making this decision.
The police will only share information with you if you sign an agreement promising not to tell anyone else.
If you think there are other people who should be told, ask the police about this.
In addition to the ‘right to ask’ (where an applicant contacts the police to ask for information), there is also a ‘right to know’. The “Right to Know” is where the police receive indirect information that may impact the safety of children and have not received a request for information through the ‘Right to Ask’ process. This could include (but is not limited to):
The purpose of the ‘Right to Know’ is to allow the police to act proactively when they are in receipt of information about a risk to a child or children, when it is already known that disclosure is necessary and proportionate.
The ‘Right to Know’ is also known as Sarah’s law or Child Sexual Offender Disclosure Scheme (CSODS).
RELATED GUIDANCE
Born into Care: Best Practice Guidelines and Other Resources (Nuffield Family Justice Observatory)
CONTENTS
There is no single accepted definition of a concealed pregnancy, but it covers situations where a woman, through fear, ignorance or denial, does not accept, or is unaware of, her pregnancy. It can include no, or late, engagement with maternity services, such as presenting at hospital in labour or delivering the child with no medical intervention.
It can cover a variety of situations such as:
Women may conceal or deny their pregnancy for a variety of reasons including:
Whilst there is a criminal offence of concealment of birth (the secret disposal of the dead body of an infant to conceal knowledge of the child’s birth), there is no criminal offence of concealment of pregnancy. A woman with mental capacity is free to choose not to engage with maternity services. However, where the woman does not have mental capacity or there is uncertainty as to mental capacity, legal advice should be sought. Lack of mental capacity may be due to factors such as learning disability, mental health or age (see also Mental Capacity and Consent chapter). If the mother is a child herself, a referral should be made to children’s social care. Action may be required to safeguard the mother and / or the child once born. If she is less than 16 years of age, a criminal offence may have been committed and police should be informed for further investigation.
Lack of antenatal care presents a risk to the unborn child due to lack of assessment of the maternal history, gestational age and health of the pregnancy, and research has shown that women who do not engage, or engage very late, with maternity services are at higher risk of maternal and foetal complications.
Risks for the baby include:
Where there is considered to be a risk of significant harm to the child, a referral to children’s social care should be made (see Referrals chapter). Consideration should be given to the reason for the concealment and a risk assessment of the reason undertaken by means of a multi-agency assessment (see also Assessments chapter).
Previous concealed pregnancies are a risk factor for future concealed pregnancies, and multi-agency information sharing is an important consideration.
Action to safeguard a child may be necessary before the child is born where there are concerns around the ability of the parents to effectively care for and safeguard the child once born. This may include:
Born into Care: Best Practice Guidelines for When the State Intervenes at Birth (Nuffield Family Justice Observatory) sets out guidelines to inform multi-agency practice when action is taken to safeguard children at birth:
Any practitioner who has concerns about the welfare of the unborn child should discuss with their safeguarding lead and consider whether a referral needs to be made to local authority children’s social care. This should be done without delay if there is a concern that the child is likely to suffer significant harm (see Referrals chapter).
The focus of multi-agency work should be on assessing the ability of the parent/s to protect and care for the child once born, what support needs to be put in place to facilitate this, action needed to safeguard the child and plans for the birth.
An early help assessment may be undertaken to assess what help needs to be put in place. Where there are concerns that the child may be at risk of significant harm once born, a child protection conference should be held to enable agencies to share all relevant information and reach a decision as to whether the child will be made subject to a child protection plan at birth and a core group established to implement the child protection plan (see Child Protection Conferences and the Child Protection Plan chapter).
Timescales should allow for the possibility of premature birth, especially where there are risk factors such as substance misuse by the mother or previous premature birth/s.
Legal advice must be sought where concerns are such that the child needs to be removed from the parents at birth. Court orders cannot be granted in respect of the child until it is born, but arrangements must be made so that an application for an interim care order can be made as soon as the child is born and / or joint risk assessments to keep mum and baby safe.
A pre-birth planning meeting should be held with relevant agencies to set out the birth arrangements and plan for the baby after birth. This should contain sufficient detail of the management of any risks. The plan should cover necessary steps to safeguard the child immediately after birth, such as:
RELATED GUIDANCE
Dogs and Children: Living Safely Together (Dogs Trust)
CONTENTS
Under the Dangerous Dogs Act 1991 (as amended), it is a criminal offence to allow a dog to be dangerously out of control anywhere, such as:
A dog is considered dangerously out of control if it:
A court could also decide that a dog is dangerously out of control if either of the following apply:
This applies to all dogs.
It is also a criminal offence to own certain specific types of dog:
It is also an offence to:
It is important to recognise that any dog can present a potential risk of harm to babies and children, and where dogs are present in the home, the risks should be assessed.
Any dog can bite if it is worried or scared and feels it has no other choice. 70% of all dog bites in the UK are to children, making them the most at-risk age group. 91% of bites to children occur within the home by a known dog, often their own dog. From a dog’s point of view, children behave very differently to adults, being unpredictable and prone to making a lot of noise, meaning supervision by parents/carers within the home and outside is crucial to keeping children safe.
Keeping Children Safe Around Dogs (RSPCA) recommends six ‘golden rules’ for parents / carers to help keep children safe around dogs, including never leaving your child alone in the same room as a dog, even your own and always supervise your child when they are with your dog.
Guidance: Code of Practice for the Welfare of Dogs (Department for Environment, Food & Rural Affairs) sets out practical guidance on how to provide a suitable environment for a dog to live in, based on the requirement of Section 9 of the Animal Welfare Act 2006.
Dogs may pose a higher risk of harm to children where:
An assessment should consider:
Practitioners should ask to see the dog and where / how it is kept.
Assessment of the risks posed by dogs in the household should be an ongoing process not a one-off event as circumstances may change.
Where there is assessed or known to be a risk of significant harm to a child, or where harm has already occurred such as the dog attacking a child, a referral should be made to children’s social care and safeguarding processes engaged (see Referrals chapter). Relevant agencies should be informed, such as police where there is a known or suspected criminal offence.
RELEVANT CHAPTERS
Multi-Agency Risk Assessment Conference (MARAC)
RELEVANT INFORMATION
Domestic Abuse Statutory Guidance (Home Office)
Controlling or Coercive Behaviour Statutory Guidance Framework (Home Office)
Domestic Abuse: How to get Help (Home Office)
SafeLives – Resources for Professionals working with victims of domestic abuse and their families
Independent Domestic Violence Adviser Statutory Guidance (Ministry of Justice)
January 2026: A new Section 5.2 Independent Domestic Violence Advisers has been added.
Scope
This policy sets out how partners across Buckinghamshire will identify, assess, protect and support children and families affected by domestic abuse, and how we will disrupt and manage perpetrators through coordinated multi‑agency practice. It applies to all organisations working with children, young people, parents/carers and families in Buckinghamshire, including statutory, voluntary and community services.
Who it’s for:
In Buckinghamshire, the BSCP, the Safer Buckinghamshire Partnership and the Buckinghamshire Domestic Abuse Partnership (BDAP) coordinate local strategy, services and training.
CONTENTS
The Domestic Abuse Act 2021 provides a definition of domestic abuse.
It is the behaviour of one person towards another where:
Behaviour is defined as abusive if it consists of any of the following:
It does not make any difference whether the behaviour is a single incident or consists of a number of incidents over a period of time.
Economic abuse is any behaviour by a person that has a negative impact on the other person’s ability to:
Children are recognised as victims of domestic abuse if they see, hear, or experience the effects of the abuse, and are related to the victim and / or perpetrator of the domestic abuse, or if the victim and / or perpetrator have parental responsibility.
The definition of domestic abuse also includes ‘honour’ based abuse (see ‘Honour’ Based Abuse chapter), female genital mutilation (see Female Genital Mutilation chapter) and forced marriage (see Forced Marriage chapter).
Domestic abuse also includes child-to-parent abuse.
See also Controlling or Coercive Behaviour Statutory Guidance Framework (Home Office)
Controlling behaviour is a range of acts designed to make a person subordinate and/or dependent by isolating them from sources of support, exploiting their resources and capacities for personal gain, depriving them of the means needed for independence, resistance and escape and regulating their everyday behaviour.
Coercive behaviour is an act or a pattern of acts of assault, threats, humiliation and intimidation or other abuse that is used to harm, punish, or frighten their victim.
Both coercive and controlling behaviour can apply to people who are no longer in a relationship but were previously.
The Act introduced the term ‘personally connected’. This applies to people who:
Victims of domestic abuse do not solely come from one gender or ethnic group. Abuse occurs in same sex relationships, is committed by young people against other family members or partners (teenage domestic abuse is the most common), as well as abuse of older relatives or those with physical or learning disabilities. Domestic abuse occurs irrespective of social class, racial, ethnic, cultural, religious or sexual relationships or identity.
Domestic abuse has a significant impact on children and young people of all ages (up to 18 years old)
Section 76 Serious Crime Act 2015 created the offence of Controlling or Coercive Behaviour (CCB) in an intimate or family relationship.
Practitioners should be mindful of how CCB overlaps with other offences such as stalking, harassment and assaults.
Experience of domestic abuse is recognised as an Adverse Childhood Experience (ACE) and can contribute towards early trauma. The presence of domestic abuse has been identified as a risk factor for child physical and emotional abuse, with children who were exposed to domestic violence being more likely to be physically abused and neglected.
Young people can also experience abuse in their own relationships (‘peer on peer abuse’). Experiencing abuse in their own intimate relationships can be hugely damaging for young people and abuse in teenage relationships should be taken just as seriously as in adult relationships.
Broadly, some of the impacts that domestic abuse can have on children can include:
Non-physical forms of domestic abuse like coercive control have a significant impact on children and professionals focused on physical acts of violence may fail to understand the daily experience of victims and children, how it is affecting them, and the level of risk posed by perpetrators.
On average victims experience on average 50 incidents, and over a two and a half year period, before seeking support (see SafeLives).
Interventions with adults who are experiencing or at risk of domestic abuse should seek to:
Professionals from any agency may receive a disclosure from a victim or perpetrator about domestic abuse or have concerns that such behaviour is taking place. All staff working with children and families should be familiar with the signs of domestic abuse and know how to respond.
Concerns may also be reported by a member of the extended family, friend or neighbour for example. Such information must be responded to in accordance with these procedures.
Professionals in contact with adults who are threatening or abusive to them as professionals, should be aware of the potential for that individual to be also abusive in their personal relationships. They should, therefore, assess whether domestic abuse may be occurring within the family environment.
See also SafeLives: Resources for identifying the risk victims face including the Domestic Abuse, Stalking and Harassment (DASH) checklist.
When carrying out a risk assessment, professionals should see the adult on their own.
When assessing domestic abuse and the needs of the adult living with domestic abuse, the following factors should be considered:
The professional should decide, based on any assessment and their professional judgement as to whether there is a threat to the safety of the adult or anyone else in the home environment. If the threat is imminent, the police should be contacted immediately by telephoning 999.
The police are often the first point of contact for adults experiencing domestic abuse. However, the Ambulance Service and hospital Emergency Departments may also be involved as a first point of contact.
Professionals should ensure that they make a full record of all discussions, including referrals to other agencies.
Under the Domestic Abuse Act, local authorities have a duty to provide support in refuges / other safe accommodation to victims of domestic abuse and their children. In addition, all eligible homeless victims of domestic abuse automatically have ‘priority need’ for homelessness assistance.
The first priority must always be the safety and welfare of the child.
Where there is an imminent risk of serious harm, the police must be contacted and steps taken to ensure immediate protection for the child. See Immediate Protection chapter.
Children and young people may be victims of domestic abuse both directly (in their own relationships) and by witnessing the abuse of others such as a parent. Domestic abuse also includes child-to-parent abuse.
Agencies should recognise the impact domestic abuse has on children and support them accordingly. Those responding to children experiencing domestic abuse should follow existing safeguarding, risk assessment and referrals processes and procedures.
A referral should be made to children’s social care and the safeguarding children process initiated and followed. See Referrals chapter.
It is vital that young people who experience domestic abuse within their own relationships are referred through a multi-agency risk assessment, using an appropriate risk assessment tool such as the Domestic Abuse, Stalking and Harassment (DASH) checklist. See SafeLives: Resources for Identifying the Risk Victims Face.
Professionals should be equipped to identify and respond to children and young people experiencing domestic abuse, drawing on the range of support available, from early intervention to crisis stage. Best practice responses involve an integrated response which combines child safeguarding and high-risk domestic abuse expertise, particularly in relation to risk assessment and safety planning. Further details on responding to young people experiencing abuse can be found in: Children and Young People (SafeLives), Work with Young People’s Violence and Abuse (Respect) and Good Practice Guidance for Specialist Services for Children and Young People (Women’s Aid).
Once their safety has been secured, children and young people should be offered support based on their individual needs, with a range of interventions, so that each child is able to access the specialised help they require. This could include access to psychoeducational support, therapeutic services (for example, counselling) or specialist children’s victim support workers or an independent domestic violence adviser (IDVA) who is able to work with children and young people. A strengths-based approach to recovery, building on ‘the resilient blocks in the child’s life’, has been shown to be effective in interventions for children.
Professionals should recognise the dynamics, impact, and risk when responding to cases of child-to-parent abuse. Where indicated, this may include, commissioning specialised local child-to-parent abuse services. It is important that a young person using abusive behaviour against a parent or family member receives a safeguarding response.
Professionals should develop an individual response for every child and young person affected, including for siblings. Professionals must take the individual needs of the child into consideration to support them to communicate in a way they feel comfortable. This may include drawing on multi-agency approaches, working with educational psychologists and drawing on the knowledge of those who know the child best, such as their teacher or any therapists currently involved in their support. It is important that children and young people have the communication tools appropriate to report abuse and engage with professionals trained to aid their communication where needed.
The Young People’s Family Justice Board have produced some Top Tips for Professionals Working with Children and Young People who Have Experience of and Been Affected by Domestic Abuse.
All agencies have a duty to assess whether a safeguarding response is required before referring an incident to a multi-agency partnership.
The response to domestic abuse is a complex one that spans several statutory and non-statutory agencies, including but not limited to, local authorities, community-based agencies, children’s services, schools, housing, health (including mental health), drug and alcohol services, specialist domestic abuse agencies, the police and the criminal justice system. Wider organisations, such as employers and financial services institutions also have a role to play.
Agencies have a responsibility to work together effectively to provide support and protection to victims of domestic abuse. This can be through strategic planning, co-commissioning and creating joined-up services. Working together is essential to help with identifying domestic abuse at an early stage and with responding to domestic abuse in a manner that can reduce the risk of escalation. It is vital to appropriately safeguard victims, including children, regardless of the level of risk.
An effective multi-agency response means that all frontline agencies consider domestic abuse and are trained to understand both the complex dynamics and the signs of domestic abuse.
Multi-agency working should be embedded into approaches to responding to domestic abuse and should offer a range of interventions and support, from early intervention to support for high-risk cases through formalised safeguarding arrangements. These responses can include but are not limited to:
A Multi-Agency Risk Assessment Conference (MARAC) is a non-statutory process that brings together statutory and voluntary agencies to jointly support adult and child victims of domestic abuse who are at a high risk of serious harm or homicide, and to disrupt and divert the behaviour of the perpetrator(s).
See Multi-Agency Risk Assessment Conference chapter
Independent Domestic Violence Advisers (IDVAs) provide independent support to victims / survivors of domestic abuse.
They provide support regardless of whether a victim / survivor has chosen to report an offence to the police, whether they have ended the relationship with the perpetrator or whether they are victims of multiple offences.
IDVAs can help victims / survivors to understand and systems and processes relating to areas such as victims’ / survivors’ rights, health and wellbeing, reporting to the police, criminal and family justice processes and accessing support services.
Children and Young Persons IDVAs (CHIDVAs) support children and young people experiencing domestic abuse between adults in their household or within their own intimate relationships.
Young Persons Violence Advisers (YPVAs) work with young people experiencing domestic abuse in their own intimate relationships.
Court IDVAs provide dedicated support for victims / survivors navigating courts by offering practical and emotional support throughout both public and private law proceedings. Their role includes explaining the court process and the different options that are available, supporting with any arrangements required (such as travelling to court or childcare), attending court with victims/survivors and liaising with court officials.
Health-based IDVAs (HIDVA) provide support to victims / survivors of domestic abuse who are accessing healthcare, alongside providing training and case consultation assistance for health professionals to understand and respond to domestic abuse.
A victim / survivor can be referred into the IDVA service at any time, by any professional engaging with them. Some IDVA services accept self-referrals by victims themselves.
See also Independent Domestic Violence Adviser Statutory Guidance
Agencies must work together and share information to ensure they are able to draw on all the available information held within each agency to build a full picture of the victims, including children, and perpetrators. This includes looking holistically at an individual’s case and circumstances to identify appropriate multi-agency support.
All relevant information should be recorded. Information sharing is only as good as the quality of the information being shared, and the level of detail can be crucial to accurate risk assessment. For example, simply recording “there is a history of domestic abuse” does not give other professionals the level of detail needed to be able to risk assess.
There must be a lawful basis to process (including sharing) any personal data. What lawful basis is appropriate will depend on the specific purpose for the processing. For further information see Information Sharing and Data Protection chapters.
See also Domestic Violence Protection Notices (DVPNs) and Domestic Violence Protection Orders (DVPOs) Guidance (gov.uk). These orders will become Domestic Abuse Protection Orders and Domestic Abuse Protection Notices under the Domestic Abuse Act 2021).
DVPOs are a civil order that fills a ‘gap’ in providing protection to victims by enabling the police and magistrates’ courts to put in place protective measures in the immediate aftermath of a domestic violence incident where there is insufficient evidence to charge a perpetrator and provide protection to a victim via bail conditions. It is important to note that bail with conditions and protective measures can be used simultaneously to build up greater protection for the victim.
A DVPN is an emergency non-molestation and eviction notice which can be issued by the police, when attending to a domestic abuse incident, to a perpetrator. Because the DVPN is a police-issued notice, it is effective from the time of issue, thereby giving the victim the immediate support they require in such a situation. Within 48 hours of the DVPN being served on the perpetrator, an application by police to a magistrates’ court for a DVPO must be heard.
A DVPO can prevent the perpetrator from returning to a residence and from having contact with the victim for up to 28 days. This allows the victim a degree of breathing space to consider their options with the help of a support agency. Both the DVPN and DVPO contain a condition prohibiting the perpetrator from molesting the victim.
A Domestic Violence Protection Notice and subsequent Order are aimed at perpetrators who present an on-going risk of violence to the victim with the objective of securing a co-ordinated approach across agencies for the protection of victims and the management of perpetrators.
The DVPN / DVPO process builds on existing procedures and bridges the current protective gap, providing immediate emergency protection for the victim and allowing them protected space to explore the options available to them and make informed decisions regarding their safety.
The DVPN / DVPO process does not aim to replace the criminal justice system in respect of charge and bail of a perpetrator. A DVPN will be issued in circumstances where no other enforceable restrictions can be placed upon the perpetrator.
Although the power to issue a DVPN and subsequent application for a DVPO lies with the police and ultimately the criminal justice service, the success of any such process will be reliant on the partnership work with other agencies and organisations including those that contribute to Multi-Agency Risk Assessment Conferences (MARACs) and service providers for independent domestic violence advisers (IDVAs) or other, similar services.
Engagement with the victim and the agencies referred to above at the earliest opportunity, is crucial to the success of the DVPN / DVPO process.
See Multi-Agency Risk Assessment Conference chapter
The Domestic Violence Disclosure Scheme (also known as Clare’s Law) is made up of two elements: the Right to Ask and the Right to Know.
Under the right to ask, a person or relevant third party (for example, a family member) can ask the police to check whether a current or ex-partner has a violent or abusive past. If records show that an individual may be at risk of domestic abuse from a partner or ex-partner, the police will consider disclosing the information.
Right to Know enables the police to make a disclosure on their own initiative if they receive information about the violent or abusive behaviour of a person that may impact on the safety of that person’s current or ex-partner. This could be information arising from a criminal investigation, through statutory or third sector agency involvement, or from another source of police intelligence.
Addressing perpetrator behaviour is as important as safeguarding and supporting victims. Tackling perpetrator behaviour and placing the onus on them should be a key consideration for partnership work.
Agencies should take the earliest opportunity available to consider how the behaviour of the perpetrator can be disrupted or constrained, putting the emphasis for change on that individual. The response to the perpetrator must be appropriate for the unique context and needs of the victim. For instance, victims subject to ‘honour’-based abuse may be experiencing a spectrum of behaviours from multiple perpetrators.
Where the threshold for HM Prison and Probation Service (HMPPS) statutory interventions is not available, agencies should consider creative options to address the behaviour of the perpetrator, including recourse to Youth Offending Teams, Integrated Offender Management (IOM), Multi-Agency Targeting And Co-ordinating (MATAC), Domestic Abuse Perpetrator Programmes, safeguarding, housing, Department for Work and Pensions (DWP) and the full range of quality assured perpetrator programmes. Any approaches adopted should work closely with existing arrangements, including MARAC to ensure perpetrator management teams have key information from victim-focused panels.
See also Multi-Agency Public Protection Arrangements chapter
It is important that local areas commission safe, effective perpetrator programmes which take into account the needs in their areas and are accompanied by support for any associated victims. These should be ‘as well as’ support for victims, not ‘instead of’.
Behaviour change interventions aim to challenge and support perpetrators of abuse to make long term changes to their violent and abusive behaviour. They also consider additional needs such as alcohol and substance misuse and mental health difficulties.
It is important to assess any potential risks to professionals, carers or other staff who are providing services to a family where domestic abuse is or has occurred. In such cases a risk assessment should be undertaken. Professionals should speak with their manager and follow their own agency’s guidance for staff safety. Such issues should also be discussed during supervision.
CONTENTS
Lord Justice Ryder wrote, in a court judgement from 2005:
“The terms ‘Munchausen Syndrome by Proxy’ and ‘Factitious (and Induced) Illness (by Proxy)’ are child protection labels that are merely descriptions of a range of behaviours, not a paediatric, psychiatric or psychological disease that is identifiable. In reality, the use of the label is intended to connote that in the individual case there are materials susceptible of analysis by paediatricians and of findings of fact by a Court concerning fabrication, exaggeration, minimisation or omission in the reporting of symptoms and evidence of harm by act, omission or suggestion (induction).
For my part, I would consign the label MSBP to the history books and however useful FII may apparently be to the child protection practitioner I would caution against its use other than as a factual description of a series of incidents or behaviours that should be accurately set out (and even then, only in the hands of the paediatrician or psychiatrist/psychologist).
What I seek to caution against is the use of the label as a substitute for factual analysis and risk assessment. “
For further information, please see A County Council v A Mother & Ors [2005] EWHC 31 (Fam)
This guidance strongly promotes the recommendations of Lord Justice Ryder.
Fabricated or Induced Illness (FII) is a term used increasingly by professionals from all agencies involved in safeguarding and protecting children. However, there remains debate and disagreement about the nature and definitions of FII. For the purposes of this guidance, FII is considered as, ‘a clinical situation where a child has suffered or is likely to suffer significant harm through the fabrication, falsification, or induction of illness by a carer and/or from responses to these parental actions by health professionals.
By using the term FII, health professionals are expressing their concerns that the child has suffered or is likely to suffer significant harm. In describing the harm, all professionals, health, and non-health, are encouraged to use the language of Working Together to Safeguard Children, which is multi-agency statutory guidance published by the Department for Education.
Medically Unexplained Symptoms (MUS): In Medically Unexplained Symptoms (MUS), a child’s symptoms, of which the child complains, and which are presumed to be genuinely experienced, are not fully explained by any known pathology. The symptoms are likely based on underlying factors in the child (usually of a psychosocial nature), and this is acknowledged by both clinicians and parents. MUS can also be described as ‘functional disorders’ and are abnormal bodily sensations which cause pain and disability by affecting the normal functioning of the body. The health professionals and parents/carers work collaboratively to achieve evidence-based therapeutic work in the best interests of the child or young person.
Perplexing Presentations (PP): The term Perplexing Presentations (PP) has been introduced to describe the commonly encountered situation when there are alerting signs of possible FII (not yet amounting to likely or actual significant harm), when the actual state of the child’s physical, mental health and neurodevelopment is not yet clear, but there is no perceived risk of immediate serious harm to the child’s physical health or life. The essence of alerting signs is the presence of discrepancies between reports, presentations of the child and independent observations of the child, implausible descriptions and unexplained findings or parental/carer’s behaviour.
Fabricated or Induced Illness (FII): FII is a clinical situation in which a child is, or is very likely to be, harmed due to parent(s)/carer(s) behaviour and action, carried out in order to convince doctors that the child’s state of physical and/or mental health and neurodevelopment is impaired (or more impaired than is actually the case). FII results in physical and emotional abuse and neglect, as a result of parental/carer’s actions, behaviours or beliefs and from doctors’ responses to these. The parent or carer does not necessarily intend to deceive, and their motivations may not be initially evident. It is important to distinguish the relationship between FII and physical abuse / non-accidental injury (NAI). In practice, illness induction is a form of physical abuse. In order for this physical abuse to be considered under FII, evidence will be required that the parent’s/carer’s motivation for harming the child is to convince doctors about the purported illness in the child and whether or not there are recurrent presentations to health and other professionals. This particularly applies in cases of suffocation or poisoning.
Alerting Features – these are clinical features associated with child maltreatment that may be observed when a child presents to healthcare professionals.
Consider – to consider child maltreatment means that maltreatment is one possible explanation for the alerting feature.
Suspect – to suspect child maltreatment means a serious level of concern about the possibility of child maltreatment but not proof of it.
In recognising the harm caused by FII, the effect and impact on the child should be the major concern of professionals caring for the child. Professionals are encouraged to consider the lived experience of the child and to listen to the voice of the child.
Rather than concentrating on diagnoses, professionals should consider the following:
Induction of illness: Induction of illness is rare. The commonest forms of induced illness are poisoning (usually by prescription medications) and suffocation. When the illness induction stops, the child may return to normal health but can still remain at risk of further harm. Further harm is likely to occur from medical interventions to investigate the cause of the child’s illness (iatrogenic harm) and the emotional impact on the child.
Falsification of illness: Falsification of illness is also rare. Clinical samples reported to be from the child can be tampered with or may not come from the child. For example, (e.g., non-human blood on clothing reported to have come from the child; urine samples can have sugar or blood added to them; thermometers can be warmed up with hot water).
Results of medical tests can be falsified or letters reportedly from health practitioners can be forged. Photographs reportedly of the child may be from another child or faked to look like a medical condition.
Fabrication of illness: Fabrication of illness is commonly encountered by health professionals. The situation can often be resolved through open discussion and careful management, however, where this is not possible, the child can sometimes experience significant harm.
Parents or carers may or may not realise that they are giving an incorrect account of the child’s health. Their description will depend upon multiple factors including parental health and health beliefs, culture, previous experience of healthcare and experience of childcare. Naïve exaggeration and deceitful lying could both be described as fabrication but are very different in how they should be managed.
Alerting signs are not evidence of FII. However, they are indicators of possible FII (not amounting to likely or actual significant harm) and, if associated with possible harm to the child, they amount to general safeguarding concerns.
Some alerting signs are initially recognised by community or primary health care professionals such as health visitors, GPs or community paediatricians, Social Care staff or by professionals in pre-school/early years, schools and other educational settings. Others are first noted by hospital-based paediatricians or in Child and Adolescent Mental Health Services (CAMHS).
The essence of alerting signs is the presence of discrepancies between reports, presentations of the child and independent observations of the child, implausible descriptions and unexplained findings or parental behaviours. Alerting signs may be recognised within the child or in the parent’s behaviour. A single alerting sign by itself is unlikely to indicate possible fabrication. It is important to look at the overall picture which includes the number and severity of alerting signs.
Clinical evidence suggests that fabricated or induced illness is usually carried out by the child’s mother or a female carer. However, practitioners should also be aware of the possibility of other perpetrators including fathers, grandparents, siblings or other children, or practitioners.
Parents/carers may have the following history or exhibit a range of alerting behaviours when they wish to convince others that their child is ill:
These patterns of behaviours are coercive, isolating and controlling and are patterns we see in a grooming process. Parents/carers could be grooming professionals through behaviours which could seek to initially get professionals to feel sorry for them, ingratiate themselves and then this can move on to intimidation.
Significant harm is defined in the multi-agency Continuum of Need Incorporating Threshold Guidance as a situation where a child is suffering, or is likely to suffer, a degree of physical, sexual and/or emotional harm (through abuse or neglect) which is so harmful there needs to be statutory intervention by child protection agencies in the life of the child and their family.
The harm caused by medical investigations and treatments always has to be balanced against their benefits. Carrying out tests, giving medicines or performing surgery on a child whose symptoms are misreported is more harmful than if symptoms are genuine. Harm can be caused directly by the parent, intentionally or unintentionally, and this harm may be reinforced by health professionals who cause iatrogenic harm inadvertently.
It is important to judge the severity of harm to the child rather than severity of a parent’s/carer’s actions. Severity of harm to the child should be assessed both by the intensity of each aspect of harm and by the cumulative effect of all the aspects. Whilst the motivation of the parent/carer is irrelevant to the determination of whether the child has suffered or is likely to suffer harm, motivation needs to be considered when planning how to manage the problem.
In the context of FII harm may be caused by physical abuse, emotional abuse or neglect. Although some of these children die, there are many that do not die as a result of having their illness fabricated or induced, but who suffer significant long term physical or psychological health consequences.
Physical abuse may include unnecessary pain and discomfort from unnecessary surgery, anaesthetic, medical investigations, procedures and treatments or through the precipitation of an illness by withholding medication.
Emotional abuse may include making the child unnecessarily anxious about their health and/or experience of healthcare, inducing psychiatric disorders and psychosocial difficulties causing social isolation so that the child’s sense of self is damaged.
Neglect may include disrupted education with unnecessary school absence and/or parental restrictions on participation in usual activities and genuine illness being overlooked.
The child’s views are important to ensure we understand how they view their symptoms and any concerns or worries that they may have. Children must be given opportunities to have their views explored, away from parents, in settings where they feel safe. Children can find it difficult to express views independently of their parents. In instances where a child is non-verbal or has communication difficulties either by language or ability, then the support of interpreting and/or specialist communication may need to be sought.
Previous FII guidance suggested that parents/carers should not be informed of safeguarding concerns until multiagency assessment had taken place. However, it is now agreed that parents/carers should be kept informed unless this would place the child at real risk of further harm.
In order to address alerting features before further harm is caused to a child, it is important that professionals are able have honest discussions with parents/carers and children at the earliest opportunity, so that a plan can be agreed to ensure the child’s wellbeing. However, a decision of who, how and when this should happen needs to be agreed by the professionals involved with the child and family at an early multi-agency discussion/professionals meeting.
If it is considered that a child is being harmed through FII, as with any other safeguarding concern, professionals should inform parents/carers (and children if appropriate) about referral to Children’s Social Care unless this would place the child at risk of further harm. An example where parents/carers might not be informed of contact with Children’s Social Care is in induced illness where poisoning is suspected. In this situation immediate protection may be needed to keep the child safe.
If you are uncertain whether to inform parents/carers take advice from your safeguarding lead or the named or designated doctor for safeguarding children. It is advised that you avoid terms such as fabrication or fictitious illness but explain to the parent/carer that they appear to be misunderstanding or processing the medical information in a way that may cause harm to their child for example missing school or not being able to participate in certain activities and therefore a referral to Children’s Social Care is being made to support them and the professionals involved with the child in understanding the medical needs of the child and to ensure that the risk to the child is reduced by supporting them with a Health and Education Rehabilitation plan.
If professionals decide not to share safeguarding concerns with parents/carers, there should be a well-considered risk assessment with clear documentation and early multi-agency discussion. Advice on whether to share safeguarding concerns in the context of FII can be obtained from Designated and/or Named Health Professionals. Professionals should note that seeking relevant permissions and informing parents and carers is to be reviewed on a regular basis by Managers, lead paediatrician and Named Doctor/Nurse, alongside partner agencies.
Careful, factual records should be kept, detailing who reported any concerns, what was observed, and by whom. Records of discussions, including about safeguarding concerns, should be kept within the child’s records (including their main health record), to ensure that this information is readily available to those involved in the child’s care, aiming to prevent further harm.
Records should include a clear explanation of the specific concerns and, where appropriate, a risk analysis based on the concerns and the professional’s opinion of these. Similarly, documentation of the harm to a child should use the recognised forms of harm. Records must include a clear account of what has or has not been discussed with the child and parents/carers.
It is recommended that professionals use caution or avoid the term ‘Fabricated or Induced Illness’ when writing records , it may be helpful to use terms such as ‘we are concerned that the parent/care giver is processing information about the child’s health in a manner that may cause harm to the child’.
See also Flowchart 1: Action if there are Alerting Signs of FII (opens as a PDF)
All professionals who have concerns about a child’s health should discuss these with their line manager, their agency’s designated safeguarding children adviser and the GP or paediatrician responsible for the child’s health. If the child is receiving services from local authority Children’s Social Care, the concerns should also be discussed with them.
It is recommended that school explain to the parents/carers that information is required from health to understand the concerns e.g. poor school attendance. It is then appropriate for education to contact health (either GP, consultant paediatrician or child psychiatrist) with their query about the actual health of the child. If parents/carers do not agree to health assessment or sharing of information, advice can be sought from organisational safeguarding leads and/or from Named or Designated Health Professionals.
If primary healthcare (GP) is the only contact for the child, then they may wish to refer to an appropriate secondary care consultant for further assessment of the child’s health. The referral must be explicit about the alerting features. If the response from health is felt to be inadequate, education can contact either the Named GP or Named Doctor for Safeguarding Children for advice.
In perplexing cases opportunities for multi-agency sharing of information, collaboration, planning and challenge should take place on a regular basis via review multi-agency meetings.
A “Responsible Consultant “, i.e., a consultant paediatrician (or, in cases of fabricated mental illness, a senior CAMHs practitioner), will lead on case management with a focus on the child’s voice and their current state of health, functioning, and involvement with health services. If initial concerns are raised in primary care or education, then a referral to an appropriate consultant should be made as in Section 8.1,Action if the initial concerns arise directly from education and not health.
Where there are concerns about more than one child in a family, each child may have a different or the same Responsible Consultant depending on the needs of the children involved. If there is disagreement about who should be the Responsible Consultant for a child, this should be discussed with the Named and/or Designated Doctor.
The Responsible Consultant should lead in liaising with all the other professionals involved to reach consensus about the child’s health and management, and then will discuss with the child and family:
A Health and Education Rehabilitation Plan should be agreed and implemented. The “Responsible Consultant” will lead on the plan, but this must be shared with all agencies involved. The plan must specify timescales and intended outcomes and be monitored and reviewed regularly. The Plan may include:
When FII is considered and/or suspected, parental or carer non-engagement, disguised and/or partial compliance are common, and need to be managed by the Responsible Consultant, together with the multi-agency team. If the parents/carers do not engage and/or oppose professionals plan for the child, the professional will have to consider whether the parents’ /carers’ actions or non-actions might lead to the child suffering significant harm and so whether referral to children’s services is indicated.
If parents/carers do not engage with the plan and the child is not considered to be at risk of significant harm the case should be reviewed to see whether monitoring and containment are appropriate. Advice may be sought from named or designated health professionals.
If the child has a social worker allocated by Children’s Services, Children’s Services will take the lead for safeguarding, working closely with the multi-agency team, particularly health and education, who will take the lead for their aspects of the case.
See also Flowchart 2: Action is Significant Harm is Suspected (opens as a PDF)
The process for the management of cases where there are concerns that a child has suffered or is likely to suffer significant harm from FII is the same as for any other case of child maltreatment. See also Section 47 Enquiries.
If at any stage, the Responsible Consultant or other professionals have concerns that the child has suffered or is likely to suffer significant harm, then the MASH should be contacted, and an urgent strategy discussion must take place with the Responsible Consultant (can include a Named or Designated Health professional) and action taken to make the child safe in accordance with each agency’s role and responsibility. Social Care, in this scenario, must. invite their Legal Representative to the Strategy Meeting. Other agencies should consider taking their own legal advice if there are concerns regarding non engagement or disguised compliance.
If there is evidence of illness induction or frank deception, such as interfering with specimens or medicine charts, urgent contact should be made with MASH, or, if needed, out of hours, with police and/or children’s services. If there are concerns of illness induction whilst a child is on the ward, for example a parent/carer interfering with medication, equipment or charts, then action should be sought to remove the parent/carer from the ward as they pose a risk to children at that point.
Chronologies are a useful tool in Perplexing Presentations or cases of FII. They should:
Chronologies should be compiled by individuals who have the expertise and ability to recognise and comment on any significant episodes. The Responsible Consultant (with support from the Named and/or Designated Doctor) is usually best placed to overview and analyse the combined multi-agency chronology and provide a report on this.
See Appendix 1 for the agreed multiagency chronology format. It is important that the headings and format are agreed across organisations and agencies so that they can be collated easily.
In most circumstances, there is agreement between professionals as to whether or not a child is at risk of significant harm and the process that should be followed. However, professional challenges should be seen as part of healthy professional working relationships.
If there are concerns about the health response from professionals (including concerns from education settings), advice can be sought from the Named GP, the Named Doctor for Safeguarding in a community or hospital trust, or from Designated Health Professionals.
If any professional considers that their concerns are not taken seriously or responded to appropriately, they should escalate their concerns following the Escalation, Challenge and Conflict Resolution Procedure.
Working Together to Safeguard Children (Department for Education) – The statutory guidance does not mention FII and FII is not a specified form of child abuse. However, within the definition of physical abuse it states that
‘Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child’.
Child Maltreatment: when to suspect maltreatment in under 18s (National Institute for Health and Care Excellence)- Contains limited guidance on when to consider FII (see paragraphs 1.2.11 – 1.2.12)
Perplexing presentations / fabricated or induced illness in children (Royal College of Paediatrics and Child Health)– This guidance is written primarily for paediatricians but can be helpful for other health professionals.
Assessment and management of adults and children in cases of fabricated or induced illness(FII) ( Royal College of Psychiatrists) – provides guidance for mental health professionals (MHPs), including psychiatrists, who may be asked to assess and manage adults and children where there is evidence of or concerns about abnormal illness-related behaviour by care givers.
Appendix 1 – Chronology of Significant Events: Template (opens in Word)
Appendix 2 – Flowchart 1: Action if there are Alerting Signs of FII (opens as a PDF)
Appendix 3 – Flowchart 2: Action if Significant Harm is Suspected (opens as a PDF)
RELEVANT INFORMATION
FGM Resource Pack (Home Office) – case studies, support materials and information on specialist organisations
Free E-Learning ‘Recognising and Preventing FGM’ (Home Office)
CONTENTS
Female Genital Mutilation (FGM) is a procedure where the female genital organs are deliberately cut, injured or changed and there is no medical reason for this. It is often a very traumatic and violent act and can cause harm in many ways. FGM can cause immediate as well as long-term health consequences, including pain and infection, mental health problems, difficulties in childbirth and/or death (see Section 2, Consequences of Female Genital Mutilation).
The age at which FGM is carried out varies according to the community. The procedure may be carried out on new-born infants, during childhood or adolescence or just before marriage or during a woman’s first pregnancy. There is no religious reason, in the Bible or Koran for example, for FGM and religious leaders from all faiths have spoken out against the practice. The exact number of girls and women alive today who have undergone FGM is unknown; however, UNICEF estimates that over 200 million girls and women worldwide have had FGM procedures.
FGM has been classified by the World Health Organisation (WHO) into four types:
Under the Female Genital Mutilation Act 2003, FGM is a criminal offence and a form of violence against women and girls.
There are no health benefits to FGM. Removing and damaging healthy female genital tissue interferes with the natural functions of women’s bodies.
Personal accounts from survivors show that FGM is an extremely traumatic experience for girls and women, the effects of which remain with them throughout their life. Young women may feel betrayed by their parents, when they are involved in the decision to have the procedure, as well as feeling regret and anger.
In England (as well as Wales and Northern Ireland), under the Female Genital Mutilation Act 2003 (‘the 2003 Act’) it:
Regardless of individual status in the UK ie. Permanent or otherwise, the same safeguarding response will be afforded to all.
A FGMPO is a civil order which can be made to protect a girl against FGM offences or protect a girl against whom a FGM offence has taken place. Breaching an order carries a penalty of up to five years in prison.
The terms of the order can be flexible, and the court can include whatever terms it thinks are necessary and appropriate to protect the girl, including to protect her from being taken abroad or to order giving up her passport so she cannot leave the country. See also: Making an Application for an FGM Protection Order (FGMPO) – Flowchart.
The most significant factor to consider when assessing if a girl may be at risk of FGM is whether her family has a history of practising FGM. In addition, it is important to consider whether FGM is known to be practised in her community or country of origin.
As FGM is illegal and therefore not discussed openly, women who have undergone FGM may not fully understand what FGM is, what the consequences are, or that they themselves have had FGM. Discussions about FGM should therefore always be undertaken with care and sensitivity.
There are a number of other factors which could indicate a girl is at risk of being subjected to FGM.
Signs that FGM may have taken place include:
If you have concerns, do not be afraid to ask a girl or woman about FGM, using appropriate and sensitive language. Women and girls sometimes say that professionals have avoided asking questions about FGM, and this can then lead to a breakdown in trust. If a professional does not give a girl / woman the opportunity to talk about FGM, it can be very difficult for her to bring this up herself.
There are screening tools that can be used to support the conversations, e.g. Guidance – FGM: Mandatory Reporting in Healthcare (Department of Health and Social Care)
FGM is illegal in England and Wales, and practitioners should act to safeguard girls who may be at risk of FGM or have been affected by it.
The girl may be at imminent risk, in which case immediate protection should be taken to protect her such as a Female Genital Mutilation Protection Order or other action such as an Emergency Protection Order or the exercise by the police of their powers of protection (see Immediate Protection chapter).
Practitioners should consult with their safeguarding lead and information should be shared with relevant agencies as appropriate to ensure a multi-agency response as necessary. A referral should be made to Children’s Social Care (see Referrals chapter).
Discussions with family members should be conducted sensitively and with use of accredited interpreters (not known to the family) as required. However, it is important to remember that the child may be at risk of harm from family members who may believe that FGM is in the girl’s best interests and may not understand the legal situation and implications. The primary consideration at all stages should be the safety and welfare of the girl.
Action should include:
Practitioners should inform their safeguarding lead and make a referral to Children’s Social Care so that further safeguarding enquiries can be made.
Regulated health and social care professionals and teachers in England and Wales have a mandatory duty to make a report to the police if they become aware of a girl having had FGM. See Section 8, FGM Mandatory Reporting Duty.
Action should include:
Whenever a girl is identified as having had, or being at risk of, FGM professionals must consider whether she is at risk of further harm, and whether there are other girls or women in her family or wider social network who may be at risk of FGM.
NHS England collects the following data from NHS acute trusts, mental health trusts and GP practices:
For more information please see Female Genital Mutilation (FGM, NHS)
Where a regulated health and social care professional or a teacher in England and Wales becomes aware of a case of FGM on a girl under the age of 18, they must report this to the police as soon as possible, preferably by the end of the next working day. They may become aware of the FGM because the girl has disclosed it to them or because they observe physical signs.
Please note: This is in addition to the safeguarding process. If a practitioner is concerned that a child has had FGM, they should also consult their safeguarding lead and make a referral to Children’s Social Care (see Referrals chapter).
See also:
Guidance – Mandatory Reporting of Female Genital Mutilation: Procedural Information (gov.uk)
Guidance – FGM: Mandatory Reporting in Healthcare (Department of Health and Social Care)
RELEVANT INFORMATION
Forced marriage and learning Disabilities: multi-agency practice guidelines (HM Government)
Forced Marriage Resource Pack (Home Office) – examples of best practice to ensure that effective support is available to victims of forced marriage
Forced Marriage: A Survivor’s Handbook (Foreign, Commonwealth & Development Office)
RESOURCES FOR RAISING AWARENESS
Forced Marriage – Free e-learning
The Foreign and Commonwealth office have produced a series of short YouTube videos covering the consequences of forced marriage, and how to spot the signs of a forced marriage.
FOR PEOPLE DIRECTLY AFFECTED – If you’re trying to stop a forced marriage or you need help leaving a marriage you’ve been forced into, contact the Forced Marriage Unit (FMU)
In an emergency call the Police on 999
CONTENTS
A forced marriage is one where one or both parties do not or cannot consent to the marriage. Pressure may be applied to agree to the marriage, but, under the Marriage and Civil Partnership (Minimum Age) Act 2022 it is a criminal offence to do any acts for the purpose of causing a child (before their 18th birthday) to marry, whether or not any forms of coercion take place.
The pressure put on children to marry against their will can be:
Forced marriage can happen to boys and girls (although most cases involve girls) and there is no ‘typical’ victim of forced marriage.
Forced marriage can take place anywhere in the world, including in the UK. In many cases forced marriage involves a potential partner being brought into the UK from overseas or a British person being taken abroad for the forced marriage, often without them knowing that they are going to be married. Forced marriage of any person, regardless of sex, age, disability, ethnic origin or sexual orientation, is illegal in the UK (see Section 5, Forced Marriage Offences).
Forced marriage is very different to an arranged marriage, which is where families of both parties take a lead in the arrangements for the marriage, but they are free to decide whether they want the marriage to go ahead or not.
People who force others into marriage often try to justify their behaviour as ‘protecting’ their children, building stronger families and preserving so-called cultural or religious beliefs. However, the act of forcing another person into marriage can never be justified on religious grounds: every major faith condemns the practice of forced marriage.
Some of the key motives given for forced marriage are:
Victims trapped in, or under the threat of, a forced marriage can be very isolated. They may feel there is nobody they can trust to keep this secret, and they have no one to speak to about their situation – some may not be able to speak English.
People who are forced to marry find it very difficult to leave the marriage, and girls may be subjected to repeated rape (sometimes until they become pregnant) and domestic abuse within the marriage. In some cases, victims suffer violence and abuse from extended family members and are forced to do all the household jobs and / or are kept under virtual ‘house arrest’ and not allowed to leave the home without a family escort.
Both male and female victims may feel that running away is their only option. For many leaving the family can be very hard. They may have little experience of life outside the family and worry about losing their support network. Also, leaving their family (or accusing them of a crime, or asking the police or the council for help) may be seen as bringing shame on their ‘honour’ and on the ‘honour of their family’. Those who do leave often live in fear of their own families, who may go to considerable lengths to find them and bring them back home.
Victims of forced marriage, their siblings and other family members are at risk of harm – particularly if they are found to asked for help or are planning to leave the marriage. Victims can face the possibility of ‘honour’-based abuse, rape, kidnap, being held against their will, threats to kill, being abducted overseas and even murder.
The Forced Marriage Unit (FMU) is available to talk to frontline professionals handling cases of forced marriage. It also offers information and advice on the wide range of tools available to tackle forced marriage, including how the law can be used in particular cases, what assistance is available to British victims in different countries and how to approach victims.
All practitioners working with suspected or actual victims of forced marriage should be aware of the “one chance” rule. This is that they may only have one opportunity to speak to a victim and may only have one chance to save their life.
If someone discloses that they are in or at risk of a forced marriage, it should never be dismissed as just a ‘family matter’. For many people, asking for help from an agency is a last resort and so all disclosures of forced marriage must be taken seriously.
Do NOT:
A multi-agency response is vital.
REMEMBER – Younger siblings might be at risk of being forced to marry when they reach a similar age. Appropriate action may be needed to safeguard younger siblings.
The Anti-social Behaviour, Crime and Policing Act 2014 made it a criminal offence in England (Wales and Scotland) to force someone to marry.
This includes:
Forcing someone to marry can result in a prison sentence of up to seven years.
The Marriage and Civil Partnership (Minimum Age) Act 2022 amended the Anti-social Behaviour, Crime and Policing Act 2014 so that that it is an offence to do any acts for the purpose of causing a child to enter into a marriage before their eighteenth birthday (whether or not the conduct amounts to violence, threats, any other form of coercion or deception). 16 to 17-year-olds are no longer able to marry / enter a civil partnership at all. (Previously, under the 2014 Act, forced marriage was only an offence if coercion was used to cause someone to marry, or if the person lacked mental capacity to consent to marry).
Anyone threatened with forced marriage or forced to marry against their will can apply for a Forced Marriage Protection Order (FMPO). Relatives, friends, voluntary workers, police officers and local authority staff can also apply for a FMPO, see Apply for a Forced Marriage Protection Order.
The order is to protect a person from being forced to marry. The details of each order will be specific to the case, for example the court may order someone to hand over the person’s passport or reveal where they are if they cannot be found.
Breaching a FMPO can result in a prison sentence of up to five years.
To protect victims of forced marriage, practitioners may need to share information with other agencies such as the police.
See Tier 1 – Children Safeguarding Data Sharing Agreement (DSA).
Keeping records of forced marriage is important. These may be used in court proceedings.
Staff should keep records of all actions taken, including the reasons why particular actions were taken. There should be a recorded agreement of which agency has agreed to each proposed action, together with the outcomes of the action.
Records should:
Even if forced marriage is not disclosed, a record of the concerns may be useful in the future.
All records should be kept secure, and only accessed by staff directly involved in the case. This is particularly important for victims / potential victims of forced marriage, to make sure no one could pass on confidential information to a victim’s family.
If no further action is to be taken this should be clearly documented, together with the reasons.
RELATED INFORMATION
Problematic and Harmful Sexual Behaviour (NSPCC)
Harmful Sexual Behaviour among Children and Young People: Guideline NG55 (NICE)
SUPPORT IN BUCKINGHAMSHIRE
CABS (Child and Adolescent Harmful Behaviour Service) for children and young people in Oxfordshire and Buckinghamshire about whom there are concerns in relation to harmful sexual behaviour (HSB).
January 2026 – This procedure which provides a framework for identifying and responding to concerns around harmful sexual behaviour is new.
CONTENTS
This procedure provides a clear, coordinated framework for professionals across Buckinghamshire to:
The term ‘harmful sexual behaviour’ describes a continuum of behaviours displayed by children and young people under 18, ranging from those considered ‘inappropriate’ at a particular age or developmental stage to ‘problematic’, ‘abusive’ and ‘violent’ behaviours (Hackett). The NSPCC uses the following definitions:
Problematic or harmful sexual behaviour can include:
Research by the Centre of Expertise on Child Sexual Abuse shows that in pre-adolescent children, behaviour is more likely to be at the ‘inappropriate’ or ‘problematic’ end of the continuum. Most pre-adolescent children displaying harmful sexual behaviour have themselves been sexually abused or experienced other kinds of trauma or neglect.
Older children and young people displaying harmful sexual behaviour are mostly boys, many of whom have a history of adverse childhood experiences and family difficulties.
Most sexually abused children and young people do not go on to abuse others, and the majority of children and young people displaying harmful sexual behaviour do not commit sexual offences as adults. However, older adolescents who abuse younger children, and those whose sexual behaviours involve violence, are at greater risk of further sexual offending.
The limited research into technology assisted harmful sexual behaviour suggests that boys who engage ‘only’ in watching images of child sexual abuse online have far less troubled histories than those who commit other sexual offences. There may sometimes be a link between viewing online pornography and subsequent harmful sexual behaviours.
There is limited published research on effective interventions, particularly at the ‘problematic’ end of the continuum, although there is a general consensus that interventions need to be holistic, child-focused and involve parents/carers.
Professionals working with children need knowledge and skills to respond to harmful sexual behaviour, and to create organisational contexts which maximise safety from abuse. Prevention education should take a long-term, ‘whole school’ approach to healthy relationships, and involve children and young people in development and delivery. Broader public health approaches which challenge gender inequality and patriarchal values and attitudes are also required.
The Harmful Sexual Behaviour (HSB) Framework and Audit: An Evidence-informed Operational Framework for Children and Young People Displaying Harmful Sexual Behaviours (Hackett, Branigan, and Holmes, NSPCC) covers the essential elements of developing and delivering an integrated and effective HSB service for children, young people and their families:
Hackett’s continuum presents sexualised behaviour as a range from ‘normal’ to ‘inappropriate’, ‘problematic’, ‘abusive’ and ‘violent’ (Hackett, Children, Young People and Sexual Violence, in Barter and Berridge Children Behaving Badly? Exploring Peer Violence Between Children and Young People, Wiley). See Continuum Guide (NSPCC)
See the Understanding Sexualised Behaviour in Children (NSPCC) for further information.

Diagram of the Hackett Continuum.
The NSPCC use the term ‘developmentally typical’ to describe behaviours that are green on the continuum – these green behaviours might also be termed ‘healthy’, ‘normal’ or ‘developmentally expected’.
Green sexual behaviour:
The NSPCC use ‘problematic sexual behaviour’ (PSB) as an umbrella term for all amber behaviours. On the Hackett continuum, amber behaviours are described as ‘inappropriate’ or ‘problematic’.
inappropriate behaviour includes:
Problematic behaviour includes:
Red sexualised behaviours are harmful to the child who displays them, as well as the people the behaviour is displayed towards. The NSPCC refer to all red sexual behaviours as ‘harmful sexual behaviour’ (HSB). Hackett divides these into ‘abusive’ and ‘violent’ behaviours.
Abusive behaviour includes:
Violent behaviour includes:
An understanding of how children develop sexually can help practitioners recognise which sexual behaviours are developmentally typical and identify if a child is displaying behaviour that is problematic or harmful.
Sexual Development and Behaviour in Children (NSPCC) contains information about the stages of typical sexual development and behaviour for different age groups.
While the behaviour of some pre-adolescent children may be ‘problematic’, it is seldom intentionally abusive. Many pre-adolescent children displaying harmful sexual behaviour have been sexually abused or exposed to developmentally inappropriate sexual experiences, such as seeing pornography. Their behaviour may be a way of communicating what has happened to them or an indirect response to other factors in their lives, including other forms of trauma and neglect.
The early teens are the peak time for the occurrence of harmful sexual behaviour. The vast majority of adolescents who display such behaviour are male, but it is rare for research or practice to focus on the significance of gender.
Most research has been conducted with criminal justice or ‘clinical’ populations and has repeatedly found that boys who have committed a sexual offence, or have been referred to specialist services because of concerns about their behaviour, generally have other major difficulties in their lives; these include experience of physical or sexual abuse or neglect, witnessing domestic violence, or having parents with mental health or substance abuse issues. Adverse childhood experiences tend to be more strongly linked to antisocial behaviour in males than in females.
Adolescents displaying abusive or violent sexual behaviour are, like their peers whose offending behaviour is non-sexual, likely to have low self-esteem, poor social skills and difficulties with anger, depression and peer relationships.
When harmful sexual behaviour involves siblings, it may occur within a context of family violence and neglect. Compared with other intra-familial abuse, it may occur more often and over longer periods, and be more likely to involve intrusive and penetrative acts.
It is increasingly recognised that some forms of sexual harassment and abusive behaviours between adolescents are so commonplace in schools and colleges that some young people may regard them as ‘normal’. Higher levels of general antisocial behaviour tend to be shown by adolescents who behave in sexually harmful ways towards their peers, compared with those whose harmful sexual behaviour targets younger children.
Children and young people with learning disabilities are more vulnerable both to being sexual abused and to displaying inappropriate or problematic sexual behaviour; in one large UK study, 38% of under-18s referred to specialist services because of harmful sexual behaviour were assessed as having a learning disability. However, it is likely that the high level of adult supervision of children and young people with learning disabilities means that their sexual behaviour is more likely to be observed and problematised.
Reasons why some children and young people with learning disabilities may be more likely to display harmful sexual behaviour include having less understanding that some sexual behaviours are not acceptable, and fewer opportunities to establish acceptable sexual relationships; receiving less sex education; struggling with social skills; and relating more easily to children younger than themselves.
While research suggests that individuals with autism spectrum disorders are not at increased risk of offending generally, a proportion of harmful sexual behaviours in individuals with autism may result from specific difficulties in understanding what other people may be thinking or feeling.
Most research into harmful sexual behaviour is based on male populations or includes only small numbers of girls. However, studies have found that girls and young women displaying abusive sexual behaviour are likely to have experienced more victimisation (including intra-familial sexual abuse, other forms of abuse and frequent exposure to family violence) than boys. Two UK studies found that, compared to boys, girls who sexually harmed had typically experienced more chronic and extensive maltreatment in childhood, had been sexually abused at an earlier age and were more likely to have been abused by more than one person.
Harmful sexual behaviour tends to be identified at a younger age in girls than in boys, and tends to involve younger victims. It is relatively rare for girls’ abusive sexual behaviour to involve the use of physical force. Girls displaying harmful sexual behaviour are less likely than boys to be charged with an offence, in part because they and their victims tend to be younger – but, like boys who display harmful sexual behaviour, they often have difficulties in school and relatively high levels of learning difficulties.
Girls’ Talk (Barnado’s) is a resource pack for practitioners supporting girls who have displayed harmful sexual behaviour to develop healthy sexual relationships.
All incidents of harmful sexual behaviour require an immediate and appropriate response. Practitioners becoming aware of incidents of harmful sexual behaviour must act appropriately to support and protect both children who have displayed the behaviour and those who have been impacted by the behaviour. Practitioners should discuss with their safeguarding lead whether a referral to children’s social care should be made (see Referrals chapter) Where a child is in immediate danger or a possible criminal offence has been committed, the police must be notified. Where there is an imminent risk of serious harm, steps may be need to ensure the child’s immediate protection (see Immediate Protection chapter).
Keeping Children Safe in Education part Five: Child on Child Sexual Violence and Sexual Harassment (Department for Education) sets out specific guidance for educational establishments. Locally, CABS (Child and Adolescent Harmful Behaviour Service) can support children and young people in Oxfordshire and Buckinghamshire about whom there are concerns in relation to harmful sexual behaviour (HSB).
For information on assessments, see Assessments chapter. Specific considerations will apply in cases of harmful sexual behaviour. In all cases it is important to undertake an holistic assessment which gives as clear a view as possible about the child or young person’s sexual behaviours and the degree to which, for a child of that age, they should be considered healthy, inappropriate, problematic or abusive.
Harmful Sexual Behaviour among Children and Young People (NICE) distinguishes between early help assessments and more specific HSB risk and needs assessments.
The NICE guidance states that an ‘early help’ assessment is warranted when a child’s sexual behaviours are indicated at the level of ‘inappropriate’ on the continuum. NICE suggests that a designated lead practitioner acts as a single point of contact for the child and family, coordinates early help and develops a care plan to deliver agreed actions. A NICE early help assessment would take into account the child or young person’s development status, gender identity and any neurodevelopmental or learning disabilities. The purpose of the assessment is to ascertain whether the child’s needs can be met by universal services or whether a referral for a more specialist HSB risk and needs assessment is necessary. Early help may help to prevent escalation of sexual violence.
For children and young people whose sexual behaviours are more indicative of abusive and violent categories on the continuum model, a more specific assessment of risk and need is likely to be required. NICE recommends that professionals responsible for risk assessments should use age-appropriate assessment tools, taking into account the child or young person’s age, neurodevelopmental disabilities, learning disabilities and gender identity. Whichever tool is used, effective assessment practice should include holistic, child-focussed, multi-agency assessments that examine the needs met by the behaviour, any underlying reasons or triggers, and protective factors and strengths that can be used to manage or reduce HSB.
It is vital to assess parental capacity to protect their children, the ability to manage a safety plan, and their capability to meet the needs of their children while considering the wider demands on the family.
Interventions are required to deal with a highly diverse group of children and young people and their families. Interventions should be tailored to the specific needs of the child and family, rather than applied routinely to all. Research suggests that a tiered approach to intervention is most appropriate, which distinguishes children and young people whose needs can be met through parental monitoring, through those who need limited psycho educative support, from those who would benefit from more specialist intervention services and placements.
Effective support should target presenting sexual behaviour problems as well as broader issues in the child or young person’s early experience (unresolved trauma, experiences of abuse, family issues). Resilience models aim to mobilise the child or young person’s strengths and reduce the risk of repeat harmful sexual behaviour by helping them develop positive relationships and pro-social ambitions.
RELATED CHAPTERS
RELATED INFORMATION
CONTENTS
The Crown Prosecution Service defines ‘honour’ based abuse as ‘an incident or crime involving violence, threats of violence, intimidation coercion or abuse (including psychological, physical, sexual, financial or emotional abuse) which has or may have been committed to protect or defend the honour of an individual, family and / or community for alleged or perceived breaches of the family and / or community’s code of behaviour.’
It can be a collection of practices, which are used to control behaviour within families or other social groups to protect perceived cultural and religious beliefs and / or so-called ‘honour’. Such violence and abuse can occur when perpetrators perceive that a relative has shamed the family and / or community by breaking their code of ‘honour’.
Victims are usually girls or women, but not exclusively so. Males may also be victims.
HBV is a violation of human rights; it may also be a form of domestic and / or sexual violence. There is no honour or justification for abusing the human rights of others, nor can there be. There is no specific offence of ‘honour’ based abuse. It is an umbrella term to encompass various offences covered by existing legislation.
Behaviour by a child which may be deemed by their family / community as breaching their code of ‘honour’ include:
Males may be targeted either by the family of a female who they are believed to have ‘dishonoured’, in which case both parties may be at risk, or by their own family if they are believed to be homosexual.
HBV is not a crime which is solely perpetrated by men; sometimes female relatives will support, incite or assist. It is also not unusual for younger relatives to be selected to undertake the abuse as a way to protect senior members of the family. Sometimes contract killers can be employed.
Shame may persist for a long time after the incident that was deemed to be dishonourable occurred. This may result in a new partner of a victim, their children, associates or siblings also being at risk.
‘Honour’ based abuse usually involves threats, intimidation and violence in an effort to get the victim to conform to the desired behaviour. These can escalate where deemed to be unsuccessful. On occasion, it may result in murder, which may involve premeditation, family conspiracy and a belief that the victim deserved to die.
In addition to information in Section 2, Common Triggers, incidents that may precede a killing include:
In some circumstances a victim’s immigration status may be used to dissuade them from seeking assistance from authorities.
Victims may suffer in isolation, resulting in depression and attempt suicide.
When dealing with potential victims of ‘honour based abuse’, it is essential that practitioners understand the seriousness of the situation and that immediate, but discreet, action is required (see Referrals and Immediate Protection chapters).
If a child discloses that they, or someone else, are at risk of ‘honour’ based abuse, the professional should:
Immediate steps must be taken as appropriate to ensure the immediate safety of the child. Consideration should be given to any other children in the family and their immediate safety.
Practitioners should ensure that they make a full record of all discussions, with whom these take place and any actions taken including referrals to other agencies. They should also seek support from their manager or safeguarding lead as per their agency protocol
Victims are sometimes persuaded to relocate under false pretences, where the intention may be to either stop them from contacting the authorities or to kill them. If a child is taken abroad, the Foreign and Commonwealth Office may assist in repatriating them back to the UK.
Practitioners should not approach the family or community leaders, share any information with them or attempt any form of mediation.
RELATED POLICIES
Concealed Pregnancy and Pre-Birth Safeguarding
RELATED GUIDANCE
Parental mental health problems (NSPCC)
Parenting and mental health problem (MIND)
Think child, think parent, think family: A guide to parental mental health and child welfare (SCIE)
Oxford Health NHS Foundation Trust provide services such as psychological services, Adult Mental Health Teams (AMHT), complex needs service, Bucks Community Eating Disorders Team (BCEDT) and adult mental health inpatient services.
CONTENTS
This procedure has been written to improve the coordination and communication between all agencies in Buckinghamshire engaged with children and families and those adults who have mental health needs.
The procedure should be applied whenever there are concerns about the well-being or safety of children whose parents or carers have mental health needs, specifically where these difficulties are impacting, or are likely to impact, on their ability to meet the needs of their children. This procedure also applies to pregnant women who have mental health problems or where their partners are known to have mental health problems.
The Final Analysis of Serious Case Reviews (2017 to 2019) published by the Department for Education reported that 55% involved parents with mental health problems. In these cases, the mental illness of the parent had a significant impact on their parenting capacity, resulting in the death or serious injury of the children. However, it remains the case that the majority of mentally ill parents do not harm their children. It also does not mean that parents who experience mental health problems have poor parenting skills.
However, the impact of parental mental health problems can, on some occasions, lead to children and families needing additional support; or, in a small number of cases, support and multi-agency action to prevent significant harm.
The guidance is underpinned by the following principles:
Here are some messages to mental health professionals written by young people from a Barnardo’s project in Liverpool2. The messages show how important it is to keep children informed.
Tell us if there is anyone we can talk to. MAYBE IT COULD BE YOU.
Mental ill health can sometimes lead to neglect of both the adults and their children’s physical, emotional and social needs. The children may have caring responsibilities, which are inappropriate to their age and may have an adverse impact on their development. Some forms of mental ill health may cause adults to be ‘unavailable’ or not responsive to the child; or to behave in bizarre, unpredictable or violent ways towards themselves, their children or environment.
The stigma and oppression associated with adult mental ill health can impair the adult’s ability to care for the child/ren and children can carry the burden of covering for parental behaviour. It can be difficult for adults to share their situation and struggles. Children may be reluctant to talk about family problems or seek support. Practitioners need to be sensitive to this. See also Section 4, Consider the Child / Children’s Experience – What is Life Like for the Child?
At the extreme, a child may be at risk of severe injury, profound neglect or even death.
An adult carer’s mental ill health will be less likely to have an adverse effect on a child when:
A significant history of violence is a risk indicator for children, as is parental and adult non- compliance with services and treatment.
Children most at risk of significant harm are those who:
The following factors may impact the ability of an adult to provide appropriate care and increase concerns that a child may have suffered, or is at risk of suffering, significant harm:
When an agency identifies a pregnant woman experiencing mental health problems, an assessment must be undertaken to determine what services she requires and the Concealed Pregnancy and Pre-Birth Safeguarding procedure must be followed.
This must include gathering relevant information from their Primary Care Team/GP, in addition to any other agencies involvement, to ensure that the full background is obtained about any existing or previous diagnosis, or treatment for mental illness or substance misuse. This is especially important where service awareness of earlier births may need to be clarified, for example, in the case of older or overseas children. If a person has moved recently, it is advisable to seek out health records from the previous Primary Care Team/GP. It is also important to identify partners of pregnant women who have mental health or substance misuse problems.
Pregnant women in Buckinghamshire now book their maternity appointments online and these are coordinated by midwives based at the hospital and not by Primary Care Teams/GPs. As such, it is possible that a pregnant woman may not see her GP during the pregnancy and the first contact with their GP may be at the face-to-face six-week post-natal appointment. It is important that those working with pregnant women do not assume that the pregnant women are being routinely seen by their GP.
Research has shown that pregnant women with a previous history of mental health needs are particularly vulnerable to breakdown during the later stages of pregnancy and following the birth of their baby.
When a parent has a substance misuse problem, as well as mental health needs, this can put the child at particular risk, especially where the potential for dealing with the substance misuse problem is limited. Where a parent/carer has mental health and substance misuse issues, the assessment of the adult should ideally be conducted in partnership between the Mental Health Care Management Team and the Adult Substance Misuse Care Management Team.
In addition, the Final Analysis of Serious Case Reviews (2017 to 2019) and previous reviews of Serious Case Reviews have shown that the three issues of domestic abuse, parental mental ill health, and alcohol or substance misuse are not the only risk factors that may contribute to cumulative risk of harm. Other risk factors often co-exist with these factors, and potentially interact with them to create harmful environments for the children. These include issues such as adverse experiences in the parent/carer’ own childhoods, a history of criminality – particularly violent crime, a pattern of multiple consecutive partners, and acrimonious separation. Professionals should be aware of this when undertaking an assessment of risk.
This flowchart is relevant to all services in Buckinghamshire which are treating or providing any kind of service to parents, carers, or pregnant women with mental health problems.
Informed assessments and effective multi-agency/disciplinary working are the key to ensuring that children and families receive the appropriate services to meet their identified needs and manage risk.
The key to ensuring children are safe, protected, and their needs are being met where parents/carers have additional needs, is to assess parent’s/carers capacity and ascertain if additional support is required. Consider the following areas:
Are parents/carers able to provide the following:
BASIC CARE
ENSURING SAFETY
EMOTIONAL WARMTH
STIMULATION
GUIDANCE AND BOUNDARIES
STABILITY
See Continuum Of Need Threshold for further information.
If there is concern about the mental health needs of a parent/carer, the adult’s Primary Cary Team/ GP should be contacted in the first instance and a request made for information to be shared regarding any existing or previous diagnosis of mental illness, and previous or current treatment or referrals.
In order for timely sharing of this information, the Primary Care Team will need to know why the information is needed, in what timescale it needs to be provided, with whom the information will be shared (within health professionals or with other agencies), what information is being asked and whether the patient has consented to this information being shared.
Practitioners should be aware that women in Buckinghamshire who are temporarily placed in refuges may be additionally vulnerable to their mental health needs not being met and patient information between systems may be limited.
If there is an imminent danger to the person or others, including a child, the police must be contacted. Staff must ensure that their decision and agreed course of action is fully and accurately documented.
Triggers that may indicate a referral to adult mental health services for initial assessment is needed are listed below. However, this is not an exhaustive list and is provided to assist professional decision-making.
Concerns should be discussed with the person’s Primary Care Team/GP in order to agree the most appropriate course of action. It would be usual practice for the Primary Care Team/GP to assess the client in the first instance and make a referral to mental health services if appropriate. However, in some circumstances another professional may make the referral, or the client may self-refer.
A past history of mental health problems will not necessarily mean a referral is required; this will depend on what the particular diagnosis was, current mental state, how long an individual has been stable and the level of support at home.
In any instance where there is a concern about the welfare of a child, professionals should consult the Continuum of Need Threshold.
A referral to Children’s Social Care for an initial assessment or pre-birth assessment should always be made if a parent, carer or pregnant woman is considered to have significant mental health problems, as indicated by the triggers given below. A referral should always be discussed with a manager.
If there is an imminent danger to the person or others, including a child, the police must be contacted.
Speak to the family to discuss the concerns and reasons for referral. Gain a better understanding of the situation and gain consent to refer if possible.
Think family – consider all family members including all the children. Risks may be relevant to some or all of the children in the family.
Consideration should be given to a referral to Early Help in order to provide additional support and safeguard children at an early stage. Early Help in Buckinghamshire is provided by the Family Support Service.
Consider schools involvement – what support is school offering? Are they aware of the family situation? Is the school counsellor involved? Is the child’s school attendance level a concern?
Triggers that indicate referral to Children’s Social Care are listed below. However, this is not an exhaustive list and is provided to assist professional decision-making.
Where a parent or carer expresses thoughts of self-harm, an assessment of risk to the child or unborn baby must be made and consideration given to a referral to Children’s Social Care based on the level of risk. Management of self-harm risk by adult mental health services staff must include in the plan actions to support the needs of the child/children/unborn baby and there should be discussion with the organisation’s lead for child safeguarding. Where necessary, advice should be sought from First Response. Consideration must always be given to the care arrangements for the children should the adult need to be admitted to hospital.
When a parent or carer has been receiving inpatient services, in whatever setting, consideration must be given to discharge arrangements to ensure provision for the children is appropriate, and their welfare and safety has been properly assessed. A formal meeting with Children’s Social Care should be held where they are already involved or if concerns are identified. If a parent or carer discharges themselves out of hours, a referral to the Emergency Duty Team should be made to ensure the children’s welfare is protected.
Newly identified risk or changes in the risk assessment in any agency must be communicated to other relevant agencies in order that they can consider if this new information impacts on their own risk assessments. Staff must always consider that a change for one member of the family might have impact on another member, and that a Think Family approach is essential.
Where the need for referral to Children’s Social Care is unclear, this must be discussed with a line manager and/or safeguarding lead. Children’s Social Care can be consulted for advice. Staff must ensure that all decisions and the agreed course of action are signed and dated. If a referral is not made, the reasons must also be clearly documented.
All information should be shared in line with Information Sharing Advice for Safeguarding Practitioners (Department for Education).
It is essential that staff working in adult mental health and children’s services work together to ensure the safety of the child and the management of the adult’s mental health.
Joint work will include mental health workers providing all information with regards to:
Parents/Carers with mental health issues entrust professionals with, or allow them to gather, sensitive information relating to their health and other matters as part of their seeking treatment. They do so in confidence, and they have legitimate expectation that staff will respect their privacy and act appropriately.
Where there are concerns about the wellbeing of a child, the need to share information will take precedence over the patient’s right to confidentiality. However, practitioners need to consider what information is and is not confidential, and the need in some circumstances to make a judgement about whether confidential information can be shared, in the public interest, without consent.
Sensitive information can be shared if there is a clear and justifiable purpose, and consideration has been made of the safety and wellbeing of the child and others who may be affected. The more sensitive the information, the greater the child focus needs to be in order to justify sharing.
The practitioner needs to be mindful that information may need to be shared with a number of agencies, therefore the ‘need to know’ and ‘proportionality to the risk of harm’ principles apply. Where a practitioner is considering the inclusion or exclusion of sensitive information, or consent has been refused, they must discuss this with their safeguarding lead within their organisation.
If an adult’s clinical information is shared without their consent, the adult should be notified of this.
Child protection workers must assess the individual needs of each child and, within this, incorporate information provided by mental health workers. They must assess the risk and impact on each child in accordance with information provided by mental health workers and the assessment framework.
Mental health professionals must attend and provide information to any meeting regarding the potential impact of parent/carer mental health concerns on the child. These will include:
Relevant professionals from Children’s Services and other agencies supporting the child should attend Care Programme Approach (CPA) and other meetings related to the management of the parent/carer’s mental health where concerns about capacity to parent have been raised.
All plans for a child, including Child Protection Plans, will identify the roles and responsibilities of mental health and other professionals. The plan will also identify the process of communication and liaison between professionals. All professionals should work in accordance with their own agency procedures/guidelines and seek advice and guidance from line management when necessary.
Key examples of good practice in joint working:
Consideration to be given to the adult’s accommodation history, have they always lived in Buckinghamshire, have the child/children been known in another local authority?
It is important to be aware that risk assessment in mental health work and risk assessment in child protection work are two different concepts, and it can be dangerous to confuse them.
The former is concerned with predicting the likelihood of a patient’s mental health deteriorating to the point where she/he poses a risk to self and/or others. The latter involves the analysis of information to consider whether or not the children’s likely experiences are acceptable, in terms of risk of physical or sexual assault, omission of care or neglect, or threat to emotional wellbeing.
Newly identified or changes in risk in one agency’s assessment must be communicated to other relevant agencies, so that they too can consider if this new information impacts on their own risk assessments. Staff must always consider that a change for one member of a family might have impact on the other member – a ‘think family’ approach is essential.
In the event of a dispute or disagreement arising between professionals, the procedure for Escalation, Challenge and Conflict Resolution should be followed.
Any disagreements or differences should be recorded on the case file, including the views of the other party.
CONTENTS
This guidance provides information about a range of mechanisms that are available when managing adults, or children and young people, who have been identified as presenting a risk, or potential risk, of harm to children.
Areas covered include:
The Children Act 1989 recognised that the identification and investigation of child abuse, together with the protection and support of victims and their families, requires multi-agency collaboration. This is rightly focused on the child and the supporting parent/carer. As part of that protection, action has been taken, usually by the Police and Children’s Social Care, to prosecute known offenders and/ or control their access to vulnerable children.
This work, while successful in addressing the safety of particular victims, has not always acknowledged the ongoing risk of harm that an individual perpetrator may pose to other children in the future. Nor does it acknowledge that a young person may also be a perpetrator and that the same young person may simultaneously be both suffering, and likely to suffer, harm, and also present a risk of harm to other children and young people.
The terms ‘Schedule One Offender’ and ‘Schedule One Offence’ were used to describe anyone convicted of an offence against a child listed in Schedule One of the Children and Young Person’s Act 1933. However, since the Sex Offences Act 2003, these offences are now known as Schedule 3 (all sex offences) or Schedule 5 (violent offences). A conviction for an offence in the schedules does not trigger any statutory requirement in relation to child protection or safeguarding children issues, and inclusion on the schedule was determined solely by the age of the victim and offence for which the offender was sentenced, and not by an assessment of whether the offender may pose a future risk of harm to children.
The ‘Schedule One Offender’ has been replaced with ‘Risk to children’. This clearly indicates that the person has been identified as presenting a risk, or potential risk, of harm to children.
Practitioners working in this area should use the Sexual Offences Act as a ‘trigger’ for a further assessment, including consideration of previous offences and behaviours, to determine if an offender should be regarded as presenting a continuing risk of harm to children. This allows agencies to focus resources on the correct group of individuals, and not include those who have been identified solely because a child was harmed during the offence, for example, as in the case of a road traffic accident.
An offender who has harmed a child might not continue to present a risk or harm towards that child or other children. Where a child or young person (aged under 18 years) offends against another child, a thorough and specialist assessment should be undertaken to establish the extent to which the young person who has offended continues to pose a risk of harm to other children and young people. They should be alert to the possibility that there may be little or no continuing risk of harm to other children and young people, but never losing sight of taking all possible actions to ensure that children are adequately protected from any future harm. Practitioners should also assess and put in place services to respond to the, often complex, needs of the young person who has offended.
Once an individual has been sentenced and identified as presenting a risk of harm to children, agencies have a responsibility to work collaboratively to monitor and manage the risk of harm to others. Where an offender is given a community sentence, Offender Managers or Youth Justice Support Team (YJST) workers will monitor the individual’s risk of harm to others and their behaviour and liaise with partner agencies as appropriate. The YJST monitors the risk of harm to others and works with other known agencies to manage that risk by holding regular Risk Management Panels (RMPs).
In cases where an offender has been sentenced to a period of custody, prison establishments undertake a similar responsibility and, in addition, notify other agencies prior to any period of release. Similarly, for offenders released on licence into the community who are assessed as potentially presenting a risk of harm to children, consideration will be given to including licence conditions which seek to prevent the offender’s contact with children.
The Sexual Offences Act 2003 introduced offences to deal with those who sexually exploit children and young people. The offences protect children up to the age of 18 and can attract tough penalties. They include:
These are not the only charges that may be brought against those who sexually exploit children or young people. Abusers and coercers often physically, sexually and emotionally abuse these children, and may effectively imprison them. If a child is a victim of serious offences, the most serious charge that the evidence will support should always be used.
See also Multi Agency Public Protection Arrangements chapter.
MAPPA provides a national framework in England and Wales for the assessment and management of the risk of serious harm posed by specified sexual and violent offenders, including offenders (including young people) who are considered to pose a risk, or potential risk, of serious harm to children. The arrangements are statutory. Sections 325–327 of the Criminal Justice Act 2003 require the police, prisons and probation services (the ‘Responsible Authority’) in each area to establish and monitor the arrangements. A number of other agencies – including Children and Adult’s Social Care services, Health, Housing, the YOS, Jobcentre Plus and electronic monitoring providers have a statutory duty to cooperate with the Responsible Authority in this work.
The focus of MAPPA is on specified sexual and violent offenders in, and returning to, the community, and its aims are to:
Offenders eligible for MAPPA are identified and information is gathered/shared about them across relevant agencies. The extent to which they pose a risk of serious harm is assessed and a risk management plan is implemented to protect the public.
Each area has a MAPPA Strategic Management Board (SMB) attended by senior representatives of each of the responsible authority and duty to cooperate agencies, plus two lay advisers. It is the SMB’s role to ensure that the MAPPA are working effectively, and to establish and maintain working relationships with the local Safeguarding Children Partnership.
MAPPA offenders are managed at one of three levels according to the extent of agency involvement needed and the number of different agencies involved:
Exchange of information is essential for effective public protection. The MAPPA guidance details how MAPPA agencies may/should exchange information among themselves to better manage offender It also explains why and how information may be disclosed to those not involved in the MAPPA management of the offenders. The expectation is that information on offenders will be disclosed to others – for example, partners, employers, schools – where this is required to manage the risks posed by the offender.
ViSOR (violent and sex offenders register) is a national database which currently carries details of MAPPA eligible offenders and other potentially dangerous individuals. All three responsible authority agencies (police, probation and prisons) can access the same IT system, thus improving the quality and timeliness of risk assessments and of interventions to prevent offending.
The National Probation Service assess risk of serious harm using the offender management system (OASys), supplemented by additional assessment procedures, depending on the nature of the offending and the specific risks identified. The Youth Justice Board uses AssetPlus for under-18-year-olds. The levels of risk are:
Risk is categorised by reference to the potential subject of the harm. This includes children who may be vulnerable to harm of various kinds, including violent or sexual behaviour, emotional harm or neglect. In this context, MAPPA works closely with local safeguarding children partnerships to ensure the best local joint arrangements can be made for any individual child being considered by either setting.
In most cases, a MAPPA eligible offender will be managed without recourse to MAPPA meetings under the ordinary arrangements applied by the agency or agencies with supervisory responsibility. This will generally be the Police for registered sexual offenders who are not on a licence to Probation, and Probation for violent offenders and those on a licence; but the YJST will lead with young offenders and Mental Health services with those on Hospital Orders. A number of offenders, however, require active multi-agency management and their risk management plans will be formulated and monitored via MAPPA meetings attended by various agencies.
There are three levels of management within the MAPPA framework, based on the level of multi-agency co-operation required to implement the risk management plan effectively:
Offenders will be moved up and down levels as appropriate.
The YJST has a duty to identify cases that meet MAPPA criteria and make appropriate referrals. However, the guidance emphasises that young people should be assessed and managed differently from adults, using age-appropriate assessment tools and always bearing in mind the need to safeguard the welfare of the young offender as well as to protect others from harm. Children’s Social Care should always be represented at MAPPA meetings when a young person is being discussed.
For more information, please see the MAPPA Guidance.
A MARAC is a multi-agency meeting focusing on the safety of high-risk victims of domestic abuse. The identification of high-risk victims has been made possible by a risk identification tool, for use across a wide range of agencies. This has permitted practitioners, both within and outside of the criminal justice system, to identify high-risk victims of domestic abuse. As a result, many more high-risk victims are being identified and, in response, the MARAC has been rolled out across England and Wales.
The MARAC is a process involving all the key statutory and voluntary agencies who might be involved in supporting a victim of domestic abuse. This includes those from the criminal justice system, those supporting children, those from the health service, the local authority, housing, substance misuse and, critically, specialist domestic abuse services, most frequently in the form of an Independent Domestic Violence Adviser (IDVA). The IDVA is a specialist caseworker who receives accredited training to work with high-risk victims of domestic abuse from the point of crisis, and whose focus is very much on the MARAC.
At a typical MARAC meeting, 15 to 20 high-risk cases are discussed in half a day, with a very brief and focused information-sharing process followed by a simple multi-agency action plan being put into place to support the victim and to make links with other public protection procedures, particularly safeguarding children, vulnerable adults and the management of perpetrators.
It is important to understand that the MARAC meeting is part of a wider process which hinges on the early involvement and support from an IDVA and continued specialist case management, both before and after the meeting. The MARAC should combine the best of specialist support together with the co-ordination of the generic agencies whose resources and involvement will be needed to keep victims and their children safe.
Where an offender is being managed at MAPPA Level 2 or Level 3, to avoid duplication of effort and resources, the MAPPA meeting should take the lead over the MARA This is because the MAPPA is a statutory set of arrangements and therefore it takes precedence over the MARAC.
For more information, see Multi Agency Risk Assessment Conference (MARAC) chapter.
Rehabilitation of offenders is the best guarantee of long-term public protection. A range of independently accredited treatment programmes, which have been developed or commissioned by the National Offender Management Service (NOMS), have been tried and tested at a national level. Examples include sex offender treatment programmes, programmes for offenders convicted of internet-related sexual offences, and programmes for perpetrators of domestic abuse.
The Disclosure & Barring Service (DBS) was formed when the Criminal Records Bureau (CRB) and Independent Safeguarding Authority (ISA) merged in 2012. The DBS holds two lists (‘Barred Lists’) of those individuals that are barred from working with (a) children and (b) vulnerable adults. It is responsible for deciding whether an individual should be included on one or both of those lists. Employers and agencies have a duty to refer to the DBS any information about individuals they believe may pose a risk of harm to children or vulnerable adults, ensuring potential threats to vulnerable groups can be identified and dealt with.
It is a criminal offence for barred individuals to seek or take up regulated activity (see definition below) with vulnerable groups, and for employers or agencies to knowingly employ/engage barred staff.
DBS checks (formerly known as CRB checks) provide information about an individual’s criminal record (if appropriate). DBS certificates are required for people applying for jobs which are defined as ‘regulated positions’.
The definition of ‘regulated activity’ for work with children is different to that of work with vulnerable adults. DBS checks sought for individuals undertaking regulated activity also include checks to see if a person is included on any lists held by the DBS of people who are barred from undertaking regulated activity with children and young people.
The revised definition of ‘regulated activity’ which determines eligibility for a DBS check is:
Roles requiring standard or enhanced DBS checks are exempt from the Rehabilitation of Offenders Act 1974, which means that all criminal information is provided about an applicant, even if it would otherwise be regarded as ‘spent’. An enhanced DBS check may also include relevant information the Police have on record, even if it has not resulted in a caution or conviction (for example if allegations have been made and reported to the Police).
Having a criminal conviction does not in itself bar a person from work with children or young people. If a DBS check discloses convictions or relevant information, an employer has to decide whether a person is suitable to be employed in the role concerned.
Organisations should have a policy for the recruitment of ex-offenders (a model version is available) which aims to ensure that all applicants are given fair and transparent consideration for employment.
A referral must be made to the DBS when the following two conditions have both been met:
Condition one – permission is withdrawn for a person to work in regulated activity with children and/or adults either through dismissal or by moving the person to another area of work that is not regulated activity. This includes situations where an employer/volunteer manager would or may have dismissed the person or moved them to other duties, if the person had not resigned, retired or otherwise left their work. For example, a teacher resigns when an allegation of harm to a student is first made. The head teacher establishes that harm did occur, or was at risk of occurring, and decides that they may have dismissed the person had they not left and so makes a referral to the DBS.
Condition two –there is a belief that a person has carried out one of the following:
The DBS will consider whether to bar a person in any of those circumstances. Referrals should be made as soon as possible after the resignation or removal of an individual.
For more information see Disclosure and Barring chapter.
By virtue of the Sexual Offences Act 2003 (Notification Requirements) (England and Wales) Regulations 2012, the Home Office has introduced measures which will extend and strengthen the system of notification requirements placed on registered sex offenders (commonly referred to as the sex offenders’ register).
A person required by the 2003 Act to register with the Police is required by law to:
An offender can only give this notification by attending a Police station prescribed for the purpose by regulations (the regulations will be periodically updated when the addresses of Police stations change).
Offenders should be asked when initially notifying the Police whether there are any addresses (such as any described in the fourth bullet above) which they regularly visit and told that they are required to notify them if they begin to visit other addresses.
Offenders should be reminded when initially notifying the Police of their names and addresses that they are also required to notify any plans to leave the UK for any periods (a separate form [Form 3317] is available for recording this information).
New name and address: For advance notification if the change takes place more than two days before the anticipated date, the Police must be informed. If an advance notification is made and the change has not taken place within three days beginning with the anticipated date, the Police must be informed within six days of the anticipated date.
A person failing to comply with the requirements of the Sexual Offences Act 2003, without reasonable excuse, or who provides the Police with information which is known to be false, could be sent to prison for up to five years.
If an individual is found to have convictions for sexual offences against children and poses a risk of causing serious harm, there is a presumption that this information will be disclosed to the person who is best placed to protect the child or children, where it is necessary to do so for this purpose.
It should be noted that, under the scope of the Disclosure Process, the presumption for disclosure will only exist in cases where the individual has convictions for child sexual offences. However, it is felt that to restrict access to information regarding convicted child sexual offenders would severely limit the effectiveness of the process and ignore significant issues regarding offences committed against children.
It is important that the disclosure of information about previous convictions, for offences which are not child sex offences, is able to continue as it is not the intention of the Disclosure Process to make access to information concerning safeguarding children more restricted.
It is of paramount importance to all involved in delivering this process to ensure that children are being protected from harm. By making a request for disclosure, a parent, guardian or carer will often also be registering their concerns about possible risks to the safety of their child or children. For that reason, it is essential to this process that police forces, Children’s Social Care and local safeguarding children partnerships work closely together to ensure that any possible risks of harm to the child or children are fully assessed and managed.
For further details please see Child Sex Offender Disclosure Scheme chapter.
Notification Orders are intended to ensure that British citizens or residents, as well as foreign nationals, can be made subject to the notification requirements (the Sex Offenders Register) in the UK if they receive convictions or cautions for sexual offences overseas. The provisions also apply to young people who have offended.
Notification Orders are made on application from the Police to a Magistrates’ Court. Therefore, if an offender is identified who has received a conviction or caution for a sexual offence overseas, the case should be referred to the local Police for action.
If a Notification Order is in force, the offender becomes subject to the requirements of the Sex Offenders Registration. For example, a Notification Order could ensure that the notification requirements apply to a British man who, while on holiday in South East Asia, received a caution for a sexual offence on a child.
Any information that an individual has received a conviction or caution for a sexual offence overseas should, where appropriate, be shared with the Police.
Sexual Harm Prevention Orders and Sexual Risk Orders were introduced by the Anti-Social Behaviour, Crime and Policing Act 2014. They replace the previous Sexual Offences Prevention Orders, Risk of Sexual Harm Orders and Foreign Travel Orders which were introduced by the Sexual Offences Act 2003.
Sexual Harm Prevention Orders can be applied to anyone convicted or cautioned of a sexual or violent offence, including where offences are committed overseas.
The Court needs to be satisfied that the order is necessary for protecting the public, or any particular members of the public, from sexual harm, or protecting children from sexual harm from the defendant outside the UK.
Violent Offender Orders (VOOs) are civil preventative orders that came into effect in 2009 (contained in Part 7 of the Criminal Justice and Immigration Act 2008).
VOOs were developed as a tool to help the Police manage those offenders who continue to pose a risk of serious violent harm to the public, even after their release from prison or when their licence has ceased. Although not specifically designed as a tool to protect children, there may be circumstances where VOOs would be an appropriate mechanism to manage an individual who poses a serious risk of harm to children.
VOOs are available on application by a chief officer of Police to a Magistrates’ Court and, if granted, will contain such restrictions, prohibitions or conditions authorised by Section 102 of the Act as the Court considers necessary to protect the public from the risk of serious violent harm caused by the offender. This may include prohibiting their access to certain places, premises, events or people to whom they pose the highest risk.
Breach of any of the prohibitions, restrictions or conditions contained in a VOO without reasonable excuse is a criminal offence, with a maximum punishment of five years’ imprisonment.
Support for Parents and Carers to Keep Children Safe Online (gov.uk)
Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) – guidance on responding to incidents and safeguarding children and young people.
Guidance: Education for a Connected World (UK Council for Internet Safety) – a framework to equip children and young people for digital life
Guidance: Challenging Victim Blaming Language and Behaviours when Dealing with the Online Experiences of Children and Young People (UK Council on Internet Safety) – guidance for professionals on how to effectively challenge victim blaming language and behaviours and advice on best practice
Ofcom Protection of Children Codes of Practice and Guidance
Internetmatters.org – supporting children’s online safety
February 2026: Information has been added on Ofcom’s Protection of Children Codes of Practice and Guidance, and guidance for professionals on Child Sexual Abuse Material Generated by Artificial Intelligence (NCA, CEOP, IWF). See Related Guidance.
Information on ways in which Artificial Intelligence (AI) is being used to create indecent images of children has also been added, as well as advice on how to respond when children and young people use AI in this way to create images of their peers. Advice on ways practitioners can support children and young people with special educational needs and disabilities (SEND) has been added into Apps to help children stay safe online.
CONTENTS
Technology is a big part of everyday life, bringing educational and social benefits and opportunities for children and young people. However, there are potential harms which children and young people may encounter when online, including online child abuse, bullying, harassment or criminal exploitation. The consequences and impact of online child abuse can be just as severe as abuse experienced offline.
The term ‘victim’ has been used within this chapter to describe a child or young person who has experienced online abuse, in any form. This includes abuse from an adult, or another child or peer. In practice, different terms may be used, for example victim or survivor. Many children or young people who have experienced online abuse would not consider themselves a victim, and would not refer to themselves as such.
In line with the Online Safety Act 2023, Ofcom has published Protection of Children Codes of Practice and Guidance. Providers of online services (such as social media sites and websites) that are likely to be accessed by children in the UK, are legally required to protect children from content that is harmful to them, including checks on their age. Any site which hosts pornography or content which encourages self-harm, suicide or eating disorders must have robust age checks in place to protect children from accessing that content. Additional detail on how staff can support children and young people with special educational needs and disabilities (SEND) to stay safe online has also been added. See Apps to help children stay safe online.
The breadth of issues classified within online safety is considerable and ever evolving. Keeping Children Safe in Education Part Two: The Management of Safeguarding (Department for Education, 2025) categorises them into four areas of risk (‘the 4Cs’):
The Sexual Offences Act 2003 and the Online Safety Act 2023 set out several criminal offences in relation to harmful online activity, and these should be reported to the police for investigation of possible criminal offences (alongside any safeguarding referral).
Some of the main categories of safeguarding risks are now considered in more detail.
See also Child Sexual Exploitation and Abuse (Including Organised Sexual Abuse) chapter.
Indecent images of children: Making, possessing, and distributing any imagery of someone under 18 which is ‘indecent’ is illegal. This includes images which have been created by using artificial intelligence (‘AI’), such as tools enabling the digital removal of clothing from images. As well as AI-generated images which are not photorealistic such as cartoons, illustrations and animations.
Sending a photograph or film of genitals (‘cyberflashing’): It is a criminal offence to intentionally send a photograph or film of any person’s genitals to another person either with the intention that the recipient will see the genitals and be caused alarm, distress or humiliation, or for the purpose of obtaining sexual gratification (inserted into the Sexual Offences Act 2003 by the Online Safety Act 2023).
Threatening / blackmailing children into sending indecent images / carrying out indecent acts online: This is an offence under the Sexual Offences Act 2003.
Sharing or threatening to share intimate photograph or film: This is a criminal offence under the Online Safety Act 2023. A person would ‘share’ the film/image if they, by any means, give or show it to another person, or make it available to another person. This includes electronic sharing, for example by posting a photograph or film on a website or emailing to someone. ‘Film’ or ‘photograph’ covers data that can be converted into such an image – for instance data stored on a hard drive or disc.
Sharing nudes and semi-nudes: Children may be encouraged, or may choose, to share nude or semi-nude images online with other children and young people.
Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) uses the term ‘sharing nudes and semi-nudes’ to mean the sending or posting of nude or semi-nude images, videos, or live streams by young people under the age of 18 online.
For example:
This could be via social media, gaming platforms, chat apps or forums. It could also involve sharing between devices via services like Apple’s AirDrop which works offline.
The sharing of nudes and semi-nudes can happen publicly online, in 1:1 messaging or via group chats and closed social media accounts.
Nude or semi-nude images, videos or live streams may include more than one child or young person. The term ‘nudes’ is used as it is most commonly recognised by young people and more appropriately covers all types of image sharing incidents. Alternative terms used by children and young people may include ‘dick pics’ or ‘pics’.
See also Section 3.2, Information on avoiding unnecessary criminalisation of children and:
The risk of physical and / or emotional harm can include the following.
Children being exposed to online threats and harmful online ‘fake news’
The Online Safety Act 2023 introduced offences of threatening communications and false communications.
A person commits the false communications offence if they send a message conveying information that they know to be false, intending the message to cause non-trivial psychological or physical harm to a likely audience (that is, someone who could reasonably be foreseen to encounter the message or its content). It is not necessary to show that the sender intended to cause the harm to any of the likely audience in particular.
A person commits the threatening communications offence if they send a message conveying a threat of death, serious injury, rape, assault by penetration, or serious financial loss. This includes situations where the recipient fears that someone other than the sender of the message may carry out the threat. It does not matter if the content of the message is created by the person who sends it; a message can consist of or include a hyperlink to other content.
Children being exposed to content designed to cause them physical and / or psychological harm
The Online Safety Act 2023 introduced offences of sending or showing flashing images electronically with the intention of causing harm to a person with epilepsy. The offence may be committed by a person who forwards or shares the electronic communication, as well as by the person originally sending it.
The Act also introduced an offence of encouraging serious self-harm. It includes online communications capable of encouraging or assisting another person to seriously self-harm. It also includes an omission, such as encouraging or assisting a person to stop eating or taking required prescription medication. The person committing the offence need not know, or even be able to identify, the person or persons who receive the communication. So, a person who intends that a recipient or recipients of their communication will seriously harm themselves is guilty of an offence, even though they may never know the identity of those who receive the communication.
An offence can be committed whether or not serious self-harm occurs. In addition, a person who arranges for someone else to do an act capable of encouraging or assisting the serious self-harm of another person will also be committing an offence if the other person carries out that act.
This category would also include cyberbullying.
Preventing Bullying: Guidance for Schools on Preventing and Responding to Bullying (Department for Education, 2017) provides further information on tackling this form of online harm.
Under the Sexual Offences Act 2003 (as amended) it is an offence for a person (over 18 years) to engage in sexual communication with a child (under 16 years) (section 15A), or to meet a child (under 16 years) following sexual grooming (section 15).
See also chapters on Child Sexual Exploitation and Abuse (Including Organised Sexual Abuse) and Multi-Agency Child Exploitation Protocol.
For further information see Radicalisation and Violent Extremism chapter
Concerns about online radicalisation can be reported to the police on 101 and / or a Prevent referral can be made, so that the victim can get safeguarding support.
Any member of the public can report terrorist content they find online through the gov.uk referral tool – more information about what to report and what happens when you do can be found on the Action Counters Terrorism campaign.
Educate Against Hate Parents’ Hub provides resources and government advice for parents and carers on keeping young people safe from extremism, including online.
The prevalence of online activity by children and young people makes it increasingly likely that children may be both victims and perpetrators of harmful online activity, which may involve the commission of criminal offences. An appropriate multi-agency response including police and safeguarding will be required in respect of all children involved. Children can abuse other children online. This can take the form of abusive, harassing, and misogynistic / misandrist messages, the non-consensual sharing of indecent images, especially around chat groups and the sharing of abusive images and pornography to those who do not want to receive such content. Child-on-child abuse can include cyberbullying, online threats of physical abuse, online threats and/or encouragement of sexual violence, online sexual harassment.
The nature of online abuse means that it can very rapidly involve multiple children, for example children sharing images online / forwarding on content, sending links of content to others and / or posting things on online platforms such as social media.
Children may create ‘nude’ images of their peers by using AI tools to digitally remove clothing from images. For further information see Child Sexual Abuse Material Generated by Artificial Intelligence: An Essential Guide for Professionals who Work with Children and Young People (NCA, CEOP, IWF).
See also Harmful Sexual Behaviour chapter
This is of particular relevance in relation to the sharing of nude / semi-nude images where both victim and perpetrator are under 18.
The law criminalising indecent images of children, for instance, was created to protect children and young people from adults seeking to sexually abuse them or gain pleasure from their sexual abuse. It was not intended to criminalise children and young people. The law was also developed long before mass adoption of the internet, mobiles and digital photography.
Despite this, children and young people who share nudes and semi-nudes of themselves, or peers, are breaking the law. Making, possessing, and distributing any imagery of someone under 18 which is ‘indecent’ is illegal. This includes imagery of the person making / sending the image if they are under 18.
Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) stresses the importance of avoiding unnecessary criminalisation of children. Situations should be considered on a case by case context, considering what is known about the children and young people involved and if there is an immediate risk of harm. Often, children and young people need education and support for example, on identifying healthy and unhealthy behaviours within relationships and understanding consent and how to give it. Safeguarding action will also be required in cases where there is risk of harm.
Investigation by police of an incident of sharing nudes and semi-nudes does not automatically mean that the child / young person involved will have a criminal record. Once an incident is reported to the police, they will investigate and decide on an appropriate outcome. If an incident is found to have abusive and / or aggravating factors, the child or young person may receive a caution or conviction.
To mitigate the risk of children and young people being negatively impacted, the police are able to record the outcome of an investigation using an ‘outcome 21’ code should an incident be found to be non-abusive and have no evidence of any of the following:
This means that even though a child or young person has broken the law, and the police could provide evidence that they have done so, the police can record that they chose not to take further action as it was not in the public interest.
It is possible for an incident of sharing nudes and semi-nudes recorded on police systems with outcome 21 to be disclosed on a DBS certificate. However, information falling short of conviction or caution can only be included on a DBS certificate when an individual has applied for an Enhanced Criminal Records Check. In such cases, it would be for a chief officer to consider what information (in addition to convictions and cautions held on the Police National Computer) should be provided for inclusion. That decision must be made on the basis that the chief officer reasonably believes the information to be relevant to the purpose of the disclosure (for example, someone taking up a position working with children) and considers that it ought to be included.
Keeping Children Safe in Education Part five: Child-on-child Sexual Violence and Sexual Harassment (Department for Education, 2025) provides information on managing harm between children, including online harm, and the importance of providing ongoing support for all affected children: victims, alleged perpetrators and other children who have been directly or indirectly affected.
If a child is convicted or receives a caution for an offence, risk assessments should be reviewed and updated to ensure relevant protections are in place for all the children affected.
Anyone concerned that a child / young person may be at risk of significant harm due to online activity should make a referral to children’s social care (see Referrals chapter) so that safeguarding procedures can be implemented (see Section 7, Safeguarding Response).
In addition, there are specific referral channels for specific concerns.
Contact the police via 999 (emergency number) where:
Report other non-emergency situations (that is, those that do not require an immediate police response) by dialling 101.
If you are concerned that a child has been a victim of online sexual abuse or you are worried about the way someone has been communicating with a child online, you can report it to NCA-CEOP.
If you see sexual images or videos of someone under 18 online, report it anonymously to the Internet Watch Foundation who can work to remove them from the web and help to identify victims and survivors.
Specific guidance on the steps to take in response to child sexual abuse material generated by AI has been produced by the NCA and partners.
To report other forms of harmful online content (other than online child sexual abuse imagery), see Report Harmful Content. This provides advice and resources on how to report a variety of different issues you may see online including:
It also offers advice on When you Should go to the Police.
Concerns about online radicalisation can be reported to the police on 101 and / or a Prevent referral can be made, so that the victim can get safeguarding support.
Any member of the public can report terrorist content they find online through the gov.uk referral tool – more information about what to report and what happens when you do can be found on the Action Counters Terrorism campaign.
Filtering and age-appropriate parental controls on digital devices can be used to restrict children’s access to age-inappropriate content. Filtering and Monitoring Standards for Schools and Colleges (Department for Education) provides further information.
Internet Matters has step-by-step guides on setting up parental controls to control what content children can access online.
The UK Safer Internet Centre has guidance on how to switch on family-friendly filters to prevent age-inappropriate content being accessed on devices.
The NSPCC has more information for parents or carers with concerns about their child seeking inappropriate or explicit content online.
Apps to help children stay safe online
The BBC has a website and app called Own It, to help children navigate their online lives.
The UKCIS Digital Passport is a resource for care-experienced children and young people and their carers. It is a communication tool created to support children and young people with care experience to talk with their carers about their online lives.
Other useful resources include:
It is also important to ensure that practitioners working with children and young people are aware of the risks posed to children by online activity and how children can be protected and encouraged to help protect themselves. This should include being able to recognise the additional risks that children with special educational needs and disabilities (SEND) face online, for example, from bullying, grooming and radicalisation, to enable practitioners to have the capability to support children with SEND to stay safe online. Agencies should provide suitable training for staff working with children and young people.
Children and young people with SEND can face distinct and heightened online‑safety risks due to differences in communication, social understanding, cognitive processing, emotional regulation and vulnerability to peer influence. These may include misinterpreting online interactions, oversharing personal information, increased susceptibility to grooming or coercion, impulsive posting, difficulty recognising scams, or relying heavily on online spaces for social connection. Some may also miss safety cues because of sensory, visual or hearing needs, or experience power imbalances in specialist settings. Practitioners therefore need to be alert to these additional vulnerabilities and equipped to provide tailored support that helps children with SEND recognise risks, build digital resilience and stay safe online. Agencies must ensure that staff receive suitable training so they can confidently identify these risks and intervene appropriately.
Useful resources include:
Victim blaming is any language or action that implies (whether intentionally or unintentionally) that a person is partially or wholly responsible for abuse that has happened to them. It is harmful and can wrongfully place responsibility, shame or blame onto a victim, making them feel that they are complicit or responsible for the harm they have experienced. For example:
Guidance: Challenging Victim Blaming Language and Behaviours when Dealing with the Online Experiences of Children and Young People helps practitioners to understand that the responsibility always lies with the person who abused the child or young person. The guidance also offers practical steps to help practitioners practice and advocate for an anti-victim blaming approach, in a constructive and supportive way.
One of the greatest barriers to a child or young person seeking help and reporting online abuse, is feeling they are to blame for something that has happened to them. When practitioners working with the child or young person speak or behave in such a way that reinforces this feeling of self-blame, the impact of the abuse the child or young person has already experienced may be greater, leading to a longer recovery. In contrast, positive responses can reduce feelings of post-traumatic stress which a young person may experience as a result of abuse occurring. They can also encourage other children and young people to report their online experiences.
When victim blaming occurs, there is a risk of diminishing the child or young person’s experiences, leading to a lack of, or an inappropriate, safeguarding response. This could be by practitioners initially dealing with an incident or by those involved subsequently. This can have a devastating impact for the child or young person who has experienced abuse and make it less likely that they, or their peers, will have the confidence to disclose abuse in the future. In addition, victim blaming attitudes can prevent families, friends and wider society from recognising certain behaviours as abuse.
Where practitioners have concerns that a child is a victim or perpetrator of online harm, they should discuss with their safeguarding lead. Where it is suspected that the child is at risk of significant harm, a referral should be made to children’s social care and safeguarding processes engaged which may include a multi-agency strategy discussion (see Referrals and Strategy Discussions chapters). Where there is an imminent risk of significant harm, steps must be taken to ensure the child’s immediate safety (see Immediate Protection chapter).
A referral should be made to children’s social care where the child is already known to them, for example, they are currently, or have in the past, been the subject of an early help or child protection plan.
A referral should also be made where there are believed to be wider safeguarding issues such as several children having been affected.
The police should be informed where there is a known or suspected criminal offence. This should take place as soon as possible to enable swift preservation of evidence.
See also Section 4, Who to Contact / How to Make a Report for additional notifications in response to particular types of online harm.
Where the harm involves indecent images, the images should not normally be viewed by practitioners but should be referred to the police. Practitioners may themselves commit a criminal offence by viewing any indecent images. Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) sets out the very limited circumstances where it may be necessary to view images, such as it being unavoidable because a child or young person has presented it directly to a staff member or nudes or semi-nudes have been found on an education setting’s device or network. Practitioners must never copy, print, share, store or save indecent images – this is illegal. If any devices need to be taken and passed onto the police, the device/s should be confiscated, and the police should be called. The device should be disconnected from Wi-Fi and data and turned off immediately to avoid imagery being removed from the device remotely through a cloud storage service. The device should be placed in a secure place, for example in a locked cupboard or safe until the police are able to come and collect it.
Viewing indecent images can be distressing for both children, young people, and adults and appropriate emotional support may be required.
Schools / colleges becoming aware of incidents involving nude / semi-nude images of children should hold an initial review meeting to establish:
An immediate referral to police and / or children’s social care should be made if at the initial stage:
Guidance – Sharing Nudes and Semi-Nudes: Advice for Education Settings Working with Children and Young People (gov.uk) sets out the very limited circumstances where an education setting may decide to respond to an incident involving sharing of nude / semi-nude images between children without involving the police or children’s social care. They can still choose to escalate the incident at any time if further information / concerns are disclosed later.
The decision to respond to the incident without involving the police or children’s social care should only be made in cases where the designated safeguarding lead (or equivalent) is confident that they have enough information to assess the risks to any child or young person involved and the risks can be managed within the education setting’s pastoral support and disciplinary framework and, if appropriate, their local network of support. The reasons for not referring the incident should be recorded.
All incidents relating to nudes and semi-nudes being shared need to be recorded by education settings. This includes incidents that have been referred to external agencies and those that have not.
Many instances of online harm will involve possible criminal offences and so will necessitate a police response and safeguarding response. Educational establishments are often likely to be involved as guidance tell us that many of these events are likely to involve the child’s educational experience in some way, such as images of children being widely circulated between pupils.
Children accessing alternative educational settings, voluntary activities and specialist units should be considered with the context of this policy.
Multi-agency information sharing is important to enable effective assessment of risk and identification of other children who may be affected.
See also Tier 1 – Children Safeguarding Data Sharing Agreement (DSA) and Data Protection.
RELATED GUIDANCE
Guidance: Learning Disability – Applying All Our Health (gov.uk)
CONTENTS
A learning disability is defined by the Department of Health and Social Care (DHSC) as:
a significantly reduced ability to understand new or complex information, to learn new skills (impaired intelligence), with a reduced ability to cope independently (impaired social functioning), which started before adulthood.
A learning disability is different for everyone. The degree of disability can vary greatly, and learning disabilities can be classified as mild, moderate, severe or profound. In all cases, a learning disability is a lifelong condition and cannot be cured. People who are known to learning disability services are likely to be those with a more significant learning disability.
A learning disability is not a physical disability. It is caused by something which affects the development of the brain either before birth, during birth or in early childhood.
There are a number of conditions and neurological disorders that often involve or cause some type of learning disability, including Down’s syndrome, autism, meningitis, epilepsy or cerebral palsy.
Possible causes of learning disabilities include:
Sometimes the cause of a learning disability remains unknown.
A particular level of IQ cannot be taken as the only defining characteristic of learning disability, and people can have different ability levels across the different components of IQ and other tests. Sometimes it can be difficult to clearly distinguish between those parents who have learning disabilities and those who do not. In the context of parenting, it may be more helpful for practitioners to focus on identifying support needs associated with the impact of the parent’s learning disability, rather than focusing on the definition of learning disability.
A learning disability is different to a learning difficulty, which is a reduced intellectual ability for a specific form of learning and includes conditions such as dyslexia (reading), dyspraxia (affecting physical co-ordination) and attention deficit hyperactivity disorder (ADHD). A person with a learning disability may also have one or more learning difficulties. However, some people who have the label ‘learning disability’ prefer to be called ‘people with learning difficulties’. Practitioners should be sensitive to how people define and describe themselves and use language that parents are comfortable with in their contact with them.
Often those parents with learning disabilities who are in contact with social care services experience a range of difficulties. They may have particularly high levels of need, and present as complex cases where it can be difficult to disentangle the competing concerns.
Compared to people without a learning disability, people with a learning disability tend to experience poorer physical and mental health and reduced life expectancy. They are also:
Parents with learning disabilities may experience a range of needs and difficulties, including a physical or sensory impairment and / or long-term health condition, mental health problems or substance misuse problems and experience domestic abuse.
Some parents with learning disabilities experience significant housing problems, including homelessness, harassment from neighbours and difficulties in maintaining a tenancy.
The same principles of safeguarding and promoting the welfare of children should be applied to the children of parents with learning disabilities as to the children of non-learning disabled parents. However, working with and assessing parents with learning disabilities often requires a specialised response such as different approaches to communication and assessment.
Lack of a formal diagnosis of learning disability may affect a parent’s eligibility for some services, but a parent who presents as having difficulty with, or being unable to, read, write, budget, deal with numbers or abstract concepts, process information, retain and apply it etc. will almost certainly require support to enable them to raise their children safely and well. This is likely to mean allowing more time for a parent with a learning disability to understand what is happening and appropriate and effective communication so they can participate fully in the process.
Effective joint working across all involved agencies is essential, in particular between adult and children’s services where they are supporting parents and children respectively.
Young parents and parents-to-be with learning disabilities may be in transition between children’s and adult services.
Good Practice Guidance on Working with Parents with a Learning Disability (Working Together with Parents Network) identifies five key features of good practice in working with parents with learning disabilities:
Accessible information and communication are crucial to enabling parents with learning disabilities to engage with services and therefore to maximise the chances of children’s needs being met.
Parents should be provided with assistance to enable them to understand what is happening and to express their views. Information may well need to be provided more than once in order for parents to understand what is going on.
Information should be provided in a format which is accessible to them, for example:
Where a child protection plan is drawn up and this involves action to be taken by parents, parents should be fully supported to understand what is required of them and what support is available to help achieve this.
Effective, two-way communication is particularly important in meetings involving a number of different professionals (such as child protection conferences). Information and communication must be accessible, jargon should be avoided and parents should have someone to support them to prepare for the meeting and take part in it, if this is what they want.
Concerns about the ability of parents with learning disabilities to adequately care for and protect their children may arise during antenatal and postnatal care.
Identification of needs should start when a pregnancy is confirmed, with early, appropriately tailored assessments carried out to identify the support which will be needed to look after a new baby. Recognising and addressing support needs at the earliest stages of the parenting experience may help to prevent difficulties for parents which undermine children’s welfare.
Adult learning disability services should take steps to ensure that people with learning disabilities who become parents know about the support available. Such services are well-placed to provide new parents and parents-to-be with accessible information about both universal and specialist services. Children’s social care should also take steps to ensure that adults with learning disabilities who become parents know about the support available to help them with their responsibilities as parents.
It is good practice that, as a general rule, referrals relating to the needs of parents with learning disabilities should be directed to learning disability services. Where there are concerns about children’s welfare a referral should also be made to children’s social care (see Referrals chapter). If a referral is made directly to children’s services, and it then becomes apparent that a parent has a learning disability, a referral should then also be made to adult learning disability services.
Good practice is promoted where there is clear agreement between adult and children’s social care as to the circumstances in which single or joint assessments are required and who should take the lead.
For example:
Assessments involving families affected by parental learning disability should always include specialist input concerning the impact of learning disability. Where there are other difficulties such as mental health and/or physical health problems, domestic abuse or substance misuse, assessments should also include, where appropriate, specialist input on these issues. Assessments should also address the possible vulnerability of the learning disabled parent and their own need to be protected from harm. Parents should be given information – in a format suitable to them – about why an assessment is being carried out, what it will involve, and what might happen as a result.
Parents should be invited to attend child protection conferences and support provided to enable them to participate fully. Careful consideration should be given to ensuring that all communication associated with the child protection conference – from invitation and the conduct of the meeting through to the minutes / notes of the meeting – is accessible to the parent with learning disabilities. Information should be sought, from the parent and / or their advocate, about what communication format is accessible to them.
Good practice will be promoted by:
Key issues for parents with learning disabilities involved in pre-proceedings and court proceedings are their needs for accessible information, support of an independent advocate, enough time to understand what is going on, to be fully involved in any assessments and care planning, and to have the chance to learn and demonstrate improved parenting capacity.
Parents whose children are the subject of section 47 enquiries should always be given early information about independent sources of advice and advocacy. Where possible, independent advocates should have the necessary skills and expertise concerning both learning disability and child protection.
Where section 47 enquiries conclude that a child is not at risk, or not at continuing risk, of significant harm, it will be important that, where appropriate, action is taken – under section 17 of the Children Act 1989 – to prevent future problems arising. It is particularly important to avoid the situation where poor standards of parental care, which do not meet the threshold of significant harm to a child, subsequently deteriorate because of a lack of support provided to the parent. It is also important to provide any necessary support when a child is no longer the subject of a child protection plan, in order to prevent a subsequent deterioration in parental care.
Families affected by parental learning disability are likely to have an ongoing need for support, and where a child protection plan is not considered necessary, another appropriate pathway should be considered.
Some parents with learning disabilities will only need short-term support, such as help with looking after a new baby or learning about child development and childcare tasks. Others, however, will need ongoing support. Most may need support at various points of their family’s life cycle. However, case-law has established that the level of support needed to ensure ‘good enough parenting’ should not be so great as to amount to ‘substitute parenting’.
CONTENTS
Unlike female genital mutilation, male circumcision is not an illegal act in itself and is not normally a child protection or safeguarding issue. This procedure provides practitioners in Buckinghamshire with an understanding of when male circumcision may raise safeguarding children concerns and how to respond if such concerns arise.
Male circumcision is the surgical removal of the foreskin on the penis. The procedure is usually requested for social, cultural or religious reasons (e.g. by families who practise Judaism or Islam). Additionally, there are parents who request circumcision for assumed medical benefits.
There is no requirement in law for professionals undertaking male circumcision to be medically trained or to have proven expertise. Traditionally, religious leaders or respected elders may conduct this practice.
Male circumcision is a non-reversible procedure.
It is rare for circumcision to be recommended for medical reasons in boys. This is because other less invasive and less risky treatments are usually available. See Circumcision in Boys (NHS). Doctors should be aware of this and reassure parents accordingly.
The medical harms or benefits of circumcision have not been unequivocally proven, except to the extent that there are clear risks of harm if the procedure is done inexpertly.
Doctors/health professionals should ensure that any parents seeking circumcision for their son in the belief that is confers health benefits are fully informed that there is a lack of professional consensus as to current evidence demonstrating any benefits. The risks/benefits to the child must be fully explained to the parents and to the child himself, if Gillick competent.
Where parents request circumcision for their son for assumed medical reasons, it is recommended that circumcision should be performed by or under the supervision of doctors trained in children’s surgery in premises suitable for surgical procedures.
Male circumcision that is performed for any reason other than physical clinical need is termed ‘non-therapeutic male circumcision’ or NTMC.
See also Section 7, Non-therapeutic Male Circumcision – Principles for Good Practice.
Practitioners may assume that the circumcision procedure (therapeutic or non-therapeutic) is lawful provided that:
If doctors or other professionals are in any doubt about the legality of their actions, they should seek legal advice.
Consent for circumcision is valid only where the people (or person) giving consent have the authority to do so and understand the risks and implications, including that it is a non-reversible procedure.
The British Medical Association (BMA) and General Medical Council (GMC) recommend that consent should be sought from both parents having parental responsibility. Non-therapeutic male circumcision has been described by the courts as an ‘important and irreversible’ decision that should not be taken against the wishes of a parent. It follows that where a child has two parents with parental responsibility, doctors considering circumcising a child must satisfy themselves that both have the necessary parental authority and have given valid consent. Where people with parental responsibility for a child disagree about whether the child should be circumcised, the child should not be circumcised without the leave of a court.
An assessment of best interests in relation to non-therapeutic male circumcision should include consideration of:
Doctors are under no obligation to comply with a request to circumcise a child and circumcision is not a service which is provided free of charge. Nevertheless, some doctors and hospitals are willing to provide circumcision without charge, rather than risk the procedure being carried out in unhygienic conditions.
Poorly performed circumcisions have legal implications for the doctor responsible. In responding to requests to perform male circumcision, doctors should follow the guidance issued by professional organisations:
Circumcision may constitute significant harm to a child if the procedure was carried out in such a way that :
Significant harm is defined in Section 31 Children Act 1989 and is referred to in accordance with the statutory guidance Working Together to Safeguard Children. Where it is believed that a child has suffered, or is likely to suffer, significant harm, concerns should be shared with Children’s Social Care as a referral (see Referrals).
Harm may stem from clinical practice being incompetent (including lack of anaesthesia) and/or clinical equipment and facilities being inadequate, not hygienic, etc. The professionals most likely to become aware that a boy is at risk of, or has already suffered from, harm from circumcision are health professionals (GPs, health visitors, A&E staff or school nurses), and childminding, day care and teaching staff. Others with responsibilities or roles within the wider community may also become aware, e.g. members of faith groups or sports/voluntary groups.
If anyone becomes aware, through something a child discloses, or another means, that the child has been, or may be, harmed through male circumcision, a referral must be made to children’s social care.
Children’s social care should assess the degree of harm and determine whether the likely or actual harm is significant for the child in question. Possible risks for other children in the family (including unborn babies) should also be considered
Where a criminal offence is suspected, e.g. sexual abuse or unjustified deliberate injury, the police must also be notified.
If any professional considers that their concerns are not being responded to appropriately, the Escalation, Challenge and Conflict Resolution Procedure should be followed.
If concerns relate to a professional or other person in a position of trust, concerns must be discussed with the Local Authority Designated Officer (LADO).
Community and religious leaders should take a lead in the absence of approved professionals and develop safeguards in practice. This could include setting standards around hygiene, advocating and promoting the practice in a medically controlled environment and outlining best practice if complications arise during the procedures.
CONTENTS
Child exploitation, whether sexual or criminal, is child abuse. Children who are exploited face significant harm to their physical, emotional and psychological health and well-being. The effects of trauma experienced through exploitation can be cumulative and can require continued ongoing support to recover from throughout the child’s lifetime and into their adult years. This harm often extends to the wider family and it is important that parents/carers are offered support also.
Agencies across Buckinghamshire are committed to safeguarding children and young people from being sexually and / or criminally exploited, and children are recognised as victims of abuse.
This protocol aligns with local arrangements to safeguard children and sets out a clear pathway by which to ensure all organisations work together to provide the best service possible for children and young people either at risk or exploitation or who have experienced exploitation in Buckinghamshire.
An overarching term of child exploitation will be used throughout this protocol to encompass both criminal and sexual exploitation of children.
This protocol is to support professionals to understand how to access support for children where there are concerns regarding exploitation. This is applicable to external professionals and local authority staff.
It is often the case that children do not perceive themselves to be victims, as they consider they have acted voluntarily or that the exploiter is their friend. Peer on Peer exploitation is commonplace and often unrecognised as exploitation by the victim. The reality is that their behaviour is not voluntary or consenting, and every child in this situation needs to be considered a victim first. The response needs to focus on disruption and engagement.
The nationally agreed definitions for sexual exploitation and criminal exploitation are used across Buckinghamshire:
Child sexual exploitation is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity:
(a) in exchange for something the victim needs or wants, and/or
(b) for the financial advantage or increased status of the perpetrator or facilitator.
The victim may have been sexually exploited even if the sexual activity appears consensual. Child sexual exploitation does not always involve physical contact; it can also occur through the use of technology (taken from Child sexual exploitation: definition and guide for practitioners, Department for Education).
Child criminal exploitation occurs where an individual or group takes advantage of a person under the age of 18 and may coerce, manipulate or deceive a child or young person under that age into any activity.
(a) in exchange for something the victim needs or wants, and/or
(b) for the financial advantage or increased status of the perpetrator or facilitator, and/or
(c) through violence or the threat of violence.
The victim may be exploited even if the activity appears consensual (i.e. moving drugs or the proceeds of drugs from one place to another). Additionally, child criminal exploitation does not always involve physical contact; it can also occur through the use of technology (taken from Serious Violence Strategy, Home Office).
Buckinghamshire Council and partners have committed resources from their agencies to ensure a collective approach is adopted across the county when managing child exploitation.
There is a clear link between children who are missing and exploited;
Children who run away are at significant risk of harm (Hanson & Holmes, 2014). Children who are missing from care, home or education are at greater vulnerability of exploitation (Pona, 2016; Brandon et al. 2020).
For guidance relation to local authority processes please see “ Missing Children Practice Guidance “.
Multi agency practitioners should refer to Children Missing from Care, Home and Education.
The Missing and Exploitation Hub will have varying degrees of involvement in a child(ren)’s case, the rationale for which will be clearly noted on the child’s social care record. All relevant agencies will be made aware of the decision and rationale for the involvement of and specific role the Hub will carry out. The majority of these decisions will be discussed collaboratively within the Multi-Agency Child Exploitation Meeting (MACE).
The Missing and Exploitation Hub is made up of;
Partners work together to;
If you have concerns regarding the exploitation of a child, the following process should to be followed:
If you are unsure if a child is known to Social Care or not, please contact the MASH who will either advise you to complete a referral and CE tool or refer you to the relevant team.
The referral will be screened at the Hub weekly touchdown screening meeting. The referrer may be asked to provide further information if required. This meeting is multi-agency and will determine if threshold is met for discussion in the Multi-Agency Child Exploitation Meeting (MACE).
If threshold is met, the child will then be added to the next Multi-Agency Child Exploitation Meeting (MACE) agenda. MACE meetings are held weekly.
The Hub will contact you and agree any immediate actions that may need to be considered to support the child / family.
The child will then be discussed at MACE where a Multi-Agency Risk Assessment and Plan (Appendix 2) will be considered. This will form part of any statutory plan and does not replace it.
Child Exploitation takes place across local communities and information and intelligence known to statutory and voluntary sector agencies should be used to highlight the threat, establish and reduce risk. An improved picture of intelligence will enable effective action in a greater number of cases of child exploitation, thereby reducing the harm that would otherwise be caused to the young victims and their families.
The MACE meeting provides the framework to allow regular information sharing and action planning to tackle child exploitation across Buckinghamshire.
MACE meetings are co-chaired by Thames Valley Police and the Local Authority and are attended by all relevant partner agencies. Additional representation from other agencies including CAMHS and drug and alcohol services also attend where required.
It is the statutory duty of the local authority to complete a referral to National Referral Mechanism (NRM) for children where it is believed they are the victim of modern-day slavery. For children, this often relates to their trafficking for the purpose of criminal and/or sexual exploitation. The NRM is a framework for identifying and referring potential victims and ensuring they receive the appropriate support. The mechanism supports both children and adults.
It is important to note that children under the age of 18 do not have to consent to being referred to the NRM, and must be first safeguarded and then referred into the NRM process. All children where there is a concern of exploitation should be referred into the NRM.
A referral form is completed online. The Missing and Exploitation Hub will complete an NRM referral form in collaboration with the professional who is working with the child. This is important as the detailed information and knowledge of the issues will be best known to the professional who is working with the child, but the oversight and tracking of referrals sits with the Missing and Exploitation Hub. For more guidance, please see the Home Office website.
Appendix 1 – Child Exploitation Screening Tool (opens in Word)
Appendix 2 – Multi Agency Risk Assessment and Plan (opens in Word)
Appendix 3 – Categories of Risk – Emerging, Significant, Experiencing (opens as a PDF)
Appendix 4 – Appropriate Language in Relation to Child Exploitation (The Children’s Society)
Appendix 5 – Contextualised Safeguarding Staff Guide (opens in Word)
RELEVANT GUIDANCE
Statutory Guidance: Multi Agency Public Protection Arrangements (MAPPA) (Ministry of Justice)
Guidance: Probation Service Management of MAPPA Level 1 Cases Policy Framework (gov.uk)
CONTENTS
Multi-Agency Public Protection Arrangements (MAPPA) was introduced in 2001 as the statutory arrangements for managing sexual and violent offenders. It is a process through which the police, probation and prison services work together, with other agencies, to help reduce the re-offending behaviour of violent and sexual offenders living in the community, in order to protect the public.
The purpose of MAPPA is to ensure that comprehensive risk assessments are undertaken and robust risk-management plans put in place. MAPPA takes advantage of coordinated information-sharing across the agencies on each MAPPA offender, and ensures that appropriate resources are directed in a way which enhances public protection.
MAPPA is not a statutory body in itself but is a mechanism through which agencies can better discharge their statutory responsibilities and protect the public in a coordinated way.
The Responsible Authority is the primary agency for MAPPA. This is the police, prison and probation service in each area, working together. The Responsible Authority has a duty to ensure that the risks posed by specified sexual and violent offenders are assessed and managed appropriately.
Other bodies have a duty to cooperate with the Responsible Authority in this task. These duty to cooperate agencies (DTC agencies) will need to work with the Responsible Authority on particular aspects of an offender’s life, for example education, employment, housing, social care. These agencies include:
The first stages of the process are to identify offenders who may be liable to management under MAPPA as a consequence of their caution or conviction and sentence. This responsibility falls to the agency that has the leading statutory responsibility for each offender. Offenders are placed into one of four MAPPA categories according to their offence and sentence:
MAPPA offenders are managed at one of three levels according to the extent of agency involvement needed and the number of different agencies involved.
Level 1: ordinary agency management – ordinary agency management level 1 is where the risks posed by the offender can be managed by the agency responsible for the supervision or case management of the offender. The majority of offenders are managed at level 1. This involves the sharing of information but does not require multi-agency meetings.
Level 2: active multi-agency management – cases should be managed at level 2 where the offender:
Level 3: active enhanced multi-agency management – level 3 management should be used for cases that meet the criteria for level 2 but where it is determined that the management issues require senior representation from the Responsible Authority and DTC agencies. This may be when there is a perceived need to commit significant resources at short notice or where, although not assessed as high or very high risk of serious harm, there is a high likelihood of media scrutiny or public interest in the management of the case and there is a need to ensure that public confidence in the criminal justice system is maintained.
The vast majority of MAPPA offenders will be managed through the ordinary management of one agency, although this will usually involve the sharing of information with other relevant agencies.
The structural basis for the discussion of MAPPA offenders who need active interagency management, including their risk assessment and risk management, is the MAPP meeting.
The Responsible Authority agencies and the MAPPA Coordinator are permanent members of these meetings. The DTC agencies should be invited to attend for any offender in respect of whom they can provide additional support and management. The frequency of meetings depends on the level of management deemed appropriate for each offender.
RELEVANT CHAPTER
CONTENTS
A Multi-Agency Risk Assessment Conference (MARAC) is a local, multi-agency victim focused meeting where professionals meet to share information on high risk cases of domestic abuse.
Information about the risks faced by those victims, the actions needed to ensure safety, and the resources available locally are discussed, and used to create a risk management plan involving all agencies. The MARAC is part of a coordinated response to domestic abuse, incorporating representatives from statutory, community and voluntary agencies working with victims, adults experiencing or at risk of abuse or neglect, children and alleged perpetrators.
The MARAC aims to:
Multi-Agency Public Protection Arrangements (MAPPA) may also need to be considered in relation to an offender (see Multi-Agency Public Protection Arrangements chapter).
The MARAC consists of a core group of professionals, representing the statutory and voluntary sectors. The meeting involves contribution and commitment from agencies including police, probation, children’s social care, adult social care (mental health, safeguarding adults), health, education, housing, substance misuse services, and specialist domestic abuse services. Other agencies can attend as required, when they have involvement in a case which is being discussed.
The victim does not attend the meeting, nor the perpetrator or Crown Prosecution Service.
Each victim referred to the MARAC will be allocated an Independent Domestic Violence Adviser (IDVA). The IDVA is a trained specialist whose goal is the safety of domestic abuse victims, focusing on victims at high risk of harm.
The IDVA will attempt to make contact with the referrer and the victim following receipt of a MARAC referral. The IDVA’s job is to be a bridge between victims and the MARAC meeting. The IDVA will try and meet the victim beforehand, or at least talk to them on the phone, and explain how the meeting works, what it can do, and what the options are.
The IDVA will also ask if there is anything the victim would want to be discussed at the meeting.
Referrals can be made (and are encouraged) by any agency who identifies a victim of domestic abuse as being high risk. A DASH Risk Identification Checklist (see Section 5, DASH Checklist) will enable a practitioner to determine the level of risk posed to a victim. Upon meeting the MARAC threshold for high risk, the local MARAC coordinator / administrator should be contacted regarding making a referral. The case will be submitted for the next available MARAC; however in some circumstances, an emergency MARAC meeting may be called.
See Resources for Identifying the Risk Victims Face, DASH Checklist (SafeLives)
The DASH Checklist is for all professionals working with victims of domestic abuse, stalking and honour based abuse.
If a practitioner identifies an individual they are or have been working with, is a victim of domestic abuse, they should complete the tool with the individual, where possible.
The DASH checklist will gather relevant information about the person’s circumstances in order to assess the risk posed to them.
DASH gives a consistent and practical tool to practitioners working with victims of domestic abuse to help them identify those who are at high risk of harm.
It should be noted, however, training is crucial to understanding the DASH Risk Model and it is therefore recommended all staff have training prior to completing the checklist in practice.
Neglect Strategy (2026 – 2028) opens as a PDF, in a new window.
RELEVANT INFORMATION
Prevent Duty Guidance (Home Office)
Prevent Duty Training (Home Office)
Channel duty guidance: protecting people susceptible to radicalisation (Home Office)
CONTENTS
Radicalisation is the process through which people come to hold increasingly extreme views or beliefs that support terrorist groups or activities. The most common types of terrorism in the UK are extreme right-wing terrorism and Islamist terrorism. Multi-agency working is key to supporting children who have been radicalised, or who are at risk of radicalisation.
Extremism is defined as the promotion or advancement of an ideology or beliefs based on violence, hatred or intolerance that aims to:
(See Definition of Extremism, gov.uk).
The Prevent Strategy defines extremism as ‘the vocal or active opposition to fundamental British values, including democracy, the rule of law, individual liberty and mutual respect and tolerance of different faiths and beliefs. It also includes calls for the death of members of the armed forces’.
Exposure to extremism can lead to radicalisation and acts of terrorism.
The national counter-terrorism strategy, CONTEST aims to reduce risks of terrorism in the UK and overseas.
Prevent is one of the key parts of CONTEST and aims to stop people becoming terrorists or supporting terrorism; it focuses on early intervention and safeguarding. Prevent is run locally by specialist staff who understand the risks and issues in the local area and know how best to support their communities. Through working together, organisations can identify people who are at risk of radicalisation and provide them with support. The objectives of Prevent are to:
The Prevent duty (Section 26, Counter-Terrorism and Security Act 2015 (CTSA) requires frontline staff working in specific organisations – including education, health, local authorities, police, prisons and probation – to work together to help prevent the risk of people becoming terrorists or supporting terrorism. It helps to make sure that people who are being radicalised are supported in the same way as they are under safeguarding processes.
Children and young people can be exposed to the messages of extremist groups or drawn into violence in different ways, including through family members, by direct contact with extremist groups or, most often, the internet.
Everyone is different and there is no single way of identifying who is at risk of being radicalised into terrorism or supporting terrorism. Signs that a child or young person is being radicalised include them:
Any child can be radicalised but there are some factors which may make a young person more vulnerable. These include them:
These factors will not always lead to radicalisation.
Children are exposed to news and information in lots of different ways and and they may see things which worry them or make them angry. Professionals and parents and carers can help them understand world events and issues in the news by:
Children should be encouraged to consider other viewpoints and to check the facts behind the information that they are looking at. Radicalisers will use conspiracy theories and fake news to draw people in.
As most radicalisation takes place on-line, make sure that devices have the appropriate parental controls in place, and monitor screen time.
Staff working in frontline roles such as education will often be the first to notice if a child displays concerning behaviour. If staff notice behaviours that are a cause for concern, they should consider whether the child is at risk of radicalisation.
There could be many different reasons for the behaviours, not just radicalisation. It is important to understand the context and try to find out why these changes are happening, before reaching conclusions too quickly.
Concerns about radicalisation or extremism should then be checked / shared with the designated safeguarding lead in the organisation. The Prevent lead in the local authority or local police can also be contacted for advice.
Before deciding whether to make a referral to Prevent, it is important to gather as much information as possible, to assess if the child or young person may be on a pathway that could lead to terrorism.
The Department for Education has a dedicated telephone helpline for schools in England who have non-emergency concerns about extremism; which can be contacted by telephoning: 020 7340 7264.
Where there are concerns about radicalisation and extremism, relevant information should be shared with children’s social care (see Referrals chapter). A multi-agency meeting will be held to discuss whether to make a referral to the police for support under Prevent. Referrals to Prevent are made using the Prevent national referral form (see Get help for radicalisation concerns , gov.uk).
Children who could be referred include those who:
REMEMBER – in an emergency, always ring 999.
Once a referral is submitted to the local Prevent team, specialist police staff will assess it. Firstly, they will check if the child is an immediate security threat. The police will then check if there is a risk of radicalisation which means that the child should be discussed at the local Channel panel to see if they are eligible for support through Prevent. This is called a ‘gateway assessment’. Referrals into Channel are made by the Police. If the child needs other support, this should continue unless there is a good reason not to do so.
Channel panels are chaired by the local authority, and attended by multi-agency partners such as police, education professionals, health services, education and children’s social care. They meet to discuss the referral, assess the risk, and, if appropriate, agree a package of support specific to the individual child. Channel is a voluntary process, and the child’s parents and carers must give their consent before a child receives support.
The type of activities that are included in a support package will depend on risk factors, vulnerabilities, and local resources, but might include:
family support contact – activities aimed at supporting family and personal relationships, including formal parenting programmes;
Where Channel is not considered suitable for the child, or their parents or carers do not consent, alternative options will be explored. If the risks cannot be managed in Channel, they will be kept under review by the police.
Where the Channel panel decides to close a case, the child and their parents and carers should be told that their case is being closed and that they will no longer receive support through Channel. They should also be told that ongoing support they are receiving through mainstream services (such as from the NHS, children’s social care, youth justice services, education) will continue.
Identifying a lead professional at the point of the case being closed provides reassurance that they can be brought back for discussion at the panel quickly, should concerns about them re-emerge.
The panel is best placed to identify which agencies will continue to engage with the child after their case with Channel has been closed and to identify a lead professional. Frontline practitioners involved in providing continuing support must be informed that Channel no longer has oversight of the child, and advised on how to re-refer them to Prevent if there are any future concerns.
When sharing personal data about children and young people at risk of radicalisation, it is important to adhere to the requirements of data protection legislation.
Data protection legislation is not intended to prevent the sharing of personal data, but to make sure that it is done lawfully and with appropriate safeguards in place. Under the Data Protection Act and UK GDPR, there must be a legal basis to share personal data. The Prevent Duty is a lawful basis on which to share data.
See also Data Protection and Tier 1 – Children Safeguarding Data Sharing Agreement (DSA)
RELATED GUIDANCE
Self-harm (Quality Standard QS 34, NICE) – covers the initial management of self-harm and the provision of longer-term support for children and young people (aged 8 to 18).
Self-harm: Assessment, Management and Preventing Recurrence Guideline NG 225, NICE) – covers assessment, management and preventing recurrence for children, young people and adults who have self-harmed. It includes those with a mental health problem, neurodevelopmental disorder or learning disability and applies to all sectors that work with people who have self-harmed.
Suicide Prevention: Resources and Guidance (Office for Health Improvement and Disparities) – help for local authorities, public healthcare professionals, police forces and others to prevent suicides in their areas
Self-Harm for Parents and Carers (Royal College of Psychiatrists)
CONTENTS
Self-harm is a term used when someone injures or harms themselves on purpose rather than by accident. Common examples include ‘overdosing’ (self-poisoning), hitting, cutting or burning oneself, pulling hair or picking skin, or self-strangulation (Royal College of Psychiatrists).
Some of the reasons children may self-harm include:
Sometimes the reason is unknown. The reasons can also change over time and will not be the same for each child or young person.
Suicide is when a child ends their own life. There is no single reason why a child dies by suicide; social, psychological and cultural factors can contribute to a child or young person being at greater risk of suicide.
Research by the Health Quality Improvement Partnership (HQIP) found that over half of young people who die by suicide have a history of self-harm and that, although there are many antecedents of suicide in young people, self-harm is a crucial indicator of risk and should always be taken seriously, even if the physical harm is minor.
Common themes in suicide by children and young people include:
Suicide-related internet / social media platform use is defined by the HQIP as:
Internet safety is an important component of suicide prevention in young people, particularly in the under-20s (see also Internet Safety / Online Safety chapter).
Principles for initial assessment and care by healthcare professionals and social care practitioners
When a health care or social care practitioner becomes aware of a child following an episode of self-harm, they should:
When a child who has self-harmed presents to a non-health professional, for example, a teacher or a member of staff in the criminal justice system, the non-health professional should:
The non-health professional should establish the following as soon as possible:
In line with the NICE Self-harm Quality Standard, children who have self‑harmed will have an initial assessment of their physical health, mental state, safeguarding concerns, social circumstances and immediate concerns about their safety, and receive a psychosocial assessment. A mental health professional experienced in assessing children and young people who self-harm should carry out the psychosocial assessment. They should ask about:
Children and young people who have been admitted to a paediatric ward following an episode of self-harm should have:
Following referral to children’s social care, a multi-agency safeguarding response will include assessment of the child’s situation and whether the child is in need of services under section 17 Children Act 1989 or whether the child is suffering or likely to suffer significant harm, and child protection enquiries should be made under section 47 Children Act 1989 (see Section 47 Enquiries chapter). Social care practitioners should foster a collaborative approach with all agencies involved in the child’s care, as well as their family members and carers as appropriate.
Assessment may be needed of the child’s mental capacity to give informed consent to medical interventions, which depends on their age. Where the child is aged 16 or over, capacity is assessed in line with the principles of the Mental Capacity Act 2005 (MCA). A child is considered unable to make a decision if they cannot:
Where the child is under the age of 16, the MCA does not apply and an assessment is based on whether they are ‘Gillick competent’. Where a child is assessed as being Gillick competent to make the particular decision or give the particular consent at the relevant time, they are able to give a valid consent or make a valid decision without the requirement for additional consent by a person with parental responsibility.
There is no set of defined questions to assess Gillick competency. Practitioners need to consider several things when assessing a child’s capacity to consent, including:
Note that capacity can fluctuate, particularly if the child is in a state of emotional distress,
For further information see Mental Capacity and Consent chapter.
A multi-agency approach is important to gain a rounded understanding of the child’s situation. The statutory guidance Working Together to Safeguard Children is clear that no single practitioner can have a full picture of a child’s needs and circumstances, so effective sharing of information between practitioners, local organisations and agencies is essential for early identification of need, assessment, and service provision to keep children safe. Practitioners should be proactive in sharing information as early as possible to help identify, assess, and respond to risks or concerns about the safety and welfare of children.
Whilst it is good practice to be transparent and inform children and their parents / carers that information will be shared for these purposes, it is not necessary to seek consent to share information for the lawful purpose of safeguarding and promoting the welfare of a child.
For further information see the Tier 1 – Children Safeguarding Data Sharing Agreement (DSA) and Data Protection chapter.
RELEVANT CHAPTER
Multi Agency Child Exploitation Protocol
RELEVANT INFORMATION
Brook – the young people’s sexual health and well-being charity
Relationships and sex education (RSE) and health education (Department for Education)
Harmful sexual behaviour among children and young people (NICE)
CONTENTS
Instances of underage sexual activity may raise difficult issues for practitioners and need to be handled with sensitivity. Agencies should ensure that all children and young people are given appropriate protection from sexual abuse. It is the responsibility of all professionals to accurately assess any risk of harm, including significant harm, when a child or young person is engaged in sexual activity. This is likely to require a multi-agency approach.
This guidance has also been formed within the context of government policy and therefore supports the principle that young people should be able to access sexual and reproductive health services, including advice about contraception and abortion.
This guidance applies to all sexual relationships. It is designed to assist staff in identifying where sexual relationships may be abusive and whether a child or young person may need the provision of protection or additional services in relation to sexual activity.
Where there are indications of actual or risk of sexual abuse of a child/young person, be it child sexual exploitation, interfamilial abuse or peer-on-peer abuse, also see the Multi Agency Child Exploitation Protocol.
The sexual behaviour of young people is conceptualised as laying on a continuum from mutual exploration to behaviours that are seriously harmful to them or to other children or young people.
 Where sexual behaviour is harmful, please refer to the Harmful Sexual Behaviour chapter.
Where sexual behaviour is harmful, please refer to the Harmful Sexual Behaviour chapter.
It is essential for agencies to clarify the age of the young person, as this will dictate the course of action to be taken. The Sexual Offences Act 2003 sets out the law in relation to children and young people under the age of 18 years old:
A child under 13 is not legally capable of consenting to sexual activity. Any offence under the Sexual Offences Act 2003 involving a child under 13 is very serious and offences committed by an adult may result in a significant prison sentence.
Where a professional is concerned that a child under 13 is involved in penetrative sex, or other intimate sexual activity, there will always be reasonable cause to suspect that a child, whether a girl or boy, is suffering or is likely to suffer significant harm. Professionals should make a referral to Children’s Social Care (see Referrals chapter).
Children’s Social Care will convene a strategy meeting which should include the professional making the referral as well as representatives from Children’s Social Care, police and other relevant agencies.
Where both parties involved in sexual activity are under 13, then both children should be considered at risk of significant harm. Thames Valley Police will seek to avoid any prosecution of a child where the children are age appropriate and there is no evidence of coercion, threat, force or other power imbalance.
Sexual activity with a child under 16 is also a criminal offence. Where it is consensual it may carry a less serious criminal penalty than under 13 but still attracts a significant prison sentence. It may nevertheless have serious consequences for the welfare of the child.
Consent is always based on choice and is active, not passive. Consent is possible only when there is equal power. Forcing someone to give in is not consent, and going along with something because of wanting to fit in with a group is not consent: ‘If you can’t say “no” comfortably then “yes” has no meaning. If you are unwilling to accept “no” then “yes” has no meaning.’
Consideration should be given in every case of sexual activity involving a child aged 13–15 as to whether there should be a discussion with other agencies and whether a referral should be made to Children’s Social Care. Professionals should use the risk indicators outlined in Section 4 to inform their decision making.
Cases of concern should be discussed with the nominated child protection lead for the agency and subsequently with other agencies if required. Where confidentiality needs to be preserved, the initial consultation can occur without identifying the child directly or indirectly.
Where there is reasonable cause to suspect that significant harm to a child has/might occur, a referral must be made to Children’s Social Care and a strategy discussion held.
Thames Valley Police will seek to avoid any prosecution of a child where the children are age appropriate and there is no evidence of coercion, threat, force or other power imbalance.
Although in most cases sexual activity in itself is not an offence when the young person is over the age of 16, young people aged 16 and 17 are still vulnerable to harm through an abusive sexual relationship and are still offered the protection of child protection procedures.
Professionals should still bear in mind the considerations outlined in this guidance, and in particular should be alert to:
The Sexual Offences Act 2003 makes provision for young people aged under 16 years to be offered confidential professional advice on contraception, condoms, pregnancy and abortion.
It is good practice to follow the Fraser guidelines when discussing personal or sexual matters with a young person under the age of 16 (Lord Fraser, House of Lords ruling in case of Victoria Gillick v West Norfolk and Wisbech Health Authority & Department of Health and Social Security 1985). These hold that sexual health services can be offered without parental consent providing that:
This exception, in statute, covers not only health professionals, but also anyone who acts to protect a child, e.g. teachers, school nurses, careers service personal advisers, youth offending service officers, youth workers, social workers and parents.
In offering such advice, a person is not guilty of aiding, abetting or counselling a sexual offence against a child where they are acting for the purpose of:
Promoting emotional wellbeing includes exploring the part that sexuality plays in the young person’s sense of identity, the emotional implications of entering into a sexual relationship, and the characteristics of healthy relationships. Where appropriate, the needs and concerns of lesbian, gay, bisexual and transgender young people should be recognised and approached sympathetically. Professionals should consider the particular needs of young people with disabilities. Young people who have been abused may need specialist support, for example where sexual feelings are regarded as shameful or where past relationships have been violent or exploitative.
The duty of confidentiality owed to a person under 16 in any setting is the same as that owed to any other person, but the right to confidentiality is not absolute.
Where there is a serious child protection risk to the health, safety or welfare of a young person or others, this outweighs the young person’s right to privacy.
Research and experience have shown repeatedly that keeping children safe from harm requires professionals and others to share information. Such information sharing must be in accordance with legal requirements and the Information Sharing Protocol.
All young people, regardless of gender or sexual orientation, who are believed to be engaged in or planning to be engaged in, sexual activity must have their needs for health education, support and/or protection assessed by the agency/agencies involved.
Consideration should be given to how the young person can access associated assessments and support, and where necessary agencies should signpost or make a referral to appropriate provision.
On each occasion that a young person is seen by an agency, consideration should be given as to whether her/his circumstances have changed or further information has been given which may lead to the need for a referral or re-referral to Children’s Social Care
Where the child is considered to be suffering or likely to suffer significant harm a referral must be made to Children’s Social Care (see Referrals chapter).
In assessing the nature of any particular behaviour, it is essential to look at the facts of the relationship between those involved.
The following considerations must be taken into account when assessing the extent to which the child (or other children) may be suffering, or are at risk of suffering, harm (this list is not exhaustive):
It is important that all decision-making is undertaken with full professional consultation and never taken by one person alone. All discussions must be recorded, giving reasons for action taken and who was involved.
In cases of concern, where sufficient information is known about the sexual partner(s), the agency should check with other agencies, including the police, to establish what, if any, information is known about them. The police should normally share the required information without beginning a full investigation.
Where a serious crime is suspected, advice should be sought from the police at the earliest opportunity to safeguard the child and minimise the risk of any evidence, such as emails or pictures, being destroyed prior to an investigation.
Sexual abuse and exploitation of a child or young person involves an imbalance of power. Any assessment should seek to identify possible power imbalances within a relationship. These can result from differences in size, age, material wealth and/or psychological, social and physical development. In addition, gender, sexuality, race and levels of sexual knowledge can be used to exert power.
Where a power imbalance results in coercion, manipulation and/or bribery and seduction, these pressures can be applied to a young person by one or two individuals, or through peer pressure (i.e. group bullying). Professionals assessing the nature of a child or young person’s relationship need to be aware of the possibility that either or both of these situations can exist for the child or young person, and they should conduct a holistic assessment of the young person’s needs.
There will be an imbalance of power, and the child or young person will not be deemed able to give consent, if the sexual partner is in a position of trust or is a family member, as defined by the Sexual Offences Act 2003, and/or any pre-existing legislation.
Disabled children and young people are more likely to be abused than non-disabled children, and they are especially at risk when they are living away from home (see Children Living Away from Home). They may be particularly vulnerable to coercion due to physical dependency or because a learning disability or a communication difficulty means that it is not easy for them to communicate their wishes to another person. This increases the risk that a sexual relationship may not be consensual.
Professionals should not, however, assume that because a young person has a disability that they are not Fraser competent. Although there is a duty to protect from abuse and exploitation, professionals also need to recognise that disabled children have the right to a full life, including a sexual life.
A child or young person with a disability could be vulnerable to harm from a sexual relationship developed through inclusive activities. This may be in mainstream schools, education colleges, leisure centres and other places where children and young people meet where supervision is at a minimum. Staff need to be alert to the different capabilities of the children and young people they supervise, and assess risks accordingly.
Where professionals in Children’s Social Care have concerns that a relationship may present a risk of harm to an older disabled young person, they should begin work with the Adult Social Care services at an early point in order for there to be a smooth transition from protection under the Children Act 1989 to protection for the young person, from their 18th birthday onwards.
Doctors and other health professionals should consider the following issues when providing advice or treatment to young people on contraception, and sexual and reproductive health.
If a request for contraception is made, doctors and other health professionals should establish rapport and give a young person support and time to make an informed choice. It is important to take account of the capacity of a young person to make informed decisions, even if they are over 16 years old.
If a young person has a learning difficulty or disability, they should be encouraged to speak to an advocate of their choice to help their voice be clearly heard.
When considering a termination of pregnancy, it is particularly important to ensure that the young person has fully understood what is happening.
The following items should be discussed when providing advice or treatment to young people on contraception, and sexual and reproductive health:
Young people need to be able to talk to a trusted adult about sex and relationship issues. Although it is desirable that this person is their parent or carer, this is not always possible. The law allows staff to respect young people’s rights to confidentiality when discussing sex and relationship issues, and a disclosure of under-age sex is not of itself a reason to break confidentiality.
Young people should be made aware that confidentiality might be breached if they or another young person is at risk. In these circumstances staff should consult the young person and endeavour to gain their cooperation to a child protection referral. If that is not possible, they should be advised that their confidentiality would be breached.
Staff in schools should consider the need to establish links with colleagues in health to facilitate the delivery of advice/support and guidance on matters of sexual health.
While police and Children’s Social Care staff may provide advice and guidance to a young person involved in under-age sexual activity, both agencies have specific responsibilities with regard to criminal activities.
Children’s Social Care staff should inform police of actual and suspected criminal offences at the earliest possible opportunity in order to consider jointly how to proceed in the best interests of the child. Any decisions not to do so must be made at a senior level and recorded on the child’s file.
Guidance for Children’s Social Care staff indicates that, as Working Together is issued under Section 7 of the Local Authority Social Services Act 1970, a decision not to inform the police where an offence has been committed against a child should only be made where ‘exceptional circumstances justify a variation’ (LASSL (2004) 21). This is likely to be where the sexual relationship is considered consensual and not abusive, and may be most relevant in respect of children in care where children’s social care is also acting as the ‘corporate parent’ for the child.
In these circumstances it may be more important that the child receives appropriate advice regarding sexual health and contraception. This may be difficult if the young person is concerned that the police will be involved. Such a decision should always be made following consultation with line managers and should be recorded.
The police will proportionately investigate all criminal activities and make appropriate decisions in relation to the need for prosecution or not. Such decisions should always be made following consultation with line managers and should be recorded.
The priority for the police is the identification and investigation of under-age sexual activity where the relationship is abusive, either by being intra-familial in nature, or where there is a significant age/power gap between the parties involved.
Where young people of a similar age are involved in consensual sexual activity, or in other sensitive cases, the police role may be confined to the undertaking of information checks only. In such cases the police will not become directly involved in an investigation unless enquiries by the police or other agencies indicate the relationship is in fact abusive.
Both police and Children’s Social Care staff together may decide that there is no need for prosecution, but young people should be advised that their confidentiality cannot be maintained if staff from these agencies are involved.
Decisions to share information with parents and carers should be taken using professional judgement, consideration of the Fraser guidelines and in consultation with the child protection procedures. Decisions should be based on the child’s age, maturity and ability to appreciate what is involved in terms of the implications and risks to themselves. This should be coupled with the parents’ and carers’ ability and commitment to protect the young person.
Given the responsibility that parents have for the conduct and welfare of their children, professionals should encourage the young person, at all points, to share information with their parents and carers wherever safe to do so.
Those working directly with young people should give consideration to the role they may have in facilitating information sharing with parents/carers, in a planned way, in partnership with the young person.
RELATED GUIDANCE
Parents with Alcohol and Drug Problems: Adult Treatment and Family Services (gov.uk) – a toolkit containing guidance, data and other resources to support professionals who are helping families affected by parental alcohol and drug problems.
CONTENTS
Government guidance uses ‘parents with problem alcohol and drug use’ to refer to parents or carers of children whose alcohol or drug use causes, or has the potential to cause, harm to children. Dependent and non-dependent problematic use are both included in this definition.
Not all children of parents who use alcohol or drugs problematically will experience significant harm, but children growing up in these families are at a greater risk of adverse outcomes.
Research shows that problem alcohol and drug use can reduce parenting capacity and is a major factor in cases of child maltreatment. Department for Education (DfE) research on the characteristics of children in need has found parents using drugs to be a factor in around 17% of child in need cases, and parental alcohol use to be a factor in 16%. DfE analysis of serious case reviews also found that parental alcohol or drug use was recorded in over a third (36%) of reviews carried out when a child has died or been seriously harmed.
Families affected by parental alcohol and drug use typically have multiple support needs. In addition to alcohol and drug use, their support needs often include:
Parents’ dependent alcohol and drug use can negatively impact on children’s physical and emotional wellbeing, their development and their safety. The impacts on children include:
The harms children experience can cause problems in the short term and later in life. Evidence shows that this includes intergenerational patterns of:
Families affected by parental alcohol and drug use may need significant support to address the long-term effects of stigma and exclusion. Children and parents may need support and encouragement to get the courage to ask for and accept help and to talk openly about issues in the family.
Guidance – Parents with Alcohol and Drug Problems: Adult Treatment and Family Services (gov.uk) lists examples of how to overcome barriers to engagement:
There is consistent evidence of an association between parental alcohol and drug use and conflict. Parental conflict is defined in government guidance as ‘conflicts that occur between parents or carers that are frequent, intense and poorly resolved’. So, parental conflict can include a range of behaviours that fall short of domestic abuse.
Where parental alcohol and drug use and conflict coexist, the risk of poor outcomes for children is greater than when either is experienced alone. The nature of these outcomes derive from internalising (for example, anxiety and depression) and externalising (for example, aggression and hostility) behaviour. These are the same outcomes as for children who experience either parental substance misuse or conflict in isolation.
Few interventions exist to address parental substance misuse and conflict. But treatment services that integrate interventions to reduce parental conflict into the support they offer report that addressing the two problems together is effective at:
Effective safeguarding work between practitioners depends on collaborative working between all relevant local agencies, and that they recognise that no single professional has all of the required knowledge or skills for this work. This should include multi-agency training and evaluating and sharing good practice between agencies.
Adult and family services should be alert to potential problem alcohol and drug use by parents who they are providing help and support to. Staff in these services should understand the potential impact of problem alcohol and drug use on children and how that combines with other risk factors. Staff should also be clear what support their own service might be able to offer as well as what local pathways exist, so they can identify, assess and refer parents and affected children.
Guidance – Parents with Alcohol and Drug Problems: Adult Treatment and Family Services (gov.uk) recommends that alcohol and drugs services should have a ‘designated practitioner’ or ‘dedicated and named practitioner’ to:
Appropriate and timely information sharing between local partner agencies is essential to identify and support families.
Drug and alcohol treatment providers should (where relevant) ask adults who use their service if they or their partner are pregnant. Where they are known to have a child living with them (or may have a child live with them in the future), practitioners should make suitable enquiries as to the welfare of the children and share information with children’s social care and other agencies as appropriate.
The statutory guidance Working Together to Safeguard Children sets out the following principles in relation to information sharing:
For further information see Tier 1 – Children Safeguarding Data Sharing Agreement (DSA) and Data Protection chapters.
There should be a focus on early help and prevention for families affected by parental alcohol and drug use. This means providing support as soon as signs of a problem emerge, at any point in a child’s life or pre-birth. This relies on organisations working together to identify children and families who might benefit from early help, undertaking an assessment of need and providing targeted early help services to children and their families with a focus on improving outcomes for children. Support can come from a wide range of statutory, health and community services according to the level of need assessed. See also Early Help chapter.
Where there is a low level of assessed need, alcohol and drug treatment services should use referral pathways to local agencies and organisations which provide universal and targeted help to parents with alcohol and drug problems, and their children.
Local alcohol and drug treatment services can take steps to help prevent later harmful consequences for parents and children, including:
When alcohol and drug treatment and children and family services are considering the impact of parental alcohol and drug use on a child, they should jointly assess families using tools and guidance which factor in all the relevant information.
Collaborative assessment, information sharing and clear pathways between systems and services are vital to identifying families affected by drug and alcohol problems and ensuring they receive appropriate support early.
This can be strengthened locally by:
NICE Clinical Guideline ‘Pregnancy and Complex Social Factors: A Model for Service Provision for Pregnant Women with Complex Social Factors’ sets out that where a pregnant woman has substance misuse issues, antenatal services should work with local agencies, including social care and substance misuse services, to coordinate antenatal care by, for example:
The woman should be offered a named midwife or doctor who has specialised knowledge of, and experience in, the care of women who misuse substances, and provided with a direct line telephone number for the named midwife or doctor.
She should also be provided with information about the potential effects of substance misuse on her unborn baby, and what to expect when the baby is born, for example what medical care the baby may need and where the baby will be cared for.
Where a practitioner has concerns about a risk of significant harm to a child (including unborn children), they should make a referral to children’s social care (see Referrals chapter). If there is an imminent threat of serious harm, the police should be called and action taken to safeguard the child (see Immediate Protection chapter).
Substance misuse practitioners working with parents should be involved in, and provide relevant information to, processes and interventions such as early help, children in need and child protection enquiries, including attendance at strategy discussions and child protection conferences. Plans for parents and children should incorporate input from all relevant practitioners. See also Assessments chapter.
Assessment should take into account:
All practitioners working with parents / carers with substance misuse issues must maintain a focus on their children’s wellbeing and the parents’ ability to adequately care for and protect their children. They should monitor and review children’s progress throughout the period of intervention and respond appropriately to any change in the circumstances of the parents and / or the child.
Where parents are to be discharged from substance misuse services, practitioners must consider the potential impact for children and engage with children’s social care colleagues as appropriate. If the situation deteriorates such that a practitioner considers there to be a risk of significant harm to the child, a referral should be made to children’s social care.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
January 2026: A link to the Multi-agency Practice Principles for Responding to Child Exploitation and Extra-familial harm has been added. See above.
Some children will experience abuse and exploitation outside the home. This is often referred to as ‘extra-familial harm’. Harm can occur in a range of extra-familial contexts, including school and other educational settings, peer groups, or within community/public spaces, and/or online. Children may experience this type of harm from other children and/or from adults. Forms of extra-familial harm include exploitation by criminal and organised crime groups and individuals (such as county lines and financial exploitation), serious violence, modern slavery and trafficking, online harm, sexual exploitation, teenage relationship abuse, and the influences of extremism which could lead to radicalisation. Children of all ages can experience extra-familial harm.
Where there are concerns that a child is experiencing extra-familial harm, practitioners should consider all the child’s needs and vulnerabilities. Some children will have vulnerabilities that can be exploited by others and will require support appropriate to their needs to minimise the potential for exploitation. All children, including those who may be causing harm to others, should receive a safeguarding response first, and practitioners should work with them to understand their experiences and what will reduce the likelihood of harm to themselves and others.
Where children may be experiencing extra-familial harm, children’s social care assessments should determine whether a child is in need under section 17 of the Children Act 1989 or whether to make enquires under section 47 of the same Act, following concerns that the child is suffering or likely to suffer significant harm. A good assessment should:
See also Assessments procedure.
Where there are concerns that more than one child may be experiencing harm in an extra-familial context, practitioners should consider the individual needs of each child as well as work with the group. The children in the group may or may not already be known to local authority children’s social care. Working with the whole group enables practitioners to build an understanding of the dynamics between those within the group and the extra-familial context.
Practitioners will need to build an understanding of the context in which the harm is occurring and draw on relevant knowledge and information from the children and wider partners in order to decide on the most appropriate interventions. Practitioners should consider the influence of groups or individuals perpetrating harm, including where this takes place online, and identify patterns of harm, risk and protective factors in these contexts. This may include working across safeguarding and community safety partnerships to agree a plan for keeping children safe.
Key decisions should be recorded and communicated to both the child and their parents or carers, so that everyone understands the action that has, or will be, taken to safeguard and promote their welfare. It is important that all partners are clear how actions contribute to safeguarding and promoting the welfare of the child.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
The Prison Service will make a child safeguarding enquiry with children’s social care for all newly sentenced prisoners, and will identify prisoners who present an ongoing risk to children from within custody. Prisons will also decide on the level of contact, if any, they will allow between a prisoner and a child based on a child contact risk assessment. A prisoner’s contact with a child will be prohibited or restricted where necessary.
When a child safeguarding enquiry is received from a prison, children’s social care should:
The Probation Service will:
Information exchange between probation and children’s social care help both agencies develop a better understanding of the children and families they work with and ensures risk assessments are accurate and well informed.
Under the UK GDPR and Data Protection Act 2018 sharing an offender’s personal information must be lawful and fair and must comply with Part 3 of the Data Protection Act 2018 and in particular the data protection principles.
See also Tier 1 – Children Safeguarding Data Sharing Agreement (DSA) and Data Protection.
Sharing of information for the purposes of law enforcement and keeping children and young people safe meets one of the requirements for lawful processing under the Data Protection Act 2018, as the data sharing is authorised by law (under section 325(3) and (4) of the Criminal Justice Act 2003) (or section 14 of the Offender Management Act 2007). It is therefore not necessary for Prison and Probation Service staff to obtain consent from the offender under the Data Protection Act 2018.
For information exchange to be effective, children’s social care should:
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
Mother and baby units (MBUs) are discrete specialist accommodation, within some prisons, for female prisoners with children up to age of 18 months or above, where appropriate. Governors or Directors of prisons which have MBUs have a duty of care to the child.
When a woman applies for a place on a mother and baby unit (MBU), a referral for assessment must be requested by the prison from children’s social care in the mother’s home local authority at the earliest opportunity and must include information on MBU provision and policy. Any assessment should set out the needs of the child in relation to the mother’s application to be placed on an MBU.
The assessment should consider:
The lead practitioner responsible for the assessment should attend the MBU Admissions Board to represent the best interests of the child. When placed in an MBU, the mother retains full parental responsibility for the day-to-day care of the child, and the local authority in which the prison is located is responsible for safeguarding and promoting the welfare of the child.
The prison should actively engage children’s social care to ensure the relevant input into processes and individual cases. Practitioners should be provided with information on the purpose, facilities and support available on the MBU. Opportunities for practitioners to visit the MBU should be offered and encouraged.
Prisons must consult children’s social care on all MBU Board decisions, including decisions relating to a change in placement, and any other matters relevant to promoting the welfare and safeguarding a child.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
Any assessment of children in secure youth establishments should take account of their specific needs. In all cases, the responsibility for the welfare and safety of a child is located jointly with the home and host local authority. Any professional conduct issues should be dealt with by the local authority in which the establishment is located. Partners should work with the secure youth establishment and, where appropriate, the Youth Custody Service to ensure that the child has a single, comprehensive support plan.
Where a child becomes looked after, as a result of being remanded to youth detention accommodation (YDA), the local authority should visit the child and assess the child’s needs before taking a decision on how they should be supported. This information should be used to prepare the care plan, which should set out how the YDA and other practitioners will meet the child’s needs whilst the child remains remanded, and at any point of transition they will experience (either returning to the community or upon receiving a custodial sentence). The care plan must be reviewed in the same way as a care plan for any other looked after child.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
CONTENTS
A crucial role of children’s social care is to provide help and support to children with disabilities and their families. When undertaking an assessment of a child with disabilities, practitioners should recognise the additional pressures caring for a child with disabilities can place on the family, and the distinct challenges they may have had to negotiate as a result of their child’s disability.
The assessment process should focus on the needs of the child and family, be strengths-based, and gather information to inform decisions on the help needed to:
The local authority must also consider whether it is necessary to provide support under section 2 of the Chronically Sick and Disabled Persons Act 1970. Where a local authority is satisfied that the identified services and assistance can be provided under section 2 of the Act, and it is necessary in order to meet the needs of a child with disabilities, it must arrange to provide that support.
Where a local authority is assessing the needs of a child with disabilities, a carer of that child may also require the local authority to undertake an assessment of their ability to provide, or to continue to provide, care for the child, under section 1 of the Carers (Recognition and Services) Act 1995. The local authority must take account of the results of any such assessment when deciding whether to provide services to the child.
If a local authority considers that a parent carer of a child with disabilities may have support needs, it must carry out an assessment under section 17ZD of the Children Act 1989. The local authority must also carry out such an assessment if a parent carer requests one. Such an assessment must consider whether it is appropriate for the parent carer to provide, or continue to provide, care for the child. The assessment should also take account of parent carer’s needs and wishes, and the specific needs and circumstances of the child resulting from their disability. Parent carers have the right to request an assessment under section 17ZD of the Children Act 1989, including where a child is not otherwise known to children’s social care. Local authorities must ensure they have a process to facilitate these assessments if requested.
In line with the commitments made in the Special Educational Needs and Alternative Provision Improvement Plan, local authorities are encouraged to implement the role of Designated Social Care Officer (DSCO) in each local area. The DSCO role is intended to provide the capacity and expertise to improve the links between social care services and the SEND system. Similar to the Designated Clinical Officer (DCO) or Designated Medical Officer (DMO) role in health, the DSCO role will support both operational input (such as the contributions from care to education, health and care assessments) and more strategic planning functions (such as the commissioning of care services such as short breaks) for children with special educational needs and disabilities.
RELEVANT GUIDANCE
Modern Slavery: statutory guidance for England and Wales (Home Office)
Safeguarding children who may have been trafficked (Department for Education and Home Office)
CONTENTS
This chapter should be read in conjunction with the following government guidance: Care of unaccompanied migrant children and child victims of modern slavery: statutory guidance for local authorities (Department for Education) which sets out the steps which local authorities should take to plan for the provision of support for Looked After Children / Children in Care who are unaccompanied asylum seeking children, unaccompanied migrant children or child victims of modern slavery including trafficking. Elements of the guidance will also be relevant for the care of Looked After Children who are UK nationals and who may also be child victims of modern slavery.
The cohort of unaccompanied migrant children and child victims of modern slavery includes a wide range of children in a variety of circumstances that a local authority will need to be aware of in order to ensure that the child receives appropriate legal advice and support. Some will have been trafficked or persecuted and may have witnessed, or been subject to, horrific acts of violence. Other migrant children may have been sent to the UK in search of a better life, or may have been brought here for a private fostering arrangement and subsequently exploited or abandoned when the arrangement fails.
There are a wide range of status possibilities for migrant children that the local authority will need to be aware of. In brief, the following categories regarding status are the most likely to be encountered. However this list is not exhaustive and legal advice should be sought wherever there is uncertainty about a migrant child’s status.
Categories of unaccompanied children include:
Where it is established that a referral concerns a young unaccompanied child migrant, regardless of the category, this will always satisfy the criteria for services as a Child in Need.
An unaccompanied child will become a Looked After Child, after they have accommodated by the local authority under Section 20(1) of the Children Act 1989 for 24 hours. Once accommodated, they will be subject to the appropriate regulations and the same provision as any other Looked After Child.
The local authority should record any modern slavery concerns on the child’s care plan.
As part of the general duty to assess and meet the needs of an Unaccompanied Asylum Seeking Child, the local authority should ensure that the child has access to a legal representative.
Unaccompanied children are highly likely to require specialist support from a variety of organisations and agencies (see for example, the Independent Unaccompanied Asylum-Seeking Children Support Service (IUSS) provided by the Refugee Council).
All professionals involved in the care of unaccompanied children and child victims of modern slavery should be able to recognise indicators of trafficking, slavery, servitude and forced or compulsory labour and should have an understanding of the particular issues likely to be faced by these children.
This is a highly complex area of work, and professionals will need to have available to them a solid understanding of the asylum process or colleagues or other professionals with such expertise.
The kinds of issues that may need to be negotiated include:
For more information, see Processing children’s asylum claims (UK Visas and Immigration).
Social workers should also have a broad understanding of the immigration system – for example, the immigration application process, different types of leave, making further leave to remain applications and the appeals process. Social workers should also have an understanding of the trafficking referral process and the wider safeguarding system around child victims of modern slavery, including how and when to refer a child to the National Referral Mechanism (NRM).
Legal advice can only be provided by a registered immigration advisor, ideally one with expertise in working with children. Legal Aid is available for asylum cases and Looked After Children will generally be eligible.
Independent Reviewing Officers (IRO) should consider the child’s needs as an unaccompanied child or child victim of modern slavery, including trafficking, when planning and providing care. They should also have an awareness of the particular needs and issues children may face as a result of being an unaccompanied child or child victim of modern slavery so that they can provide appropriate challenge at review.
Service providers should ensure that foster carers and all other care staff in placement settings are aware of appropriate steps to reduce the risk of trafficked children returning to their traffickers.
Social workers should consider all unaccompanied migrant children as potential victims of modern slavery in the first instance until this possibility is either confirmed or discounted and they should also have an understanding of the trafficking referral process under the National Referral Mechanism.
The social worker must ensure that all unaccompanied children have access to specialist asylum and/or immigration legal advice and representation in their assessment so as to ensure the child can fully present their case for asylum or leave to remain.
The assessment will take account of:
Unaccompanied migrant children and child victims of modern slavery will need access to specialist legal advice and support. This will be in relation to immigration and asylum applications, and decisions and any associated legal proceedings. If they have been a victim of modern slavery, they will also need support in relation to criminal proceedings or compensation claims. The assessment should note that specialist legal support is required and how it will be provided. The child’s social worker should ensure that they are accompanied in all meetings, including meetings with legal professionals. The person accompanying the child does not have to be the child’s social worker.
In determining an unaccompanied young person’s accommodation needs, the assessment must have regard to their age and independent living skills and consider the intensity of service required. This may range between independent accommodation, semi-independent accommodation foster or residential placements, or in specific cases, a specialist residential therapeutic unit.
No assumptions should be made about the child’s language skills. An appropriately qualified and vetted interpreter must be used to assist in all assessments (see Interpreting, Signing and Communication Needs).
When completing cases records, it is important to pay particular attention to the detail of spelling names and of descriptions of family relationships.
Planning for the child should include planning for a variety of possible outcomes regarding the child’s immigration status – see Section 10, Asylum Process – Possible Outcomes.
Where the age of the child is uncertain and there are reasons to believe they are a child, they will be presumed to be a child in order to receive immediate assistance, support and protection in accordance with Section 51 Modern Slavery Act 2015. Assessments must be undertaken in accordance with standards established in case law and should only be carried out where there is reason to doubt that the child is the age they claim. For further guidance see: Age Assessment Guidance published by ADCS. In all cases where a referral is received concerning an unaccompanied child, the relevant Team will carry out an assessment in accordance with the Assessment Procedure, to determine whether they are a Child in Need.
Young unaccompanied child migrants should be provided with information about the services available to them from the local authority and other agencies.
The young person will also be given assistance to register with a GP and dentist, and enrol in a local school or college. The health professionals and the school should be aware of the child’s status and senior managers such as the Virtual School Head should be informed of the school placement. There will be a need to set out clearly any particular implications of the child’s status for non-specialist professionals such as GPs and teachers, including any urgency of involvement – particularly with health practitioners. An interpreter should be booked to accompany the young person to appointments with the GP or school, where necessary.
Where a young person’s needs are for independent or semi-independent accommodation, and the manager agrees, assistance should be given with completion of the necessary Housing Application.
Where the assessment identifies that an unaccompanied young child migrant needs to be Looked After, all the procedures in relation to Care Plans, Health Care Plans, Personal Education Plans and Placement Plans must be completed (see Decision to Look After, Buckinghamshire Children’s Social Care Procedures).
For unaccompanied migrant children who are Looked After, the placement decision will also need to be informed by careful consideration of the wider support needs of the child, including their cultural and social needs. It may be that the accommodation setting or carers cannot meet those needs on their own so other more creative ways, such as mentors or links to diaspora groups, could be used. As with all Looked After Children, an unaccompanied child’s ethnicity, cultural and linguistic background should be taken into account when placing the child with foster carers. However, these are not overriding considerations and should be taken into account alongside all of the child’s needs. Nevertheless, the placement should meet the child’s needs as a whole and be consistent with their wishes and feelings.
Where there are safeguarding concerns relating to the care and welfare of any unaccompanied child, including where modern slavery is suspected or has been identified, these should be investigated in line with the statutory provisions contained in Working Together to Safeguard Children. The opportunity to intervene to prevent any further exploitation might be very narrow, so the entry local authority should convene a Strategy Meeting/Discussion as soon as possible and take any necessary immediate action to safeguard and promote the child’s welfare. This Strategy Meeting/Discussion should involve the police, Immigration officials and any other relevant agencies and plan rapid further action if concerns are substantiated.
Provision may need to be made for the child to be in a safe place before any further assessment takes place and for the possibility that they may not be able to disclose full information about their circumstances immediately. The location of the child should not be divulged to any enquirers until their identity and relationship with the child have been established and the local authority is assured of their motives, if necessary, with the help of police and Immigration officials. The installation of police installed alarms should be considered and the child or young person advised about the safe use of mobile phones, so they cannot be traced etc.
All unaccompanied young asylum-seekers who are eligible for a service will be entitled to financial assistance which must first be authorised by the manager. The social worker should arrange for payment of the relevant amounts in accordance with the local authority procedures.
Travel cards or warrants will be issued to young unaccompanied asylum-seekers in relation to appointments at the Home Office.
Where an assessment identifies that an unaccompanied child migrant does not meet the criteria for a service from Children’s Social care but appears to be in need of services from elsewhere, the social worker will refer the young person to the appropriate agency which may be a different local authority Children’s Social Care department, the Refugee Council, UK Visas and Immigration and/or an appropriate voluntary agency.
In such circumstances, the duty social worker should make an appointment for the young person and advise them of the name, address (including a map where necessary) and contact number of the person with whom the appointment has been made. In addition, the duty worker must send a copy of the referral and assessment to the relevant office.
In all cases where a service is to be refused, the social worker must consult their manager before the decision is made and the letter confirming the decision is sent. Any correspondence received in relation to the decision should be referred to the manager.
The provision of a service is dependent on the young person continuing to qualify for the service.
Services to an unaccompanied child migrant may be withdrawn, for example, where another adult wishes to assume Parental Responsibility and this is assessed as appropriate.
The service must not be withdrawn without a Child in Need Plan Review (see Child in Need Plans and Reviews Procedure, Buckinghamshire Children’s Services) and the agreement of the social worker’s manager. Any such decision must be clearly recorded, with reasons. In all such cases, legal advice should usually be obtained before a final decision is made.
Where a service is withdrawn, the social worker should inform the Finance Office, if appropriate, immediately.
Planning transition to adulthood for unaccompanied children is a particularly complex process that needs to address their developing care needs in the context of their immigration status.
Pathway Planning to support an unaccompanied child’s transition to adulthood must cover the areas that would be addressed within any care leaver’s plan as well as any additional needs arising from their immigration status and the action required to resolve this. (See Leaving Care and Transition Procedure, Buckinghamshire Children’s Services.)
Former unaccompanied children who qualify as care leavers and who have been granted leave to remain, or who have an outstanding asylum or other human rights claim or appeal, are entitled to the same level of care and support from the local authority as any other care leaver.
The extent of any care leaver duties on local authorities to provide support to former unaccompanied children who have turned 18, exhausted their appeal rights, established no lawful basis to remain in the UK and should return to their home country is subject to a Human Rights Assessment by the local authority. This is set out under the restrictions on local authority support for adults without immigration status.
For former unaccompanied children whose long-term future is in the UK, transition planning will need to consider the challenges and issues facing any care leaver, such as education or preparing for independent living. Planning for children and young adults who have been granted refugee status or humanitarian protection should also consider when they may be required to make a further application for leave to remain.
Where an unaccompanied child or child victim of modern slavery qualifies for local authority care leaving support, a personal adviser must be appointed to support them.
Pathway plans should always consider and reflect the implications for the child or young adult if their asylum claim is refused without a grant of leave, if their application to extend their leave is refused or if their appeal against a refusal is dismissed. In such circumstances, the person will become unlawfully present in the UK and be expected to make plans for a return to their home country. A plan for a return to their home country may also need to be made at any other point, should the care leaver decide to leave the UK.
Planning may have to be based around short-term achievable goals whilst entitlement to remain in the UK is being determined. For the majority of unaccompanied children who do not have permanent immigration status, transition planning should initially take a dual or triple planning perspective, which, over time should be refined as the young person’s immigration status is resolved.
Planning cannot pre-empt the outcome of any immigration decision and may be based on:
Assistance should be given in advance of their 18th birthday with the necessary applications for housing, Housing Benefit and any other relevant benefits. The social worker must ensure that the young person has accommodation to which to move on their 18th birthday. The provider of the young person’s present accommodation and the Finance Office should be informed when the accommodation arrangement will end.
Financial support for care leavers who are former unaccompanied child migrants should reflect their needs and their immigration status. Financial policies should highlight any entitlements and how their immigration status may affect these. Pathway plans should address employment opportunities and funding arrangements for education and training, taking account of the young person’s immigration status.
If a young person has No Recourse to Public Funds (NRPF), they will be unable to access a number of welfare benefits and social housing. Subject to the Human Rights Assessment by the Local Authority under Schedule 3 Nationality, Immigration and Asylum Act 2002 (as amended), the provision of accommodation may form part of the Leaving Care support provided to a young person who has NRPF. For further information please go to Families with No Recourse to Public Funds Procedure, Buckinghamshire Children’s Services.
Having NRPF does not prevent a person from accessing other publicly funded services, but many of these will have eligibility criteria based on immigration status which will need to be considered. (See NRPF Network – What are public funds?)
Where a young person is Looked After, their circumstances will be reviewed in accordance with the Looked After Reviews Procedure.
Any other services provided should be reviewed at least every 6 months as set out in the Child in Need Plans and Reviews Procedure.
In advance of each review, the social worker will send the young person a checklist setting out the documents which are required to be produced at the Review, such as confirmation of registration with a GP, enrolment at schools/college and updated information concerning their asylum status.
The young person should be invited to the Review and an interpreter should be booked as necessary.
Independent Reviewing Officers (IRO) should have regard to the child’s needs as an unaccompanied child or child victim of modern slavery, including trafficking, when planning and providing care. They should also have an awareness of the particular needs and issues children may face as a result of being an unaccompanied child or child victim of modern slavery so that they can provide appropriate challenge at review. Service providers should ensure that foster carers and all other care staff in placement settings are aware of appropriate steps to reduce the risk of trafficked children returning to their traffickers.
Guidance for cases where the child has been the subject of sexual exploitation can be found in the Multi Agency Child Exploitation Protocol.
Where a Review confirms the service, the Financial Assessment Form should be updated. Where additional support services are identified as necessary, the Plan should be updated to reflect this.
Where services are withdrawn as a result of the Review, the relevant teams should be notified immediately.
There are four main possible outcomes of the asylum process for an unaccompanied child, which will determine what the long term solution might be:
Granted refugee status (i.e. granted asylum), with limited leave to remain for five years, after which time they can normally apply for settlement (i.e. indefinite leave to remain);
Refused asylum but granted humanitarian protection, with limited leave to remain for five years, after which time they can normally apply for settlement (i.e. indefinite leave to remain). This is most commonly granted where the person is at risk of a form of ‘ill treatment’ in their country of origin but which does not meet the criteria of the Refugee Convention. As it is very likely that those granted refugee status or humanitarian protection will qualify for indefinite leave to remain, their care and pathway planning should primarily focus on their long-term future in the UK, in the same way as for any other Care Leaver;
Refused asylum but granted Unaccompanied Asylum Seeking Child (UASC) Leave. This is normally for 30 months or until the age of 17½, whichever is the shorter period. This form of leave is granted to unaccompanied children where they do not qualify for refugee status or humanitarian protection, but where the Home Office cannot return them to their home country because it is not satisfied that safe and adequate reception arrangements are in place in that country. It is a form of temporary leave to remain and is not a route to settlement. It is important to note that this decision is a refusal of the child’s asylum claim and will attract a right of appeal. The child should be assisted to obtain legal advice on appealing against such a refusal. Before the child’s UASC Leave expires, they can submit an application for further leave to remain and/or a fresh claim for asylum, which will be considered. It is essential that they are assisted to access legal advice and make any such further application or claim before their UASC Leave expires. In such cases, care and pathway planning should therefore consider the possibility that the child may have to return to their home country once their UASC Leave expires or that they may become legally resident in the UK long-term (if a subsequent application or appeal is successful). Planning should also cover the possibility that they reach the age of 18 with an outstanding application or appeal and are entitled to remain in the UK until its outcome is known;
Refused asylum and granted no leave to remain. In this case the unaccompanied child is expected to return to their home country and their care plan should address the relevant actions and the support required. The Home Office will not return an unaccompanied child to their home country unless it is satisfied that safe and adequate reception arrangements are in place in that country. Any appeal or further application should be submitted where appropriate by the child’s legal adviser.
Although the above are the four main types of outcomes for an unaccompanied child, there may be others. For example, a child may be granted discretionary leave depending on whether they meet other criteria such as needing to stay in the UK to help police with their enquires after being conclusively identified as a victim of trafficking. Other examples include: leave as a stateless person; limited or discretionary leave for compassionate reasons; and limited leave on the basis of family or private life.
Local Government Association – Council Support: Refugees, Asylum Seekers and Unaccompanied Children – resource for council staff, designed to answer questions about supporting refugees, asylum seekers and unaccompanied children.
National Referral Mechanism: Guidance for Child First Responders – provides details on how to refer a child into the NRM and complete the referral form, reviews of decisions and the benefits of referral.
Guidance on Processing Children’s Asylum Claims – Case worker guidance – sets out the process which immigration officials follow in determining an asylum claim from a child and the possible outcomes for the child
Modern Slavery and Exploitation Helpline (Unseen)
National Transfer Protocol for Unaccompanied Asylum Seeking Children – interim national transfer procedure and transfer flow chart for the safe transfer of UASC from one UK Local Authority to another.
Child Protection: Working with Foreign Authorities (Department for Education) – guidance on child protection cases and care orders where the child has links to a foreign country
Modern Slavery: How to identify and support victims (Home Office)
RELATED GUIDANCE
CONTENTS
Where the local authority plan to return a child to the care of their family, an assessment should be carried out while the child is looked after as part of the care planning process (under regulation 39 of the Care Planning Regulations 2010).
This assessment should consider what services and support the child and their family might need once the child ceases to be looked after. Family group decision-making, such as family group conferences, can be used to establish how the family network will support the child to return home. The outcome of this assessment should be included in the child’s care plan.
The decision to cease to look after a child will, in most cases, require approval under regulation 39 of the Care Planning Regulations 2010. Practitioners must carry out an assessment of need for eligible children to consider their eligibility for independence and transition into adulthood.
There should be a clear plan for all children who return home that reflects the current and previous assessments, focuses on outcomes, and includes details of services and support required. Following the child’s return home:
The impact of services and support should be monitored and recorded, and where a child is remanded to local authority or youth detention accommodation, consideration must be given to what ongoing support and accommodation the child may need after their period of remand. This should be included in their care plan.
Where a child who is accommodated under section 20 of the Children Act 1989 returns home in an unplanned way, (for example, the decision is not made as part of the care planning process, but the parent removes the child, or the child decides to leave), the local authority should work with partner agencies to consider whether there are any immediate concerns about the safety and wellbeing of the child. This could include harm from outside the home. The local authority should take appropriate action, including considering making enquiries under section 47 of the Children Act 1989, if there is concern that the child is suffering or likely to suffer significant harm (see Section 47 Enquiries chapter).
RELATED CHAPTER
Tier 1 – Children Safeguarding Data Sharing Agreement (DSA)
RELATED INFORMATION
Sarah’s Law (Child Sex Offender Disclosure Scheme) Thames Valley Police
CONTENTS
The aim of the Child Sex Offender Disclosure Scheme is to provide parents, guardians, and carers with information that will enable them to better safeguard their children’s safety and welfare. It introduced the principle of a two-way disclosure by enabling the public to ask about the history of a person who has access to their child. It enables limited public access to information about registered sex offenders.
Under the Scheme, there is a ‘right to ask’ for information, whereby a person can make an application to the police for information about a person (subject) who has some form of contact with a named child or children. This could include any third party, such as a grandparent, neighbour, or friend; it does not need to be a relative of the child.
‘Contact’ means the person has enough access to a specific child to pose a real risk of harm. For example:
In the event that a subject has convictions for sexual offences against children, poses a risk of causing harm to the child concerned, and disclosure is necessary to protect the child and is a proportionate response to manage that risk, there is a presumption that this information will be disclosed. However, any disclosure under the Scheme will only be made to the person best placed to protect the child. This may not be the individual that made the application.
Each request for information will be dealt with on a case-by-case basis and, while there may not be information that can be disclosed in accordance with the Scheme, disclosure of other relevant information may still be possible
You can:
When you ask for a check, you’ll need to:
It can take up to 28 days for the police to finish a check. If the child is in immediate danger, then the police will act right away before the check is finished.
In the first 24 hours after you ask for a check, the police will work with you to find a safe way to keep in touch.
Within 10 days of asking for a check, you’ll need to attend a meeting or have a call with the police to:
If the police cannot confirm your identity, you cannot be told the results of the check. The police will still act to keep the child safe.
If the police have found any relevant information, they’ll decide who needs to be told. This might not be you.
It will usually be the people best placed to protect the child, such as the child’s parent, guardian or carer.
The police will normally tell the person who was checked that they’re sharing this information, if they decide it’s safe to do that. This might include telling the person that you asked for the check. The police will talk to you when making this decision.
The police will only share information with you if you sign an agreement promising not to tell anyone else.
If you think there are other people who should be told, ask the police about this.
In addition to the ‘right to ask’ (where an applicant contacts the police to ask for information), there is also a ‘right to know’. The “Right to Know” is where the police receive indirect information that may impact the safety of children and have not received a request for information through the ‘Right to Ask’ process. This could include (but is not limited to):
The purpose of the ‘Right to Know’ is to allow the police to act proactively when they are in receipt of information about a risk to a child or children, when it is already known that disclosure is necessary and proportionate.
The ‘Right to Know’ is also known as Sarah’s law or Child Sexual Offender Disclosure Scheme (CSODS).
RELATED GUIDANCE
Dogs and Children: Living Safely Together (Dogs Trust)
CONTENTS
Under the Dangerous Dogs Act 1991 (as amended), it is a criminal offence to allow a dog to be dangerously out of control anywhere, such as:
A dog is considered dangerously out of control if it:
A court could also decide that a dog is dangerously out of control if either of the following apply:
This applies to all dogs.
It is also a criminal offence to own certain specific types of dog:
It is also an offence to:
It is important to recognise that any dog can present a potential risk of harm to babies and children, and where dogs are present in the home, the risks should be assessed.
Any dog can bite if it is worried or scared and feels it has no other choice. 70% of all dog bites in the UK are to children, making them the most at-risk age group. 91% of bites to children occur within the home by a known dog, often their own dog. From a dog’s point of view, children behave very differently to adults, being unpredictable and prone to making a lot of noise, meaning supervision by parents/carers within the home and outside is crucial to keeping children safe.
Keeping Children Safe Around Dogs (RSPCA) recommends six ‘golden rules’ for parents / carers to help keep children safe around dogs, including never leaving your child alone in the same room as a dog, even your own and always supervise your child when they are with your dog.
Guidance: Code of Practice for the Welfare of Dogs (Department for Environment, Food & Rural Affairs) sets out practical guidance on how to provide a suitable environment for a dog to live in, based on the requirement of Section 9 of the Animal Welfare Act 2006.
Dogs may pose a higher risk of harm to children where:
An assessment should consider:
Practitioners should ask to see the dog and where / how it is kept.
Assessment of the risks posed by dogs in the household should be an ongoing process not a one-off event as circumstances may change.
Where there is assessed or known to be a risk of significant harm to a child, or where harm has already occurred such as the dog attacking a child, a referral should be made to children’s social care and safeguarding processes engaged (see Referrals chapter). Relevant agencies should be informed, such as police where there is a known or suspected criminal offence.
CONTENTS
Lord Justice Ryder wrote, in a court judgement from 2005:
“The terms ‘Munchausen Syndrome by Proxy’ and ‘Factitious (and Induced) Illness (by Proxy)’ are child protection labels that are merely descriptions of a range of behaviours, not a paediatric, psychiatric or psychological disease that is identifiable. In reality, the use of the label is intended to connote that in the individual case there are materials susceptible of analysis by paediatricians and of findings of fact by a Court concerning fabrication, exaggeration, minimisation or omission in the reporting of symptoms and evidence of harm by act, omission or suggestion (induction).
For my part, I would consign the label MSBP to the history books and however useful FII may apparently be to the child protection practitioner I would caution against its use other than as a factual description of a series of incidents or behaviours that should be accurately set out (and even then, only in the hands of the paediatrician or psychiatrist/psychologist).
What I seek to caution against is the use of the label as a substitute for factual analysis and risk assessment. “
For further information, please see A County Council v A Mother & Ors [2005] EWHC 31 (Fam)
This guidance strongly promotes the recommendations of Lord Justice Ryder.
Fabricated or Induced Illness (FII) is a term used increasingly by professionals from all agencies involved in safeguarding and protecting children. However, there remains debate and disagreement about the nature and definitions of FII. For the purposes of this guidance, FII is considered as, ‘a clinical situation where a child has suffered or is likely to suffer significant harm through the fabrication, falsification, or induction of illness by a carer and/or from responses to these parental actions by health professionals.
By using the term FII, health professionals are expressing their concerns that the child has suffered or is likely to suffer significant harm. In describing the harm, all professionals, health, and non-health, are encouraged to use the language of Working Together to Safeguard Children, which is multi-agency statutory guidance published by the Department for Education.
Medically Unexplained Symptoms (MUS): In Medically Unexplained Symptoms (MUS), a child’s symptoms, of which the child complains, and which are presumed to be genuinely experienced, are not fully explained by any known pathology. The symptoms are likely based on underlying factors in the child (usually of a psychosocial nature), and this is acknowledged by both clinicians and parents. MUS can also be described as ‘functional disorders’ and are abnormal bodily sensations which cause pain and disability by affecting the normal functioning of the body. The health professionals and parents/carers work collaboratively to achieve evidence-based therapeutic work in the best interests of the child or young person.
Perplexing Presentations (PP): The term Perplexing Presentations (PP) has been introduced to describe the commonly encountered situation when there are alerting signs of possible FII (not yet amounting to likely or actual significant harm), when the actual state of the child’s physical, mental health and neurodevelopment is not yet clear, but there is no perceived risk of immediate serious harm to the child’s physical health or life. The essence of alerting signs is the presence of discrepancies between reports, presentations of the child and independent observations of the child, implausible descriptions and unexplained findings or parental/carer’s behaviour.
Fabricated or Induced Illness (FII): FII is a clinical situation in which a child is, or is very likely to be, harmed due to parent(s)/carer(s) behaviour and action, carried out in order to convince doctors that the child’s state of physical and/or mental health and neurodevelopment is impaired (or more impaired than is actually the case). FII results in physical and emotional abuse and neglect, as a result of parental/carer’s actions, behaviours or beliefs and from doctors’ responses to these. The parent or carer does not necessarily intend to deceive, and their motivations may not be initially evident. It is important to distinguish the relationship between FII and physical abuse / non-accidental injury (NAI). In practice, illness induction is a form of physical abuse. In order for this physical abuse to be considered under FII, evidence will be required that the parent’s/carer’s motivation for harming the child is to convince doctors about the purported illness in the child and whether or not there are recurrent presentations to health and other professionals. This particularly applies in cases of suffocation or poisoning.
Alerting Features – these are clinical features associated with child maltreatment that may be observed when a child presents to healthcare professionals.
Consider – to consider child maltreatment means that maltreatment is one possible explanation for the alerting feature.
Suspect – to suspect child maltreatment means a serious level of concern about the possibility of child maltreatment but not proof of it.
In recognising the harm caused by FII, the effect and impact on the child should be the major concern of professionals caring for the child. Professionals are encouraged to consider the lived experience of the child and to listen to the voice of the child.
Rather than concentrating on diagnoses, professionals should consider the following:
Induction of illness: Induction of illness is rare. The commonest forms of induced illness are poisoning (usually by prescription medications) and suffocation. When the illness induction stops, the child may return to normal health but can still remain at risk of further harm. Further harm is likely to occur from medical interventions to investigate the cause of the child’s illness (iatrogenic harm) and the emotional impact on the child.
Falsification of illness: Falsification of illness is also rare. Clinical samples reported to be from the child can be tampered with or may not come from the child. For example, (e.g., non-human blood on clothing reported to have come from the child; urine samples can have sugar or blood added to them; thermometers can be warmed up with hot water).
Results of medical tests can be falsified or letters reportedly from health practitioners can be forged. Photographs reportedly of the child may be from another child or faked to look like a medical condition.
Fabrication of illness: Fabrication of illness is commonly encountered by health professionals. The situation can often be resolved through open discussion and careful management, however, where this is not possible, the child can sometimes experience significant harm.
Parents or carers may or may not realise that they are giving an incorrect account of the child’s health. Their description will depend upon multiple factors including parental health and health beliefs, culture, previous experience of healthcare and experience of childcare. Naïve exaggeration and deceitful lying could both be described as fabrication but are very different in how they should be managed.
Alerting signs are not evidence of FII. However, they are indicators of possible FII (not amounting to likely or actual significant harm) and, if associated with possible harm to the child, they amount to general safeguarding concerns.
Some alerting signs are initially recognised by community or primary health care professionals such as health visitors, GPs or community paediatricians, Social Care staff or by professionals in pre-school/early years, schools and other educational settings. Others are first noted by hospital-based paediatricians or in Child and Adolescent Mental Health Services (CAMHS).
The essence of alerting signs is the presence of discrepancies between reports, presentations of the child and independent observations of the child, implausible descriptions and unexplained findings or parental behaviours. Alerting signs may be recognised within the child or in the parent’s behaviour. A single alerting sign by itself is unlikely to indicate possible fabrication. It is important to look at the overall picture which includes the number and severity of alerting signs.
Clinical evidence suggests that fabricated or induced illness is usually carried out by the child’s mother or a female carer. However, practitioners should also be aware of the possibility of other perpetrators including fathers, grandparents, siblings or other children, or practitioners.
Parents/carers may have the following history or exhibit a range of alerting behaviours when they wish to convince others that their child is ill:
These patterns of behaviours are coercive, isolating and controlling and are patterns we see in a grooming process. Parents/carers could be grooming professionals through behaviours which could seek to initially get professionals to feel sorry for them, ingratiate themselves and then this can move on to intimidation.
Significant harm is defined in the multi-agency Continuum of Need Incorporating Threshold Guidance as a situation where a child is suffering, or is likely to suffer, a degree of physical, sexual and/or emotional harm (through abuse or neglect) which is so harmful there needs to be statutory intervention by child protection agencies in the life of the child and their family.
The harm caused by medical investigations and treatments always has to be balanced against their benefits. Carrying out tests, giving medicines or performing surgery on a child whose symptoms are misreported is more harmful than if symptoms are genuine. Harm can be caused directly by the parent, intentionally or unintentionally, and this harm may be reinforced by health professionals who cause iatrogenic harm inadvertently.
It is important to judge the severity of harm to the child rather than severity of a parent’s/carer’s actions. Severity of harm to the child should be assessed both by the intensity of each aspect of harm and by the cumulative effect of all the aspects. Whilst the motivation of the parent/carer is irrelevant to the determination of whether the child has suffered or is likely to suffer harm, motivation needs to be considered when planning how to manage the problem.
In the context of FII harm may be caused by physical abuse, emotional abuse or neglect. Although some of these children die, there are many that do not die as a result of having their illness fabricated or induced, but who suffer significant long term physical or psychological health consequences.
Physical abuse may include unnecessary pain and discomfort from unnecessary surgery, anaesthetic, medical investigations, procedures and treatments or through the precipitation of an illness by withholding medication.
Emotional abuse may include making the child unnecessarily anxious about their health and/or experience of healthcare, inducing psychiatric disorders and psychosocial difficulties causing social isolation so that the child’s sense of self is damaged.
Neglect may include disrupted education with unnecessary school absence and/or parental restrictions on participation in usual activities and genuine illness being overlooked.
The child’s views are important to ensure we understand how they view their symptoms and any concerns or worries that they may have. Children must be given opportunities to have their views explored, away from parents, in settings where they feel safe. Children can find it difficult to express views independently of their parents. In instances where a child is non-verbal or has communication difficulties either by language or ability, then the support of interpreting and/or specialist communication may need to be sought.
Previous FII guidance suggested that parents/carers should not be informed of safeguarding concerns until multiagency assessment had taken place. However, it is now agreed that parents/carers should be kept informed unless this would place the child at real risk of further harm.
In order to address alerting features before further harm is caused to a child, it is important that professionals are able have honest discussions with parents/carers and children at the earliest opportunity, so that a plan can be agreed to ensure the child’s wellbeing. However, a decision of who, how and when this should happen needs to be agreed by the professionals involved with the child and family at an early multi-agency discussion/professionals meeting.
If it is considered that a child is being harmed through FII, as with any other safeguarding concern, professionals should inform parents/carers (and children if appropriate) about referral to Children’s Social Care unless this would place the child at risk of further harm. An example where parents/carers might not be informed of contact with Children’s Social Care is in induced illness where poisoning is suspected. In this situation immediate protection may be needed to keep the child safe.
If you are uncertain whether to inform parents/carers take advice from your safeguarding lead or the named or designated doctor for safeguarding children. It is advised that you avoid terms such as fabrication or fictitious illness but explain to the parent/carer that they appear to be misunderstanding or processing the medical information in a way that may cause harm to their child for example missing school or not being able to participate in certain activities and therefore a referral to Children’s Social Care is being made to support them and the professionals involved with the child in understanding the medical needs of the child and to ensure that the risk to the child is reduced by supporting them with a Health and Education Rehabilitation plan.
If professionals decide not to share safeguarding concerns with parents/carers, there should be a well-considered risk assessment with clear documentation and early multi-agency discussion. Advice on whether to share safeguarding concerns in the context of FII can be obtained from Designated and/or Named Health Professionals. Professionals should note that seeking relevant permissions and informing parents and carers is to be reviewed on a regular basis by Managers, lead paediatrician and Named Doctor/Nurse, alongside partner agencies.
Careful, factual records should be kept, detailing who reported any concerns, what was observed, and by whom. Records of discussions, including about safeguarding concerns, should be kept within the child’s records (including their main health record), to ensure that this information is readily available to those involved in the child’s care, aiming to prevent further harm.
Records should include a clear explanation of the specific concerns and, where appropriate, a risk analysis based on the concerns and the professional’s opinion of these. Similarly, documentation of the harm to a child should use the recognised forms of harm. Records must include a clear account of what has or has not been discussed with the child and parents/carers.
It is recommended that professionals use caution or avoid the term ‘Fabricated or Induced Illness’ when writing records , it may be helpful to use terms such as ‘we are concerned that the parent/care giver is processing information about the child’s health in a manner that may cause harm to the child’.
See also Flowchart 1: Action if there are Alerting Signs of FII (opens as a PDF)
All professionals who have concerns about a child’s health should discuss these with their line manager, their agency’s designated safeguarding children adviser and the GP or paediatrician responsible for the child’s health. If the child is receiving services from local authority Children’s Social Care, the concerns should also be discussed with them.
It is recommended that school explain to the parents/carers that information is required from health to understand the concerns e.g. poor school attendance. It is then appropriate for education to contact health (either GP, consultant paediatrician or child psychiatrist) with their query about the actual health of the child. If parents/carers do not agree to health assessment or sharing of information, advice can be sought from organisational safeguarding leads and/or from Named or Designated Health Professionals.
If primary healthcare (GP) is the only contact for the child, then they may wish to refer to an appropriate secondary care consultant for further assessment of the child’s health. The referral must be explicit about the alerting features. If the response from health is felt to be inadequate, education can contact either the Named GP or Named Doctor for Safeguarding Children for advice.
In perplexing cases opportunities for multi-agency sharing of information, collaboration, planning and challenge should take place on a regular basis via review multi-agency meetings.
A “Responsible Consultant “, i.e., a consultant paediatrician (or, in cases of fabricated mental illness, a senior CAMHs practitioner), will lead on case management with a focus on the child’s voice and their current state of health, functioning, and involvement with health services. If initial concerns are raised in primary care or education, then a referral to an appropriate consultant should be made as in Section 8.1,Action if the initial concerns arise directly from education and not health.
Where there are concerns about more than one child in a family, each child may have a different or the same Responsible Consultant depending on the needs of the children involved. If there is disagreement about who should be the Responsible Consultant for a child, this should be discussed with the Named and/or Designated Doctor.
The Responsible Consultant should lead in liaising with all the other professionals involved to reach consensus about the child’s health and management, and then will discuss with the child and family:
A Health and Education Rehabilitation Plan should be agreed and implemented. The “Responsible Consultant” will lead on the plan, but this must be shared with all agencies involved. The plan must specify timescales and intended outcomes and be monitored and reviewed regularly. The Plan may include:
When FII is considered and/or suspected, parental or carer non-engagement, disguised and/or partial compliance are common, and need to be managed by the Responsible Consultant, together with the multi-agency team. If the parents/carers do not engage and/or oppose professionals plan for the child, the professional will have to consider whether the parents’ /carers’ actions or non-actions might lead to the child suffering significant harm and so whether referral to children’s services is indicated.
If parents/carers do not engage with the plan and the child is not considered to be at risk of significant harm the case should be reviewed to see whether monitoring and containment are appropriate. Advice may be sought from named or designated health professionals.
If the child has a social worker allocated by Children’s Services, Children’s Services will take the lead for safeguarding, working closely with the multi-agency team, particularly health and education, who will take the lead for their aspects of the case.
See also Flowchart 2: Action is Significant Harm is Suspected (opens as a PDF)
The process for the management of cases where there are concerns that a child has suffered or is likely to suffer significant harm from FII is the same as for any other case of child maltreatment. See also Section 47 Enquiries.
If at any stage, the Responsible Consultant or other professionals have concerns that the child has suffered or is likely to suffer significant harm, then the MASH should be contacted, and an urgent strategy discussion must take place with the Responsible Consultant (can include a Named or Designated Health professional) and action taken to make the child safe in accordance with each agency’s role and responsibility. Social Care, in this scenario, must. invite their Legal Representative to the Strategy Meeting. Other agencies should consider taking their own legal advice if there are concerns regarding non engagement or disguised compliance.
If there is evidence of illness induction or frank deception, such as interfering with specimens or medicine charts, urgent contact should be made with MASH, or, if needed, out of hours, with police and/or children’s services. If there are concerns of illness induction whilst a child is on the ward, for example a parent/carer interfering with medication, equipment or charts, then action should be sought to remove the parent/carer from the ward as they pose a risk to children at that point.
Chronologies are a useful tool in Perplexing Presentations or cases of FII. They should:
Chronologies should be compiled by individuals who have the expertise and ability to recognise and comment on any significant episodes. The Responsible Consultant (with support from the Named and/or Designated Doctor) is usually best placed to overview and analyse the combined multi-agency chronology and provide a report on this.
See Appendix 1 for the agreed multiagency chronology format. It is important that the headings and format are agreed across organisations and agencies so that they can be collated easily.
In most circumstances, there is agreement between professionals as to whether or not a child is at risk of significant harm and the process that should be followed. However, professional challenges should be seen as part of healthy professional working relationships.
If there are concerns about the health response from professionals (including concerns from education settings), advice can be sought from the Named GP, the Named Doctor for Safeguarding in a community or hospital trust, or from Designated Health Professionals.
If any professional considers that their concerns are not taken seriously or responded to appropriately, they should escalate their concerns following the Escalation, Challenge and Conflict Resolution Procedure.
Working Together to Safeguard Children (Department for Education) – The statutory guidance does not mention FII and FII is not a specified form of child abuse. However, within the definition of physical abuse it states that
‘Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child’.
Child Maltreatment: when to suspect maltreatment in under 18s (National Institute for Health and Care Excellence)- Contains limited guidance on when to consider FII (see paragraphs 1.2.11 – 1.2.12)
Perplexing presentations / fabricated or induced illness in children (Royal College of Paediatrics and Child Health)– This guidance is written primarily for paediatricians but can be helpful for other health professionals.
Assessment and management of adults and children in cases of fabricated or induced illness(FII) ( Royal College of Psychiatrists) – provides guidance for mental health professionals (MHPs), including psychiatrists, who may be asked to assess and manage adults and children where there is evidence of or concerns about abnormal illness-related behaviour by care givers.
Appendix 1 – Chronology of Significant Events: Template (opens in Word)
Appendix 2 – Flowchart 1: Action if there are Alerting Signs of FII (opens as a PDF)
Appendix 3 – Flowchart 2: Action if Significant Harm is Suspected (opens as a PDF)
RELEVANT INFORMATION
Forced marriage and learning Disabilities: multi-agency practice guidelines (HM Government)
Forced Marriage Resource Pack (Home Office) – examples of best practice to ensure that effective support is available to victims of forced marriage
Forced Marriage: A Survivor’s Handbook (Foreign, Commonwealth & Development Office)
RESOURCES FOR RAISING AWARENESS
Forced Marriage – Free e-learning
The Foreign and Commonwealth office have produced a series of short YouTube videos covering the consequences of forced marriage, and how to spot the signs of a forced marriage.
FOR PEOPLE DIRECTLY AFFECTED – If you’re trying to stop a forced marriage or you need help leaving a marriage you’ve been forced into, contact the Forced Marriage Unit (FMU)
In an emergency call the Police on 999
CONTENTS
A forced marriage is one where one or both parties do not or cannot consent to the marriage. Pressure may be applied to agree to the marriage, but, under the Marriage and Civil Partnership (Minimum Age) Act 2022 it is a criminal offence to do any acts for the purpose of causing a child (before their 18th birthday) to marry, whether or not any forms of coercion take place.
The pressure put on children to marry against their will can be:
Forced marriage can happen to boys and girls (although most cases involve girls) and there is no ‘typical’ victim of forced marriage.
Forced marriage can take place anywhere in the world, including in the UK. In many cases forced marriage involves a potential partner being brought into the UK from overseas or a British person being taken abroad for the forced marriage, often without them knowing that they are going to be married. Forced marriage of any person, regardless of sex, age, disability, ethnic origin or sexual orientation, is illegal in the UK (see Section 5, Forced Marriage Offences).
Forced marriage is very different to an arranged marriage, which is where families of both parties take a lead in the arrangements for the marriage, but they are free to decide whether they want the marriage to go ahead or not.
People who force others into marriage often try to justify their behaviour as ‘protecting’ their children, building stronger families and preserving so-called cultural or religious beliefs. However, the act of forcing another person into marriage can never be justified on religious grounds: every major faith condemns the practice of forced marriage.
Some of the key motives given for forced marriage are:
Victims trapped in, or under the threat of, a forced marriage can be very isolated. They may feel there is nobody they can trust to keep this secret, and they have no one to speak to about their situation – some may not be able to speak English.
People who are forced to marry find it very difficult to leave the marriage, and girls may be subjected to repeated rape (sometimes until they become pregnant) and domestic abuse within the marriage. In some cases, victims suffer violence and abuse from extended family members and are forced to do all the household jobs and / or are kept under virtual ‘house arrest’ and not allowed to leave the home without a family escort.
Both male and female victims may feel that running away is their only option. For many leaving the family can be very hard. They may have little experience of life outside the family and worry about losing their support network. Also, leaving their family (or accusing them of a crime, or asking the police or the council for help) may be seen as bringing shame on their ‘honour’ and on the ‘honour of their family’. Those who do leave often live in fear of their own families, who may go to considerable lengths to find them and bring them back home.
Victims of forced marriage, their siblings and other family members are at risk of harm – particularly if they are found to asked for help or are planning to leave the marriage. Victims can face the possibility of ‘honour’-based abuse, rape, kidnap, being held against their will, threats to kill, being abducted overseas and even murder.
The Forced Marriage Unit (FMU) is available to talk to frontline professionals handling cases of forced marriage. It also offers information and advice on the wide range of tools available to tackle forced marriage, including how the law can be used in particular cases, what assistance is available to British victims in different countries and how to approach victims.
All practitioners working with suspected or actual victims of forced marriage should be aware of the “one chance” rule. This is that they may only have one opportunity to speak to a victim and may only have one chance to save their life.
If someone discloses that they are in or at risk of a forced marriage, it should never be dismissed as just a ‘family matter’. For many people, asking for help from an agency is a last resort and so all disclosures of forced marriage must be taken seriously.
Do NOT:
A multi-agency response is vital.
REMEMBER – Younger siblings might be at risk of being forced to marry when they reach a similar age. Appropriate action may be needed to safeguard younger siblings.
The Anti-social Behaviour, Crime and Policing Act 2014 made it a criminal offence in England (Wales and Scotland) to force someone to marry.
This includes:
Forcing someone to marry can result in a prison sentence of up to seven years.
The Marriage and Civil Partnership (Minimum Age) Act 2022 amended the Anti-social Behaviour, Crime and Policing Act 2014 so that that it is an offence to do any acts for the purpose of causing a child to enter into a marriage before their eighteenth birthday (whether or not the conduct amounts to violence, threats, any other form of coercion or deception). 16 to 17-year-olds are no longer able to marry / enter a civil partnership at all. (Previously, under the 2014 Act, forced marriage was only an offence if coercion was used to cause someone to marry, or if the person lacked mental capacity to consent to marry).
Anyone threatened with forced marriage or forced to marry against their will can apply for a Forced Marriage Protection Order (FMPO). Relatives, friends, voluntary workers, police officers and local authority staff can also apply for a FMPO, see Apply for a Forced Marriage Protection Order.
The order is to protect a person from being forced to marry. The details of each order will be specific to the case, for example the court may order someone to hand over the person’s passport or reveal where they are if they cannot be found.
Breaching a FMPO can result in a prison sentence of up to five years.
To protect victims of forced marriage, practitioners may need to share information with other agencies such as the police.
See Tier 1 – Children Safeguarding Data Sharing Agreement (DSA).
Keeping records of forced marriage is important. These may be used in court proceedings.
Staff should keep records of all actions taken, including the reasons why particular actions were taken. There should be a recorded agreement of which agency has agreed to each proposed action, together with the outcomes of the action.
Records should:
Even if forced marriage is not disclosed, a record of the concerns may be useful in the future.
All records should be kept secure, and only accessed by staff directly involved in the case. This is particularly important for victims / potential victims of forced marriage, to make sure no one could pass on confidential information to a victim’s family.
If no further action is to be taken this should be clearly documented, together with the reasons.
RELATED CHAPTERS
RELATED INFORMATION
CONTENTS
The Crown Prosecution Service defines ‘honour’ based abuse as ‘an incident or crime involving violence, threats of violence, intimidation coercion or abuse (including psychological, physical, sexual, financial or emotional abuse) which has or may have been committed to protect or defend the honour of an individual, family and / or community for alleged or perceived breaches of the family and / or community’s code of behaviour.’
It can be a collection of practices, which are used to control behaviour within families or other social groups to protect perceived cultural and religious beliefs and / or so-called ‘honour’. Such violence and abuse can occur when perpetrators perceive that a relative has shamed the family and / or community by breaking their code of ‘honour’.
Victims are usually girls or women, but not exclusively so. Males may also be victims.
HBV is a violation of human rights; it may also be a form of domestic and / or sexual violence. There is no honour or justification for abusing the human rights of others, nor can there be. There is no specific offence of ‘honour’ based abuse. It is an umbrella term to encompass various offences covered by existing legislation.
Behaviour by a child which may be deemed by their family / community as breaching their code of ‘honour’ include:
Males may be targeted either by the family of a female who they are believed to have ‘dishonoured’, in which case both parties may be at risk, or by their own family if they are believed to be homosexual.
HBV is not a crime which is solely perpetrated by men; sometimes female relatives will support, incite or assist. It is also not unusual for younger relatives to be selected to undertake the abuse as a way to protect senior members of the family. Sometimes contract killers can be employed.
Shame may persist for a long time after the incident that was deemed to be dishonourable occurred. This may result in a new partner of a victim, their children, associates or siblings also being at risk.
‘Honour’ based abuse usually involves threats, intimidation and violence in an effort to get the victim to conform to the desired behaviour. These can escalate where deemed to be unsuccessful. On occasion, it may result in murder, which may involve premeditation, family conspiracy and a belief that the victim deserved to die.
In addition to information in Section 2, Common Triggers, incidents that may precede a killing include:
In some circumstances a victim’s immigration status may be used to dissuade them from seeking assistance from authorities.
Victims may suffer in isolation, resulting in depression and attempt suicide.
When dealing with potential victims of ‘honour based abuse’, it is essential that practitioners understand the seriousness of the situation and that immediate, but discreet, action is required (see Referrals and Immediate Protection chapters).
If a child discloses that they, or someone else, are at risk of ‘honour’ based abuse, the professional should:
Immediate steps must be taken as appropriate to ensure the immediate safety of the child. Consideration should be given to any other children in the family and their immediate safety.
Practitioners should ensure that they make a full record of all discussions, with whom these take place and any actions taken including referrals to other agencies. They should also seek support from their manager or safeguarding lead as per their agency protocol
Victims are sometimes persuaded to relocate under false pretences, where the intention may be to either stop them from contacting the authorities or to kill them. If a child is taken abroad, the Foreign and Commonwealth Office may assist in repatriating them back to the UK.
Practitioners should not approach the family or community leaders, share any information with them or attempt any form of mediation.
CONTENTS
This guidance provides information about a range of mechanisms that are available when managing adults, or children and young people, who have been identified as presenting a risk, or potential risk, of harm to children.
Areas covered include:
The Children Act 1989 recognised that the identification and investigation of child abuse, together with the protection and support of victims and their families, requires multi-agency collaboration. This is rightly focused on the child and the supporting parent/carer. As part of that protection, action has been taken, usually by the Police and Children’s Social Care, to prosecute known offenders and/ or control their access to vulnerable children.
This work, while successful in addressing the safety of particular victims, has not always acknowledged the ongoing risk of harm that an individual perpetrator may pose to other children in the future. Nor does it acknowledge that a young person may also be a perpetrator and that the same young person may simultaneously be both suffering, and likely to suffer, harm, and also present a risk of harm to other children and young people.
The terms ‘Schedule One Offender’ and ‘Schedule One Offence’ were used to describe anyone convicted of an offence against a child listed in Schedule One of the Children and Young Person’s Act 1933. However, since the Sex Offences Act 2003, these offences are now known as Schedule 3 (all sex offences) or Schedule 5 (violent offences). A conviction for an offence in the schedules does not trigger any statutory requirement in relation to child protection or safeguarding children issues, and inclusion on the schedule was determined solely by the age of the victim and offence for which the offender was sentenced, and not by an assessment of whether the offender may pose a future risk of harm to children.
The ‘Schedule One Offender’ has been replaced with ‘Risk to children’. This clearly indicates that the person has been identified as presenting a risk, or potential risk, of harm to children.
Practitioners working in this area should use the Sexual Offences Act as a ‘trigger’ for a further assessment, including consideration of previous offences and behaviours, to determine if an offender should be regarded as presenting a continuing risk of harm to children. This allows agencies to focus resources on the correct group of individuals, and not include those who have been identified solely because a child was harmed during the offence, for example, as in the case of a road traffic accident.
An offender who has harmed a child might not continue to present a risk or harm towards that child or other children. Where a child or young person (aged under 18 years) offends against another child, a thorough and specialist assessment should be undertaken to establish the extent to which the young person who has offended continues to pose a risk of harm to other children and young people. They should be alert to the possibility that there may be little or no continuing risk of harm to other children and young people, but never losing sight of taking all possible actions to ensure that children are adequately protected from any future harm. Practitioners should also assess and put in place services to respond to the, often complex, needs of the young person who has offended.
Once an individual has been sentenced and identified as presenting a risk of harm to children, agencies have a responsibility to work collaboratively to monitor and manage the risk of harm to others. Where an offender is given a community sentence, Offender Managers or Youth Justice Support Team (YJST) workers will monitor the individual’s risk of harm to others and their behaviour and liaise with partner agencies as appropriate. The YJST monitors the risk of harm to others and works with other known agencies to manage that risk by holding regular Risk Management Panels (RMPs).
In cases where an offender has been sentenced to a period of custody, prison establishments undertake a similar responsibility and, in addition, notify other agencies prior to any period of release. Similarly, for offenders released on licence into the community who are assessed as potentially presenting a risk of harm to children, consideration will be given to including licence conditions which seek to prevent the offender’s contact with children.
The Sexual Offences Act 2003 introduced offences to deal with those who sexually exploit children and young people. The offences protect children up to the age of 18 and can attract tough penalties. They include:
These are not the only charges that may be brought against those who sexually exploit children or young people. Abusers and coercers often physically, sexually and emotionally abuse these children, and may effectively imprison them. If a child is a victim of serious offences, the most serious charge that the evidence will support should always be used.
See also Multi Agency Public Protection Arrangements chapter.
MAPPA provides a national framework in England and Wales for the assessment and management of the risk of serious harm posed by specified sexual and violent offenders, including offenders (including young people) who are considered to pose a risk, or potential risk, of serious harm to children. The arrangements are statutory. Sections 325–327 of the Criminal Justice Act 2003 require the police, prisons and probation services (the ‘Responsible Authority’) in each area to establish and monitor the arrangements. A number of other agencies – including Children and Adult’s Social Care services, Health, Housing, the YOS, Jobcentre Plus and electronic monitoring providers have a statutory duty to cooperate with the Responsible Authority in this work.
The focus of MAPPA is on specified sexual and violent offenders in, and returning to, the community, and its aims are to:
Offenders eligible for MAPPA are identified and information is gathered/shared about them across relevant agencies. The extent to which they pose a risk of serious harm is assessed and a risk management plan is implemented to protect the public.
Each area has a MAPPA Strategic Management Board (SMB) attended by senior representatives of each of the responsible authority and duty to cooperate agencies, plus two lay advisers. It is the SMB’s role to ensure that the MAPPA are working effectively, and to establish and maintain working relationships with the local Safeguarding Children Partnership.
MAPPA offenders are managed at one of three levels according to the extent of agency involvement needed and the number of different agencies involved:
Exchange of information is essential for effective public protection. The MAPPA guidance details how MAPPA agencies may/should exchange information among themselves to better manage offender It also explains why and how information may be disclosed to those not involved in the MAPPA management of the offenders. The expectation is that information on offenders will be disclosed to others – for example, partners, employers, schools – where this is required to manage the risks posed by the offender.
ViSOR (violent and sex offenders register) is a national database which currently carries details of MAPPA eligible offenders and other potentially dangerous individuals. All three responsible authority agencies (police, probation and prisons) can access the same IT system, thus improving the quality and timeliness of risk assessments and of interventions to prevent offending.
The National Probation Service assess risk of serious harm using the offender management system (OASys), supplemented by additional assessment procedures, depending on the nature of the offending and the specific risks identified. The Youth Justice Board uses AssetPlus for under-18-year-olds. The levels of risk are:
Risk is categorised by reference to the potential subject of the harm. This includes children who may be vulnerable to harm of various kinds, including violent or sexual behaviour, emotional harm or neglect. In this context, MAPPA works closely with local safeguarding children partnerships to ensure the best local joint arrangements can be made for any individual child being considered by either setting.
In most cases, a MAPPA eligible offender will be managed without recourse to MAPPA meetings under the ordinary arrangements applied by the agency or agencies with supervisory responsibility. This will generally be the Police for registered sexual offenders who are not on a licence to Probation, and Probation for violent offenders and those on a licence; but the YJST will lead with young offenders and Mental Health services with those on Hospital Orders. A number of offenders, however, require active multi-agency management and their risk management plans will be formulated and monitored via MAPPA meetings attended by various agencies.
There are three levels of management within the MAPPA framework, based on the level of multi-agency co-operation required to implement the risk management plan effectively:
Offenders will be moved up and down levels as appropriate.
The YJST has a duty to identify cases that meet MAPPA criteria and make appropriate referrals. However, the guidance emphasises that young people should be assessed and managed differently from adults, using age-appropriate assessment tools and always bearing in mind the need to safeguard the welfare of the young offender as well as to protect others from harm. Children’s Social Care should always be represented at MAPPA meetings when a young person is being discussed.
For more information, please see the MAPPA Guidance.
A MARAC is a multi-agency meeting focusing on the safety of high-risk victims of domestic abuse. The identification of high-risk victims has been made possible by a risk identification tool, for use across a wide range of agencies. This has permitted practitioners, both within and outside of the criminal justice system, to identify high-risk victims of domestic abuse. As a result, many more high-risk victims are being identified and, in response, the MARAC has been rolled out across England and Wales.
The MARAC is a process involving all the key statutory and voluntary agencies who might be involved in supporting a victim of domestic abuse. This includes those from the criminal justice system, those supporting children, those from the health service, the local authority, housing, substance misuse and, critically, specialist domestic abuse services, most frequently in the form of an Independent Domestic Violence Adviser (IDVA). The IDVA is a specialist caseworker who receives accredited training to work with high-risk victims of domestic abuse from the point of crisis, and whose focus is very much on the MARAC.
At a typical MARAC meeting, 15 to 20 high-risk cases are discussed in half a day, with a very brief and focused information-sharing process followed by a simple multi-agency action plan being put into place to support the victim and to make links with other public protection procedures, particularly safeguarding children, vulnerable adults and the management of perpetrators.
It is important to understand that the MARAC meeting is part of a wider process which hinges on the early involvement and support from an IDVA and continued specialist case management, both before and after the meeting. The MARAC should combine the best of specialist support together with the co-ordination of the generic agencies whose resources and involvement will be needed to keep victims and their children safe.
Where an offender is being managed at MAPPA Level 2 or Level 3, to avoid duplication of effort and resources, the MAPPA meeting should take the lead over the MARA This is because the MAPPA is a statutory set of arrangements and therefore it takes precedence over the MARAC.
For more information, see Multi Agency Risk Assessment Conference (MARAC) chapter.
Rehabilitation of offenders is the best guarantee of long-term public protection. A range of independently accredited treatment programmes, which have been developed or commissioned by the National Offender Management Service (NOMS), have been tried and tested at a national level. Examples include sex offender treatment programmes, programmes for offenders convicted of internet-related sexual offences, and programmes for perpetrators of domestic abuse.
The Disclosure & Barring Service (DBS) was formed when the Criminal Records Bureau (CRB) and Independent Safeguarding Authority (ISA) merged in 2012. The DBS holds two lists (‘Barred Lists’) of those individuals that are barred from working with (a) children and (b) vulnerable adults. It is responsible for deciding whether an individual should be included on one or both of those lists. Employers and agencies have a duty to refer to the DBS any information about individuals they believe may pose a risk of harm to children or vulnerable adults, ensuring potential threats to vulnerable groups can be identified and dealt with.
It is a criminal offence for barred individuals to seek or take up regulated activity (see definition below) with vulnerable groups, and for employers or agencies to knowingly employ/engage barred staff.
DBS checks (formerly known as CRB checks) provide information about an individual’s criminal record (if appropriate). DBS certificates are required for people applying for jobs which are defined as ‘regulated positions’.
The definition of ‘regulated activity’ for work with children is different to that of work with vulnerable adults. DBS checks sought for individuals undertaking regulated activity also include checks to see if a person is included on any lists held by the DBS of people who are barred from undertaking regulated activity with children and young people.
The revised definition of ‘regulated activity’ which determines eligibility for a DBS check is:
Roles requiring standard or enhanced DBS checks are exempt from the Rehabilitation of Offenders Act 1974, which means that all criminal information is provided about an applicant, even if it would otherwise be regarded as ‘spent’. An enhanced DBS check may also include relevant information the Police have on record, even if it has not resulted in a caution or conviction (for example if allegations have been made and reported to the Police).
Having a criminal conviction does not in itself bar a person from work with children or young people. If a DBS check discloses convictions or relevant information, an employer has to decide whether a person is suitable to be employed in the role concerned.
Organisations should have a policy for the recruitment of ex-offenders (a model version is available) which aims to ensure that all applicants are given fair and transparent consideration for employment.
A referral must be made to the DBS when the following two conditions have both been met:
Condition one – permission is withdrawn for a person to work in regulated activity with children and/or adults either through dismissal or by moving the person to another area of work that is not regulated activity. This includes situations where an employer/volunteer manager would or may have dismissed the person or moved them to other duties, if the person had not resigned, retired or otherwise left their work. For example, a teacher resigns when an allegation of harm to a student is first made. The head teacher establishes that harm did occur, or was at risk of occurring, and decides that they may have dismissed the person had they not left and so makes a referral to the DBS.
Condition two –there is a belief that a person has carried out one of the following:
The DBS will consider whether to bar a person in any of those circumstances. Referrals should be made as soon as possible after the resignation or removal of an individual.
For more information see Disclosure and Barring chapter.
By virtue of the Sexual Offences Act 2003 (Notification Requirements) (England and Wales) Regulations 2012, the Home Office has introduced measures which will extend and strengthen the system of notification requirements placed on registered sex offenders (commonly referred to as the sex offenders’ register).
A person required by the 2003 Act to register with the Police is required by law to:
An offender can only give this notification by attending a Police station prescribed for the purpose by regulations (the regulations will be periodically updated when the addresses of Police stations change).
Offenders should be asked when initially notifying the Police whether there are any addresses (such as any described in the fourth bullet above) which they regularly visit and told that they are required to notify them if they begin to visit other addresses.
Offenders should be reminded when initially notifying the Police of their names and addresses that they are also required to notify any plans to leave the UK for any periods (a separate form [Form 3317] is available for recording this information).
New name and address: For advance notification if the change takes place more than two days before the anticipated date, the Police must be informed. If an advance notification is made and the change has not taken place within three days beginning with the anticipated date, the Police must be informed within six days of the anticipated date.
A person failing to comply with the requirements of the Sexual Offences Act 2003, without reasonable excuse, or who provides the Police with information which is known to be false, could be sent to prison for up to five years.
If an individual is found to have convictions for sexual offences against children and poses a risk of causing serious harm, there is a presumption that this information will be disclosed to the person who is best placed to protect the child or children, where it is necessary to do so for this purpose.
It should be noted that, under the scope of the Disclosure Process, the presumption for disclosure will only exist in cases where the individual has convictions for child sexual offences. However, it is felt that to restrict access to information regarding convicted child sexual offenders would severely limit the effectiveness of the process and ignore significant issues regarding offences committed against children.
It is important that the disclosure of information about previous convictions, for offences which are not child sex offences, is able to continue as it is not the intention of the Disclosure Process to make access to information concerning safeguarding children more restricted.
It is of paramount importance to all involved in delivering this process to ensure that children are being protected from harm. By making a request for disclosure, a parent, guardian or carer will often also be registering their concerns about possible risks to the safety of their child or children. For that reason, it is essential to this process that police forces, Children’s Social Care and local safeguarding children partnerships work closely together to ensure that any possible risks of harm to the child or children are fully assessed and managed.
For further details please see Child Sex Offender Disclosure Scheme chapter.
Notification Orders are intended to ensure that British citizens or residents, as well as foreign nationals, can be made subject to the notification requirements (the Sex Offenders Register) in the UK if they receive convictions or cautions for sexual offences overseas. The provisions also apply to young people who have offended.
Notification Orders are made on application from the Police to a Magistrates’ Court. Therefore, if an offender is identified who has received a conviction or caution for a sexual offence overseas, the case should be referred to the local Police for action.
If a Notification Order is in force, the offender becomes subject to the requirements of the Sex Offenders Registration. For example, a Notification Order could ensure that the notification requirements apply to a British man who, while on holiday in South East Asia, received a caution for a sexual offence on a child.
Any information that an individual has received a conviction or caution for a sexual offence overseas should, where appropriate, be shared with the Police.
Sexual Harm Prevention Orders and Sexual Risk Orders were introduced by the Anti-Social Behaviour, Crime and Policing Act 2014. They replace the previous Sexual Offences Prevention Orders, Risk of Sexual Harm Orders and Foreign Travel Orders which were introduced by the Sexual Offences Act 2003.
Sexual Harm Prevention Orders can be applied to anyone convicted or cautioned of a sexual or violent offence, including where offences are committed overseas.
The Court needs to be satisfied that the order is necessary for protecting the public, or any particular members of the public, from sexual harm, or protecting children from sexual harm from the defendant outside the UK.
Violent Offender Orders (VOOs) are civil preventative orders that came into effect in 2009 (contained in Part 7 of the Criminal Justice and Immigration Act 2008).
VOOs were developed as a tool to help the Police manage those offenders who continue to pose a risk of serious violent harm to the public, even after their release from prison or when their licence has ceased. Although not specifically designed as a tool to protect children, there may be circumstances where VOOs would be an appropriate mechanism to manage an individual who poses a serious risk of harm to children.
VOOs are available on application by a chief officer of Police to a Magistrates’ Court and, if granted, will contain such restrictions, prohibitions or conditions authorised by Section 102 of the Act as the Court considers necessary to protect the public from the risk of serious violent harm caused by the offender. This may include prohibiting their access to certain places, premises, events or people to whom they pose the highest risk.
Breach of any of the prohibitions, restrictions or conditions contained in a VOO without reasonable excuse is a criminal offence, with a maximum punishment of five years’ imprisonment.
RELATED GUIDANCE
Guidance: Learning Disability – Applying All Our Health (gov.uk)
CONTENTS
A learning disability is defined by the Department of Health and Social Care (DHSC) as:
a significantly reduced ability to understand new or complex information, to learn new skills (impaired intelligence), with a reduced ability to cope independently (impaired social functioning), which started before adulthood.
A learning disability is different for everyone. The degree of disability can vary greatly, and learning disabilities can be classified as mild, moderate, severe or profound. In all cases, a learning disability is a lifelong condition and cannot be cured. People who are known to learning disability services are likely to be those with a more significant learning disability.
A learning disability is not a physical disability. It is caused by something which affects the development of the brain either before birth, during birth or in early childhood.
There are a number of conditions and neurological disorders that often involve or cause some type of learning disability, including Down’s syndrome, autism, meningitis, epilepsy or cerebral palsy.
Possible causes of learning disabilities include:
Sometimes the cause of a learning disability remains unknown.
A particular level of IQ cannot be taken as the only defining characteristic of learning disability, and people can have different ability levels across the different components of IQ and other tests. Sometimes it can be difficult to clearly distinguish between those parents who have learning disabilities and those who do not. In the context of parenting, it may be more helpful for practitioners to focus on identifying support needs associated with the impact of the parent’s learning disability, rather than focusing on the definition of learning disability.
A learning disability is different to a learning difficulty, which is a reduced intellectual ability for a specific form of learning and includes conditions such as dyslexia (reading), dyspraxia (affecting physical co-ordination) and attention deficit hyperactivity disorder (ADHD). A person with a learning disability may also have one or more learning difficulties. However, some people who have the label ‘learning disability’ prefer to be called ‘people with learning difficulties’. Practitioners should be sensitive to how people define and describe themselves and use language that parents are comfortable with in their contact with them.
Often those parents with learning disabilities who are in contact with social care services experience a range of difficulties. They may have particularly high levels of need, and present as complex cases where it can be difficult to disentangle the competing concerns.
Compared to people without a learning disability, people with a learning disability tend to experience poorer physical and mental health and reduced life expectancy. They are also:
Parents with learning disabilities may experience a range of needs and difficulties, including a physical or sensory impairment and / or long-term health condition, mental health problems or substance misuse problems and experience domestic abuse.
Some parents with learning disabilities experience significant housing problems, including homelessness, harassment from neighbours and difficulties in maintaining a tenancy.
The same principles of safeguarding and promoting the welfare of children should be applied to the children of parents with learning disabilities as to the children of non-learning disabled parents. However, working with and assessing parents with learning disabilities often requires a specialised response such as different approaches to communication and assessment.
Lack of a formal diagnosis of learning disability may affect a parent’s eligibility for some services, but a parent who presents as having difficulty with, or being unable to, read, write, budget, deal with numbers or abstract concepts, process information, retain and apply it etc. will almost certainly require support to enable them to raise their children safely and well. This is likely to mean allowing more time for a parent with a learning disability to understand what is happening and appropriate and effective communication so they can participate fully in the process.
Effective joint working across all involved agencies is essential, in particular between adult and children’s services where they are supporting parents and children respectively.
Young parents and parents-to-be with learning disabilities may be in transition between children’s and adult services.
Good Practice Guidance on Working with Parents with a Learning Disability (Working Together with Parents Network) identifies five key features of good practice in working with parents with learning disabilities:
Accessible information and communication are crucial to enabling parents with learning disabilities to engage with services and therefore to maximise the chances of children’s needs being met.
Parents should be provided with assistance to enable them to understand what is happening and to express their views. Information may well need to be provided more than once in order for parents to understand what is going on.
Information should be provided in a format which is accessible to them, for example:
Where a child protection plan is drawn up and this involves action to be taken by parents, parents should be fully supported to understand what is required of them and what support is available to help achieve this.
Effective, two-way communication is particularly important in meetings involving a number of different professionals (such as child protection conferences). Information and communication must be accessible, jargon should be avoided and parents should have someone to support them to prepare for the meeting and take part in it, if this is what they want.
Concerns about the ability of parents with learning disabilities to adequately care for and protect their children may arise during antenatal and postnatal care.
Identification of needs should start when a pregnancy is confirmed, with early, appropriately tailored assessments carried out to identify the support which will be needed to look after a new baby. Recognising and addressing support needs at the earliest stages of the parenting experience may help to prevent difficulties for parents which undermine children’s welfare.
Adult learning disability services should take steps to ensure that people with learning disabilities who become parents know about the support available. Such services are well-placed to provide new parents and parents-to-be with accessible information about both universal and specialist services. Children’s social care should also take steps to ensure that adults with learning disabilities who become parents know about the support available to help them with their responsibilities as parents.
It is good practice that, as a general rule, referrals relating to the needs of parents with learning disabilities should be directed to learning disability services. Where there are concerns about children’s welfare a referral should also be made to children’s social care (see Referrals chapter). If a referral is made directly to children’s services, and it then becomes apparent that a parent has a learning disability, a referral should then also be made to adult learning disability services.
Good practice is promoted where there is clear agreement between adult and children’s social care as to the circumstances in which single or joint assessments are required and who should take the lead.
For example:
Assessments involving families affected by parental learning disability should always include specialist input concerning the impact of learning disability. Where there are other difficulties such as mental health and/or physical health problems, domestic abuse or substance misuse, assessments should also include, where appropriate, specialist input on these issues. Assessments should also address the possible vulnerability of the learning disabled parent and their own need to be protected from harm. Parents should be given information – in a format suitable to them – about why an assessment is being carried out, what it will involve, and what might happen as a result.
Parents should be invited to attend child protection conferences and support provided to enable them to participate fully. Careful consideration should be given to ensuring that all communication associated with the child protection conference – from invitation and the conduct of the meeting through to the minutes / notes of the meeting – is accessible to the parent with learning disabilities. Information should be sought, from the parent and / or their advocate, about what communication format is accessible to them.
Good practice will be promoted by:
Key issues for parents with learning disabilities involved in pre-proceedings and court proceedings are their needs for accessible information, support of an independent advocate, enough time to understand what is going on, to be fully involved in any assessments and care planning, and to have the chance to learn and demonstrate improved parenting capacity.
Parents whose children are the subject of section 47 enquiries should always be given early information about independent sources of advice and advocacy. Where possible, independent advocates should have the necessary skills and expertise concerning both learning disability and child protection.
Where section 47 enquiries conclude that a child is not at risk, or not at continuing risk, of significant harm, it will be important that, where appropriate, action is taken – under section 17 of the Children Act 1989 – to prevent future problems arising. It is particularly important to avoid the situation where poor standards of parental care, which do not meet the threshold of significant harm to a child, subsequently deteriorate because of a lack of support provided to the parent. It is also important to provide any necessary support when a child is no longer the subject of a child protection plan, in order to prevent a subsequent deterioration in parental care.
Families affected by parental learning disability are likely to have an ongoing need for support, and where a child protection plan is not considered necessary, another appropriate pathway should be considered.
Some parents with learning disabilities will only need short-term support, such as help with looking after a new baby or learning about child development and childcare tasks. Others, however, will need ongoing support. Most may need support at various points of their family’s life cycle. However, case-law has established that the level of support needed to ensure ‘good enough parenting’ should not be so great as to amount to ‘substitute parenting’.
CONTENTS
Child exploitation, whether sexual or criminal, is child abuse. Children who are exploited face significant harm to their physical, emotional and psychological health and well-being. The effects of trauma experienced through exploitation can be cumulative and can require continued ongoing support to recover from throughout the child’s lifetime and into their adult years. This harm often extends to the wider family and it is important that parents/carers are offered support also.
Agencies across Buckinghamshire are committed to safeguarding children and young people from being sexually and / or criminally exploited, and children are recognised as victims of abuse.
This protocol aligns with local arrangements to safeguard children and sets out a clear pathway by which to ensure all organisations work together to provide the best service possible for children and young people either at risk or exploitation or who have experienced exploitation in Buckinghamshire.
An overarching term of child exploitation will be used throughout this protocol to encompass both criminal and sexual exploitation of children.
This protocol is to support professionals to understand how to access support for children where there are concerns regarding exploitation. This is applicable to external professionals and local authority staff.
It is often the case that children do not perceive themselves to be victims, as they consider they have acted voluntarily or that the exploiter is their friend. Peer on Peer exploitation is commonplace and often unrecognised as exploitation by the victim. The reality is that their behaviour is not voluntary or consenting, and every child in this situation needs to be considered a victim first. The response needs to focus on disruption and engagement.
The nationally agreed definitions for sexual exploitation and criminal exploitation are used across Buckinghamshire:
Child sexual exploitation is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity:
(a) in exchange for something the victim needs or wants, and/or
(b) for the financial advantage or increased status of the perpetrator or facilitator.
The victim may have been sexually exploited even if the sexual activity appears consensual. Child sexual exploitation does not always involve physical contact; it can also occur through the use of technology (taken from Child sexual exploitation: definition and guide for practitioners, Department for Education).
Child criminal exploitation occurs where an individual or group takes advantage of a person under the age of 18 and may coerce, manipulate or deceive a child or young person under that age into any activity.
(a) in exchange for something the victim needs or wants, and/or
(b) for the financial advantage or increased status of the perpetrator or facilitator, and/or
(c) through violence or the threat of violence.
The victim may be exploited even if the activity appears consensual (i.e. moving drugs or the proceeds of drugs from one place to another). Additionally, child criminal exploitation does not always involve physical contact; it can also occur through the use of technology (taken from Serious Violence Strategy, Home Office).
Buckinghamshire Council and partners have committed resources from their agencies to ensure a collective approach is adopted across the county when managing child exploitation.
There is a clear link between children who are missing and exploited;
Children who run away are at significant risk of harm (Hanson & Holmes, 2014). Children who are missing from care, home or education are at greater vulnerability of exploitation (Pona, 2016; Brandon et al. 2020).
For guidance relation to local authority processes please see “ Missing Children Practice Guidance “.
Multi agency practitioners should refer to Children Missing from Care, Home and Education.
The Missing and Exploitation Hub will have varying degrees of involvement in a child(ren)’s case, the rationale for which will be clearly noted on the child’s social care record. All relevant agencies will be made aware of the decision and rationale for the involvement of and specific role the Hub will carry out. The majority of these decisions will be discussed collaboratively within the Multi-Agency Child Exploitation Meeting (MACE).
The Missing and Exploitation Hub is made up of;
Partners work together to;
If you have concerns regarding the exploitation of a child, the following process should to be followed:
If you are unsure if a child is known to Social Care or not, please contact the MASH who will either advise you to complete a referral and CE tool or refer you to the relevant team.
The referral will be screened at the Hub weekly touchdown screening meeting. The referrer may be asked to provide further information if required. This meeting is multi-agency and will determine if threshold is met for discussion in the Multi-Agency Child Exploitation Meeting (MACE).
If threshold is met, the child will then be added to the next Multi-Agency Child Exploitation Meeting (MACE) agenda. MACE meetings are held weekly.
The Hub will contact you and agree any immediate actions that may need to be considered to support the child / family.
The child will then be discussed at MACE where a Multi-Agency Risk Assessment and Plan (Appendix 2) will be considered. This will form part of any statutory plan and does not replace it.
Child Exploitation takes place across local communities and information and intelligence known to statutory and voluntary sector agencies should be used to highlight the threat, establish and reduce risk. An improved picture of intelligence will enable effective action in a greater number of cases of child exploitation, thereby reducing the harm that would otherwise be caused to the young victims and their families.
The MACE meeting provides the framework to allow regular information sharing and action planning to tackle child exploitation across Buckinghamshire.
MACE meetings are co-chaired by Thames Valley Police and the Local Authority and are attended by all relevant partner agencies. Additional representation from other agencies including CAMHS and drug and alcohol services also attend where required.
It is the statutory duty of the local authority to complete a referral to National Referral Mechanism (NRM) for children where it is believed they are the victim of modern-day slavery. For children, this often relates to their trafficking for the purpose of criminal and/or sexual exploitation. The NRM is a framework for identifying and referring potential victims and ensuring they receive the appropriate support. The mechanism supports both children and adults.
It is important to note that children under the age of 18 do not have to consent to being referred to the NRM, and must be first safeguarded and then referred into the NRM process. All children where there is a concern of exploitation should be referred into the NRM.
A referral form is completed online. The Missing and Exploitation Hub will complete an NRM referral form in collaboration with the professional who is working with the child. This is important as the detailed information and knowledge of the issues will be best known to the professional who is working with the child, but the oversight and tracking of referrals sits with the Missing and Exploitation Hub. For more guidance, please see the Home Office website.
Appendix 1 – Child Exploitation Screening Tool (opens in Word)
Appendix 2 – Multi Agency Risk Assessment and Plan (opens in Word)
Appendix 3 – Categories of Risk – Emerging, Significant, Experiencing (opens as a PDF)
Appendix 4 – Appropriate Language in Relation to Child Exploitation (The Children’s Society)
Appendix 5 – Contextualised Safeguarding Staff Guide (opens in Word)
RELEVANT CHAPTER
CONTENTS
A Multi-Agency Risk Assessment Conference (MARAC) is a local, multi-agency victim focused meeting where professionals meet to share information on high risk cases of domestic abuse.
Information about the risks faced by those victims, the actions needed to ensure safety, and the resources available locally are discussed, and used to create a risk management plan involving all agencies. The MARAC is part of a coordinated response to domestic abuse, incorporating representatives from statutory, community and voluntary agencies working with victims, adults experiencing or at risk of abuse or neglect, children and alleged perpetrators.
The MARAC aims to:
Multi-Agency Public Protection Arrangements (MAPPA) may also need to be considered in relation to an offender (see Multi-Agency Public Protection Arrangements chapter).
The MARAC consists of a core group of professionals, representing the statutory and voluntary sectors. The meeting involves contribution and commitment from agencies including police, probation, children’s social care, adult social care (mental health, safeguarding adults), health, education, housing, substance misuse services, and specialist domestic abuse services. Other agencies can attend as required, when they have involvement in a case which is being discussed.
The victim does not attend the meeting, nor the perpetrator or Crown Prosecution Service.
Each victim referred to the MARAC will be allocated an Independent Domestic Violence Adviser (IDVA). The IDVA is a trained specialist whose goal is the safety of domestic abuse victims, focusing on victims at high risk of harm.
The IDVA will attempt to make contact with the referrer and the victim following receipt of a MARAC referral. The IDVA’s job is to be a bridge between victims and the MARAC meeting. The IDVA will try and meet the victim beforehand, or at least talk to them on the phone, and explain how the meeting works, what it can do, and what the options are.
The IDVA will also ask if there is anything the victim would want to be discussed at the meeting.
Referrals can be made (and are encouraged) by any agency who identifies a victim of domestic abuse as being high risk. A DASH Risk Identification Checklist (see Section 5, DASH Checklist) will enable a practitioner to determine the level of risk posed to a victim. Upon meeting the MARAC threshold for high risk, the local MARAC coordinator / administrator should be contacted regarding making a referral. The case will be submitted for the next available MARAC; however in some circumstances, an emergency MARAC meeting may be called.
See Resources for Identifying the Risk Victims Face, DASH Checklist (SafeLives)
The DASH Checklist is for all professionals working with victims of domestic abuse, stalking and honour based abuse.
If a practitioner identifies an individual they are or have been working with, is a victim of domestic abuse, they should complete the tool with the individual, where possible.
The DASH checklist will gather relevant information about the person’s circumstances in order to assess the risk posed to them.
DASH gives a consistent and practical tool to practitioners working with victims of domestic abuse to help them identify those who are at high risk of harm.
It should be noted, however, training is crucial to understanding the DASH Risk Model and it is therefore recommended all staff have training prior to completing the checklist in practice.
RELEVANT INFORMATION
Prevent Duty Guidance (Home Office)
Prevent Duty Training (Home Office)
Channel duty guidance: protecting people susceptible to radicalisation (Home Office)
CONTENTS
Radicalisation is the process through which people come to hold increasingly extreme views or beliefs that support terrorist groups or activities. The most common types of terrorism in the UK are extreme right-wing terrorism and Islamist terrorism. Multi-agency working is key to supporting children who have been radicalised, or who are at risk of radicalisation.
Extremism is defined as the promotion or advancement of an ideology or beliefs based on violence, hatred or intolerance that aims to:
(See Definition of Extremism, gov.uk).
The Prevent Strategy defines extremism as ‘the vocal or active opposition to fundamental British values, including democracy, the rule of law, individual liberty and mutual respect and tolerance of different faiths and beliefs. It also includes calls for the death of members of the armed forces’.
Exposure to extremism can lead to radicalisation and acts of terrorism.
The national counter-terrorism strategy, CONTEST aims to reduce risks of terrorism in the UK and overseas.
Prevent is one of the key parts of CONTEST and aims to stop people becoming terrorists or supporting terrorism; it focuses on early intervention and safeguarding. Prevent is run locally by specialist staff who understand the risks and issues in the local area and know how best to support their communities. Through working together, organisations can identify people who are at risk of radicalisation and provide them with support. The objectives of Prevent are to:
The Prevent duty (Section 26, Counter-Terrorism and Security Act 2015 (CTSA) requires frontline staff working in specific organisations – including education, health, local authorities, police, prisons and probation – to work together to help prevent the risk of people becoming terrorists or supporting terrorism. It helps to make sure that people who are being radicalised are supported in the same way as they are under safeguarding processes.
Children and young people can be exposed to the messages of extremist groups or drawn into violence in different ways, including through family members, by direct contact with extremist groups or, most often, the internet.
Everyone is different and there is no single way of identifying who is at risk of being radicalised into terrorism or supporting terrorism. Signs that a child or young person is being radicalised include them:
Any child can be radicalised but there are some factors which may make a young person more vulnerable. These include them:
These factors will not always lead to radicalisation.
Children are exposed to news and information in lots of different ways and and they may see things which worry them or make them angry. Professionals and parents and carers can help them understand world events and issues in the news by:
Children should be encouraged to consider other viewpoints and to check the facts behind the information that they are looking at. Radicalisers will use conspiracy theories and fake news to draw people in.
As most radicalisation takes place on-line, make sure that devices have the appropriate parental controls in place, and monitor screen time.
Staff working in frontline roles such as education will often be the first to notice if a child displays concerning behaviour. If staff notice behaviours that are a cause for concern, they should consider whether the child is at risk of radicalisation.
There could be many different reasons for the behaviours, not just radicalisation. It is important to understand the context and try to find out why these changes are happening, before reaching conclusions too quickly.
Concerns about radicalisation or extremism should then be checked / shared with the designated safeguarding lead in the organisation. The Prevent lead in the local authority or local police can also be contacted for advice.
Before deciding whether to make a referral to Prevent, it is important to gather as much information as possible, to assess if the child or young person may be on a pathway that could lead to terrorism.
The Department for Education has a dedicated telephone helpline for schools in England who have non-emergency concerns about extremism; which can be contacted by telephoning: 020 7340 7264.
Where there are concerns about radicalisation and extremism, relevant information should be shared with children’s social care (see Referrals chapter). A multi-agency meeting will be held to discuss whether to make a referral to the police for support under Prevent. Referrals to Prevent are made using the Prevent national referral form (see Get help for radicalisation concerns , gov.uk).
Children who could be referred include those who:
REMEMBER – in an emergency, always ring 999.
Once a referral is submitted to the local Prevent team, specialist police staff will assess it. Firstly, they will check if the child is an immediate security threat. The police will then check if there is a risk of radicalisation which means that the child should be discussed at the local Channel panel to see if they are eligible for support through Prevent. This is called a ‘gateway assessment’. Referrals into Channel are made by the Police. If the child needs other support, this should continue unless there is a good reason not to do so.
Channel panels are chaired by the local authority, and attended by multi-agency partners such as police, education professionals, health services, education and children’s social care. They meet to discuss the referral, assess the risk, and, if appropriate, agree a package of support specific to the individual child. Channel is a voluntary process, and the child’s parents and carers must give their consent before a child receives support.
The type of activities that are included in a support package will depend on risk factors, vulnerabilities, and local resources, but might include:
family support contact – activities aimed at supporting family and personal relationships, including formal parenting programmes;
Where Channel is not considered suitable for the child, or their parents or carers do not consent, alternative options will be explored. If the risks cannot be managed in Channel, they will be kept under review by the police.
Where the Channel panel decides to close a case, the child and their parents and carers should be told that their case is being closed and that they will no longer receive support through Channel. They should also be told that ongoing support they are receiving through mainstream services (such as from the NHS, children’s social care, youth justice services, education) will continue.
Identifying a lead professional at the point of the case being closed provides reassurance that they can be brought back for discussion at the panel quickly, should concerns about them re-emerge.
The panel is best placed to identify which agencies will continue to engage with the child after their case with Channel has been closed and to identify a lead professional. Frontline practitioners involved in providing continuing support must be informed that Channel no longer has oversight of the child, and advised on how to re-refer them to Prevent if there are any future concerns.
When sharing personal data about children and young people at risk of radicalisation, it is important to adhere to the requirements of data protection legislation.
Data protection legislation is not intended to prevent the sharing of personal data, but to make sure that it is done lawfully and with appropriate safeguards in place. Under the Data Protection Act and UK GDPR, there must be a legal basis to share personal data. The Prevent Duty is a lawful basis on which to share data.
See also Data Protection and Tier 1 – Children Safeguarding Data Sharing Agreement (DSA)
RELEVANT CHAPTER
Multi Agency Child Exploitation Protocol
RELEVANT INFORMATION
Brook – the young people’s sexual health and well-being charity
Relationships and sex education (RSE) and health education (Department for Education)
Harmful sexual behaviour among children and young people (NICE)
CONTENTS
Instances of underage sexual activity may raise difficult issues for practitioners and need to be handled with sensitivity. Agencies should ensure that all children and young people are given appropriate protection from sexual abuse. It is the responsibility of all professionals to accurately assess any risk of harm, including significant harm, when a child or young person is engaged in sexual activity. This is likely to require a multi-agency approach.
This guidance has also been formed within the context of government policy and therefore supports the principle that young people should be able to access sexual and reproductive health services, including advice about contraception and abortion.
This guidance applies to all sexual relationships. It is designed to assist staff in identifying where sexual relationships may be abusive and whether a child or young person may need the provision of protection or additional services in relation to sexual activity.
Where there are indications of actual or risk of sexual abuse of a child/young person, be it child sexual exploitation, interfamilial abuse or peer-on-peer abuse, also see the Multi Agency Child Exploitation Protocol.
The sexual behaviour of young people is conceptualised as laying on a continuum from mutual exploration to behaviours that are seriously harmful to them or to other children or young people.
Where sexual behaviour is harmful, please refer to the Harmful Sexual Behaviour chapter.
It is essential for agencies to clarify the age of the young person, as this will dictate the course of action to be taken. The Sexual Offences Act 2003 sets out the law in relation to children and young people under the age of 18 years old:
A child under 13 is not legally capable of consenting to sexual activity. Any offence under the Sexual Offences Act 2003 involving a child under 13 is very serious and offences committed by an adult may result in a significant prison sentence.
Where a professional is concerned that a child under 13 is involved in penetrative sex, or other intimate sexual activity, there will always be reasonable cause to suspect that a child, whether a girl or boy, is suffering or is likely to suffer significant harm. Professionals should make a referral to Children’s Social Care (see Referrals chapter).
Children’s Social Care will convene a strategy meeting which should include the professional making the referral as well as representatives from Children’s Social Care, police and other relevant agencies.
Where both parties involved in sexual activity are under 13, then both children should be considered at risk of significant harm. Thames Valley Police will seek to avoid any prosecution of a child where the children are age appropriate and there is no evidence of coercion, threat, force or other power imbalance.
Sexual activity with a child under 16 is also a criminal offence. Where it is consensual it may carry a less serious criminal penalty than under 13 but still attracts a significant prison sentence. It may nevertheless have serious consequences for the welfare of the child.
Consent is always based on choice and is active, not passive. Consent is possible only when there is equal power. Forcing someone to give in is not consent, and going along with something because of wanting to fit in with a group is not consent: ‘If you can’t say “no” comfortably then “yes” has no meaning. If you are unwilling to accept “no” then “yes” has no meaning.’
Consideration should be given in every case of sexual activity involving a child aged 13–15 as to whether there should be a discussion with other agencies and whether a referral should be made to Children’s Social Care. Professionals should use the risk indicators outlined in Section 4 to inform their decision making.
Cases of concern should be discussed with the nominated child protection lead for the agency and subsequently with other agencies if required. Where confidentiality needs to be preserved, the initial consultation can occur without identifying the child directly or indirectly.
Where there is reasonable cause to suspect that significant harm to a child has/might occur, a referral must be made to Children’s Social Care and a strategy discussion held.
Thames Valley Police will seek to avoid any prosecution of a child where the children are age appropriate and there is no evidence of coercion, threat, force or other power imbalance.
Although in most cases sexual activity in itself is not an offence when the young person is over the age of 16, young people aged 16 and 17 are still vulnerable to harm through an abusive sexual relationship and are still offered the protection of child protection procedures.
Professionals should still bear in mind the considerations outlined in this guidance, and in particular should be alert to:
The Sexual Offences Act 2003 makes provision for young people aged under 16 years to be offered confidential professional advice on contraception, condoms, pregnancy and abortion.
It is good practice to follow the Fraser guidelines when discussing personal or sexual matters with a young person under the age of 16 (Lord Fraser, House of Lords ruling in case of Victoria Gillick v West Norfolk and Wisbech Health Authority & Department of Health and Social Security 1985). These hold that sexual health services can be offered without parental consent providing that:
This exception, in statute, covers not only health professionals, but also anyone who acts to protect a child, e.g. teachers, school nurses, careers service personal advisers, youth offending service officers, youth workers, social workers and parents.
In offering such advice, a person is not guilty of aiding, abetting or counselling a sexual offence against a child where they are acting for the purpose of:
Promoting emotional wellbeing includes exploring the part that sexuality plays in the young person’s sense of identity, the emotional implications of entering into a sexual relationship, and the characteristics of healthy relationships. Where appropriate, the needs and concerns of lesbian, gay, bisexual and transgender young people should be recognised and approached sympathetically. Professionals should consider the particular needs of young people with disabilities. Young people who have been abused may need specialist support, for example where sexual feelings are regarded as shameful or where past relationships have been violent or exploitative.
The duty of confidentiality owed to a person under 16 in any setting is the same as that owed to any other person, but the right to confidentiality is not absolute.
Where there is a serious child protection risk to the health, safety or welfare of a young person or others, this outweighs the young person’s right to privacy.
Research and experience have shown repeatedly that keeping children safe from harm requires professionals and others to share information. Such information sharing must be in accordance with legal requirements and the Information Sharing Protocol.
All young people, regardless of gender or sexual orientation, who are believed to be engaged in or planning to be engaged in, sexual activity must have their needs for health education, support and/or protection assessed by the agency/agencies involved.
Consideration should be given to how the young person can access associated assessments and support, and where necessary agencies should signpost or make a referral to appropriate provision.
On each occasion that a young person is seen by an agency, consideration should be given as to whether her/his circumstances have changed or further information has been given which may lead to the need for a referral or re-referral to Children’s Social Care
Where the child is considered to be suffering or likely to suffer significant harm a referral must be made to Children’s Social Care (see Referrals chapter).
In assessing the nature of any particular behaviour, it is essential to look at the facts of the relationship between those involved.
The following considerations must be taken into account when assessing the extent to which the child (or other children) may be suffering, or are at risk of suffering, harm (this list is not exhaustive):
It is important that all decision-making is undertaken with full professional consultation and never taken by one person alone. All discussions must be recorded, giving reasons for action taken and who was involved.
In cases of concern, where sufficient information is known about the sexual partner(s), the agency should check with other agencies, including the police, to establish what, if any, information is known about them. The police should normally share the required information without beginning a full investigation.
Where a serious crime is suspected, advice should be sought from the police at the earliest opportunity to safeguard the child and minimise the risk of any evidence, such as emails or pictures, being destroyed prior to an investigation.
Sexual abuse and exploitation of a child or young person involves an imbalance of power. Any assessment should seek to identify possible power imbalances within a relationship. These can result from differences in size, age, material wealth and/or psychological, social and physical development. In addition, gender, sexuality, race and levels of sexual knowledge can be used to exert power.
Where a power imbalance results in coercion, manipulation and/or bribery and seduction, these pressures can be applied to a young person by one or two individuals, or through peer pressure (i.e. group bullying). Professionals assessing the nature of a child or young person’s relationship need to be aware of the possibility that either or both of these situations can exist for the child or young person, and they should conduct a holistic assessment of the young person’s needs.
There will be an imbalance of power, and the child or young person will not be deemed able to give consent, if the sexual partner is in a position of trust or is a family member, as defined by the Sexual Offences Act 2003, and/or any pre-existing legislation.
Disabled children and young people are more likely to be abused than non-disabled children, and they are especially at risk when they are living away from home (see Children Living Away from Home). They may be particularly vulnerable to coercion due to physical dependency or because a learning disability or a communication difficulty means that it is not easy for them to communicate their wishes to another person. This increases the risk that a sexual relationship may not be consensual.
Professionals should not, however, assume that because a young person has a disability that they are not Fraser competent. Although there is a duty to protect from abuse and exploitation, professionals also need to recognise that disabled children have the right to a full life, including a sexual life.
A child or young person with a disability could be vulnerable to harm from a sexual relationship developed through inclusive activities. This may be in mainstream schools, education colleges, leisure centres and other places where children and young people meet where supervision is at a minimum. Staff need to be alert to the different capabilities of the children and young people they supervise, and assess risks accordingly.
Where professionals in Children’s Social Care have concerns that a relationship may present a risk of harm to an older disabled young person, they should begin work with the Adult Social Care services at an early point in order for there to be a smooth transition from protection under the Children Act 1989 to protection for the young person, from their 18th birthday onwards.
Doctors and other health professionals should consider the following issues when providing advice or treatment to young people on contraception, and sexual and reproductive health.
If a request for contraception is made, doctors and other health professionals should establish rapport and give a young person support and time to make an informed choice. It is important to take account of the capacity of a young person to make informed decisions, even if they are over 16 years old.
If a young person has a learning difficulty or disability, they should be encouraged to speak to an advocate of their choice to help their voice be clearly heard.
When considering a termination of pregnancy, it is particularly important to ensure that the young person has fully understood what is happening.
The following items should be discussed when providing advice or treatment to young people on contraception, and sexual and reproductive health:
Young people need to be able to talk to a trusted adult about sex and relationship issues. Although it is desirable that this person is their parent or carer, this is not always possible. The law allows staff to respect young people’s rights to confidentiality when discussing sex and relationship issues, and a disclosure of under-age sex is not of itself a reason to break confidentiality.
Young people should be made aware that confidentiality might be breached if they or another young person is at risk. In these circumstances staff should consult the young person and endeavour to gain their cooperation to a child protection referral. If that is not possible, they should be advised that their confidentiality would be breached.
Staff in schools should consider the need to establish links with colleagues in health to facilitate the delivery of advice/support and guidance on matters of sexual health.
While police and Children’s Social Care staff may provide advice and guidance to a young person involved in under-age sexual activity, both agencies have specific responsibilities with regard to criminal activities.
Children’s Social Care staff should inform police of actual and suspected criminal offences at the earliest possible opportunity in order to consider jointly how to proceed in the best interests of the child. Any decisions not to do so must be made at a senior level and recorded on the child’s file.
Guidance for Children’s Social Care staff indicates that, as Working Together is issued under Section 7 of the Local Authority Social Services Act 1970, a decision not to inform the police where an offence has been committed against a child should only be made where ‘exceptional circumstances justify a variation’ (LASSL (2004) 21). This is likely to be where the sexual relationship is considered consensual and not abusive, and may be most relevant in respect of children in care where children’s social care is also acting as the ‘corporate parent’ for the child.
In these circumstances it may be more important that the child receives appropriate advice regarding sexual health and contraception. This may be difficult if the young person is concerned that the police will be involved. Such a decision should always be made following consultation with line managers and should be recorded.
The police will proportionately investigate all criminal activities and make appropriate decisions in relation to the need for prosecution or not. Such decisions should always be made following consultation with line managers and should be recorded.
The priority for the police is the identification and investigation of under-age sexual activity where the relationship is abusive, either by being intra-familial in nature, or where there is a significant age/power gap between the parties involved.
Where young people of a similar age are involved in consensual sexual activity, or in other sensitive cases, the police role may be confined to the undertaking of information checks only. In such cases the police will not become directly involved in an investigation unless enquiries by the police or other agencies indicate the relationship is in fact abusive.
Both police and Children’s Social Care staff together may decide that there is no need for prosecution, but young people should be advised that their confidentiality cannot be maintained if staff from these agencies are involved.
Decisions to share information with parents and carers should be taken using professional judgement, consideration of the Fraser guidelines and in consultation with the child protection procedures. Decisions should be based on the child’s age, maturity and ability to appreciate what is involved in terms of the implications and risks to themselves. This should be coupled with the parents’ and carers’ ability and commitment to protect the young person.
Given the responsibility that parents have for the conduct and welfare of their children, professionals should encourage the young person, at all points, to share information with their parents and carers wherever safe to do so.
Those working directly with young people should give consideration to the role they may have in facilitating information sharing with parents/carers, in a planned way, in partnership with the young person.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
January 2026: A link to the Multi-agency Practice Principles for Responding to Child Exploitation and Extra-familial harm has been added. See above.
Some children will experience abuse and exploitation outside the home. This is often referred to as ‘extra-familial harm’. Harm can occur in a range of extra-familial contexts, including school and other educational settings, peer groups, or within community/public spaces, and/or online. Children may experience this type of harm from other children and/or from adults. Forms of extra-familial harm include exploitation by criminal and organised crime groups and individuals (such as county lines and financial exploitation), serious violence, modern slavery and trafficking, online harm, sexual exploitation, teenage relationship abuse, and the influences of extremism which could lead to radicalisation. Children of all ages can experience extra-familial harm.
Where there are concerns that a child is experiencing extra-familial harm, practitioners should consider all the child’s needs and vulnerabilities. Some children will have vulnerabilities that can be exploited by others and will require support appropriate to their needs to minimise the potential for exploitation. All children, including those who may be causing harm to others, should receive a safeguarding response first, and practitioners should work with them to understand their experiences and what will reduce the likelihood of harm to themselves and others.
Where children may be experiencing extra-familial harm, children’s social care assessments should determine whether a child is in need under section 17 of the Children Act 1989 or whether to make enquires under section 47 of the same Act, following concerns that the child is suffering or likely to suffer significant harm. A good assessment should:
See also Assessments procedure.
Where there are concerns that more than one child may be experiencing harm in an extra-familial context, practitioners should consider the individual needs of each child as well as work with the group. The children in the group may or may not already be known to local authority children’s social care. Working with the whole group enables practitioners to build an understanding of the dynamics between those within the group and the extra-familial context.
Practitioners will need to build an understanding of the context in which the harm is occurring and draw on relevant knowledge and information from the children and wider partners in order to decide on the most appropriate interventions. Practitioners should consider the influence of groups or individuals perpetrating harm, including where this takes place online, and identify patterns of harm, risk and protective factors in these contexts. This may include working across safeguarding and community safety partnerships to agree a plan for keeping children safe.
Key decisions should be recorded and communicated to both the child and their parents or carers, so that everyone understands the action that has, or will be, taken to safeguard and promote their welfare. It is important that all partners are clear how actions contribute to safeguarding and promoting the welfare of the child.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
Mother and baby units (MBUs) are discrete specialist accommodation, within some prisons, for female prisoners with children up to age of 18 months or above, where appropriate. Governors or Directors of prisons which have MBUs have a duty of care to the child.
When a woman applies for a place on a mother and baby unit (MBU), a referral for assessment must be requested by the prison from children’s social care in the mother’s home local authority at the earliest opportunity and must include information on MBU provision and policy. Any assessment should set out the needs of the child in relation to the mother’s application to be placed on an MBU.
The assessment should consider:
The lead practitioner responsible for the assessment should attend the MBU Admissions Board to represent the best interests of the child. When placed in an MBU, the mother retains full parental responsibility for the day-to-day care of the child, and the local authority in which the prison is located is responsible for safeguarding and promoting the welfare of the child.
The prison should actively engage children’s social care to ensure the relevant input into processes and individual cases. Practitioners should be provided with information on the purpose, facilities and support available on the MBU. Opportunities for practitioners to visit the MBU should be offered and encouraged.
Prisons must consult children’s social care on all MBU Board decisions, including decisions relating to a change in placement, and any other matters relevant to promoting the welfare and safeguarding a child.
RELATED INFORMATION
Working Together to Safeguard Children (Department for Education)
CONTENTS
A crucial role of children’s social care is to provide help and support to children with disabilities and their families. When undertaking an assessment of a child with disabilities, practitioners should recognise the additional pressures caring for a child with disabilities can place on the family, and the distinct challenges they may have had to negotiate as a result of their child’s disability.
The assessment process should focus on the needs of the child and family, be strengths-based, and gather information to inform decisions on the help needed to:
The local authority must also consider whether it is necessary to provide support under section 2 of the Chronically Sick and Disabled Persons Act 1970. Where a local authority is satisfied that the identified services and assistance can be provided under section 2 of the Act, and it is necessary in order to meet the needs of a child with disabilities, it must arrange to provide that support.
Where a local authority is assessing the needs of a child with disabilities, a carer of that child may also require the local authority to undertake an assessment of their ability to provide, or to continue to provide, care for the child, under section 1 of the Carers (Recognition and Services) Act 1995. The local authority must take account of the results of any such assessment when deciding whether to provide services to the child.
If a local authority considers that a parent carer of a child with disabilities may have support needs, it must carry out an assessment under section 17ZD of the Children Act 1989. The local authority must also carry out such an assessment if a parent carer requests one. Such an assessment must consider whether it is appropriate for the parent carer to provide, or continue to provide, care for the child. The assessment should also take account of parent carer’s needs and wishes, and the specific needs and circumstances of the child resulting from their disability. Parent carers have the right to request an assessment under section 17ZD of the Children Act 1989, including where a child is not otherwise known to children’s social care. Local authorities must ensure they have a process to facilitate these assessments if requested.
In line with the commitments made in the Special Educational Needs and Alternative Provision Improvement Plan, local authorities are encouraged to implement the role of Designated Social Care Officer (DSCO) in each local area. The DSCO role is intended to provide the capacity and expertise to improve the links between social care services and the SEND system. Similar to the Designated Clinical Officer (DCO) or Designated Medical Officer (DMO) role in health, the DSCO role will support both operational input (such as the contributions from care to education, health and care assessments) and more strategic planning functions (such as the commissioning of care services such as short breaks) for children with special educational needs and disabilities.
RELEVANT CHAPTERS
Allegations against People Working with Children / In Positions of Trust
See also BSCP Safer Recruitment Toolkit and Better Hiring Toolkit (Disclosure and Barring Service and partners)
CONTENTS
Safer recruitment, induction and supervision of staff are essential to the safeguarding of children. All organisations should have generic recruitment policies and procedures in place. This chapter provides additional, specific guidance in relation to safer recruitment practices at each step of the generic recruitment process, which aims to prevent unsuitable persons from working with children, either as a paid member of staff or volunteer whether they are permanent, temporary or agency staff or recruited from abroad. In addition, it applies to staff / volunteers who are seen by children as trustworthy and / or have access to confidential information. This may include administrative staff, caretakers, and maintenance workers for example.
Commissioners should ensure the principles of safer recruitment and employment are included in service level agreements or contracts drawn up between them and service providers. A service level agreement or contract should also contain the service’s safeguarding statement (see Section 2.2 Safeguarding policies).
All organisations should have a statement about their commitment to the prevention of abuse and neglect and promoting the wellbeing of children and adults with care and support needs, to which it is expected all staff and volunteers will abide by and embed in their daily practice. This should include that robust recruitment and selection procedures are in place to identify and deter people who might abuse or neglect children or who are otherwise unsuitable for employment / volunteering. The statement should be included in recruitment material such as job adverts, candidate information packs and person specifications.
Organisations should publish a safeguarding policy for staff which reflects these Safeguarding Children Policies and Procedures, and sets out the responsibilities of all staff to operate within it. It should include information on:
Organisations should also produce guidance outlining the rights of staff and how employers will respond where abuse is alleged against them within either a criminal or disciplinary context (see Allegations Against People Working with Children/In Positions of Trust chapter).
The advertisement should include the organisation’s policy statement (see 2.1, Commitment to safeguarding). It should also include reference to the requirement for the successful applicant to undertake a Disclosure and Barring Service check, as appropriate.
The job description (JD) should be specific about extent of contact and levels of responsibility the post holder will have for children, including prevention of abuse or neglect at operational and / or strategic levels.
The person specification (PS) should include any other requirements the post holder will need in order to perform the role in relation to working with children, including experience specific to the post, for example working with children with learning disabilities. The successful candidate should be able to demonstrate such required competencies and qualities.
The information pack should also highlight that a robust selection process is in place, and include reference to the organisation’s safeguarding policy. It should state proof of identity will be required, as well as a Disclosure and Barring Service check, as appropriate.
Employers should only use their own application forms for applicants. It is not good practice to accept curriculum vitae (CV) instead of an application form as this may only contain information the person wants to present rather than all the information the organisation requires to enable shortlisting. The applicant form should again include reference to the organisation’s commitment to safeguarding children.
Application forms should be scrutinised for any unexplained gaps in employment history, or other potential concerns in relation to safeguarding. References should be sought on all candidates who are shortlisted for interview.
Where an applicant is not currently working with children, but has done so previously, a reference should also be obtained from the last such employer, in addition to the current / most recent employer. This should include confirmation of the reason why the applicant left the post.
The referee should state:
The interview should assess the merits of the candidate against the JD and PS, and explore their suitability to work with children.
The panel should state to each candidate there will be a requirement to complete an application for a Disclosure and Barring Service check, confirm their identity and receive satisfactory references.
One member of the panel should be trained in safer recruitment practice.
The panel should explore with the candidate:
Children can make very valuable contributions as part of recruitment of new staff positions. Their participation should be built into the process at all levels, from administration posts to senior positions. Their roles should be clarified, so they understand how their views will be considered and what weighting they will be given.
Offers of appointment will be conditional on receipt of satisfactory checks and references.
In the following circumstances the applicant should be reported to the police:
See Disclosure and Barring chapter
The level of Disclosure and Barring Service check requested should reflect the nature of the post and degree of contact with children or with confidential information.
Types of Disclosure and Barring Service (DBS) checks are as follows:
For guidance on which type of DBS check is appropriate for the role being advertised, please see the DBS website.
A record should be kept of the date when the disclosure was obtained, by whom, level of disclosure and unique reference number.
In ‘signing off’ or agreeing a personal budget a local authority may add conditions such as a DBS check as part of its risk assessment of safeguarding in specific cases. The local authority may also require personal budget holders using direct payments to tell them who they employ.
The same checks should be made on overseas staff as for all other staff, however the Disclosure and Barring Service cannot access criminal records held overseas, so a DBS check may not provide a complete view of an applicant’s criminal record if they have lived outside the UK.
Where an applicant has worked or been resident overseas for 12 months or more (whether continuously or in total) in the last 10 years while aged 18 or over, the employer should obtain a check of the applicant’s criminal record from the relevant authority in that country as well as information about their conduct. It should be noted that not all overseas organisations / countries are able to provide such information. The application process for criminal records checks or ‘Certificates of Good Character’ for someone from overseas varies between different countries. For further information, see Criminal Records Checks for Overseas Applicants (Home Office).
Written confirmation should be provided by the agency that the necessary checks have been undertaken and are satisfactory.
In relation to each candidate who is appointed, records should be made of:
On starting in a new post, the member of staff should be given written information in relation to:
Regular supervision sessions should take place as per the organisation’s policies and procedures, as should annual staff reviews. Both processes aide both the organisation and member of staff by ensuring:
The DBS also provides an online Update Service, to which staff or volunteers can subscribe and renew annually for a small fee (this may be free for volunteers). This helps them keep their DBS certificate up to date, so it can be taken with them from one job to another, as long as they remain within the same workforce (children, for example).
RELEVANT CHAPTERS
Safer Recruitment and Employment
Allegations against those Working with Children / People in Positions of Trust
RELEVANT INFORMATION
Disclosure and Barring Service
Disclosure and Barring Service: Guidance for Children’s Social Care Providers and Managers (Ofsted)
Check Someone’s Criminal Record as an Employer (UK Government)
CONTENTS
Employers need to ensure, to the best of their ability, that the people who they employ – as paid staff, volunteers or contractors – are committed to providing good quality care and support to children and families.
Carrying out robust criminal records checks is part of a number of safer recruitment measures which can help to prevent unsuitable people being employed to work with children.
Thorough recruitment processes, and ongoing training, supervision and appraisal programmes are also key to ensuring safer working practices.
The Disclosure and Barring Service (DBS) helps employers make safer recruitment decisions. It is responsible for:
The minimum age at which someone can be asked to apply for a criminal record check from the DBS is 16 years old.
Before an organisation requires a standard or enhanced check through the Disclosure and Barring Service, it is legally responsible for ensuring the job is eligible (see Eligibility, DBS).
The DBS eligibility tool can be used to determine what type of check a particular role could be eligible for: Find out which DBS Check is Right for your Employee.
There are four different types of checks:
Under the Rehabilitation of Offenders Act 1974, many convictions or cautions become ‘spent’ after a specified length of time, known as the ‘rehabilitation period’. This means that once the rehabilitation period has been completed, they will not show on a basic DBS check. Applicants do not need to tell anyone about a spent conviction unless they are applying for a job where a standard, enhanced, or enhanced with barred lists DBS check is needed.
The DBS provides an online Update Service, to which staff or volunteers can subscribe and renew annually for a small fee (this may be free for volunteers). This helps them keep their DBS certificate up to date, so it can be taken with them from one job to another, as long as they remain within the same workforce unless:
Employers can do immediate online checks of people who have registered with the Update Service. The Update Service is for standard and enhanced DBS checks only (see Section 3.1, Types of checks).
A new DBS check will only be required if the update service check indicates there has been a change in the person’s status, due to new information added.
See also Disclosing your criminal record (Ministry of Justice)
Staff, including volunteers, who apply for posts that require a standard, enhanced or enhanced with barred lists DBS check must legally disclose a criminal conviction if the employer asks- even it if is ‘spent’. It is vital, therefore, that this is a standard question on application forms for such posts. If the employer asks the applicant and they do not disclose their conviction/s, the employer could later revoke the job offer or the employee could be dismissed if they have already commenced their employment. They could face a further conviction if they are found to have worked, or attempted to work, whilst barred from such positions (see Section 4, Barred Lists and Duty to Refer).
If an applicant discloses previous convictions, they can still be considered for the post They should be asked to meet with members of the interviewing panel to discuss the offences (with dates) for which they were convicted and any other relevant information that will help the panel make a decision their suitability for the post.
There are two barred lists maintained by the DBS, those who are:
A person who is barred from working with children or adults commits a criminal offence if they work, volunteer or try to work or volunteer with the group from which they have been barred.
An organisation which knows they are employing someone who is barred from working with that particular group, will also be committing a criminal offence.
Legally an organisation must make a referral to the Disclosure and Barring Service if two conditions are met:
See the DBS Barring Referral Flowchart
Regulated activity is work which involves close and unsupervised contact with children and which cannot be undertaken by a person who is on the DBS Barred List. It includes:
There is a duty on a ‘regulated activity provider’ to find out whether a person is barred before allowing that person to carry out regulated activity tasks in their work.
It is a criminal offence for a person on one of the barred lists to take part in regulated activity, or for an employer / voluntary organisation knowingly to employ a barred person in a regulated activity role.
For more information, see Regulated Activity with Children (DBS)
To follow.
Information on the the process for managing allegations and contact details for the Local Authority Designated Officer (LADO) can be found on the Buckinghamshire Safeguarding Children Partnership website.
RELATED INFORMATION
Working Together to Safeguard Children, Chapter 6 (Department for Education)
CONTENTS
The death of any child is a tragedy. Every parent has a right to have such an event properly investigated. Many sudden child deaths are the result of natural causes. However, all child deaths need to be appropriately investigated to exclude homicide, to reassure the family and ensure that future children are protected, and to satisfy wider public concerns.
This guideline is provided to support multi-agency staff working within Buckinghamshire following the death of a child or young person. It aims to give an overview of the whole Child Death Review Process and to offer specific operational guidance on the management of child deaths.
A child is defined as anyone who has not yet reached their 18th birthday. ‘Children’ therefore means ‘children and young people’ throughout. The fact that a child has reached 16 years of age, is living independently or is in further education, is a member of the armed forces, is in hospital, in prison or in a Young Offenders’ Institution, does not change his or her status or entitlement to services or protection under the Children Act 1989.
This protocol does not apply to stillbirths, unless the stillbirth occurs within the community, without any medical interventions, and a doctor is not able to issue a death certificate.
This document provides the framework for a comprehensive and sensitive enquiry aimed at establishing the cause of, and factors contributing to, all deaths in all children under 18 years, with particular attention to the management of sudden, unexpected deaths. This guidance is not intended to be prescriptive, but endeavours to provide advice to practitioners who are confronted with these tragic circumstances.
Professionals need to strike a balance between the sensitivities of handling the bereaved parents and securing and preserving evidence, which may aid them in arriving at an understanding of why a child has died.
When dealing with an unexpected or unexplained child death, all agencies need to follow five common, equally important, principles:
The purposes of the Child Death Review process are:
There are two inter-related processes for reviewing child deaths:
(Click on the image to increase size)
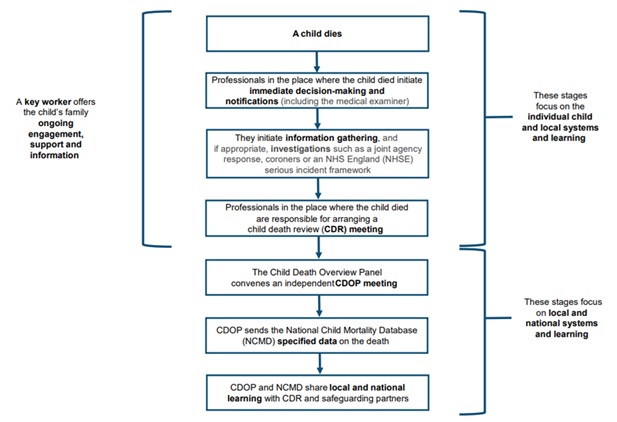
Several decisions need to be made by professionals in the hours immediately following the death of a child. These include:
A number of notifications should also be made: to the child’s GP and other professionals; to the Child Health Information System; and the relevant Child Death Review partners (as a minimum police and social care) and the Child Death Overview Panel (CDOP).
Following the notification of a child death, a number of investigations may then follow. These include:
Post-mortem examinations may be required in some cases. Which investigations are necessary will vary depending on the circumstances of the individual case. They may run in parallel, and timeframes will vary greatly from case to case.
Although investigations following the death of a child will vary, every child’s death should be discussed at a Child Death Review Meeting. This is the multi-professional meeting attended by professionals directly involved in the care of that child during life and those involved in the investigation after death.
The nature of this meeting will vary according to the circumstances of the child’s death and the practitioners involved.
Child Death Overview Panels (CDOP’s) are responsible for reviewing information on all child deaths. Information from the above investigations is fed into the CDOP for final review. In Buckinghamshire there are two CDOP’s. One operates in Milton Keynes and the other one is a joint Panel between Buckinghamshire and Oxfordshire (as per requirements for the minimum numbers of cases). The CDOP for Buckinghamshire contains representation from the Integrated Care Board (ICB), Children’s Social Care, Thames Valley Police, the Buckinghamshire Coroner’s Office, Public Health, South Central Ambulance Service, Midwifery and Education. In addition the Paediatric Liaison Nurse and Designated Doctor for Child Death Reviews in Buckinghamshire also attend.
Child death review processes have been mandatory since April 2008.
Supporting and engaging the family who have lost a child is of prime importance throughout the whole child death review process. Recognizing the complexity of the process, and the different emotional responses that bereavement can bring, families should be given a single, named point of contact, i.e. the “key worker”, for information on the processes following their child’s death, and who can signpost them to sources of support.
Multiagency discussion and planning are required within the first few hours following notification of a child’s death. Necessary discussions may be face-to-face or by telephone and should engage the following professionals:
Information about the circumstances of the child’s death and medical and social background should be sought to aid with the following:
The outcome of these discussions should also be fed back to the family.
A post-mortem examination is sometimes required as part of a coronial investigation. If a coroner requires a post-mortem examination parental consent is not required and parents cannot refuse the examination.
In cases where a death certificate can be issued a hospital post-mortem examination (PM) may still provide important information as to why a child has died. It is therefore important to explore the issue with the family at the time of death, even in cases where the coroner does not require a PM.
This should be completed electronically filling out a notification form within 24 hours of the death (or next working day). This is done via the Oxfordshire Buckinghamshire eCDOP website login using the “Submit Notification form A”:
For all deaths essential information regarding demographics, circumstances of death and background medical history should be submitted to CDOP via the reporting form (previously Form B).
The following people should also be notified within 24 hours (or the next working day) of the child’s death:
The nature of the investigation(s) varies with individual circumstances. They may include:
For all deaths essential information regarding demographics, circumstances of death and background medical history should be submitted to CDOP via the Notification Reporting Form A process. Oxfordshire/Buckinghamshire eCDOP website log-in.
The coroner’s office must be informed of all ‘unexpected’ deaths via 01494 475505 (call Thames Valley Police on 101 out of hours). Once the death has been declared, the coroner assumes immediate responsibility for the body. Samples may be taken post-mortem as outlined in the BHT Policy.
Anyone can refer a death to the coroner for investigation. Reasons for referral are as follows:
They may order a post-mortem (PM) examination, if necessary. Following the PM, the body of the child is usually promptly released back to their family for the death to be registered and funeral arrangements to be made. Release may however be later if organs or tissues have been taken for analysis, or if a second independent post-mortem examination is required.
Not all deaths reported to the coroner proceed to inquest although most unexplained deaths of children do. The inquest aims to determine the identity of the person that died and how, when and where they came by their death. The coroner will examine the evidence and, commonly without a jury, record the answers to the questions listed on a public document called the Record of Inquest. The details of the coroner’s findings are forwarded to the local registrar.
All agencies holding pertinent information are under a duty to disclose such information.
The family should be informed early on of the coroner’s involvement, and the need for and timing of a post-mortem examination, their right to be represented at the examination should they so wish, whether an investigation or inquest has been opened so that they may attend the inquest opening and the dates of any investigation reviews, pre-inquest reviews and the inquest itself.
Once the jurisdiction of the coroner is engaged, the coroner’s officer is the main point of contact with the family for matters relating to the coronial process.
All deceased children that meet the criteria for a JAR should be transferred to the nearest appropriate Emergency Department (ED) to enable the JAR to be triggered.
A Joint Agency Response should be triggered if a child’s death:
In any of these circumstances, the on-call paediatrician at Stoke Mandeville Hospital, (pager 593), police investigator, and duty social worker should be contacted immediately to initiate the Joint Agency Response.
A Joint Agency Response should also be triggered if such children are brought to hospital near death, are successfully resuscitated, but are expected to die in the following days. This enables an accurate history of events to be taken and, if necessary, a ‘scene of collapse’ visit to occur. Appropriate clinical investigations should also be performed in such cases.
A lead health professional should be assigned. This will usually be the on-call paediatrician. This person will ensure that all health responses are implemented and be responsible for on-going liaison with the police and other agencies.
Flowchart setting out the sequence of events that should unfold in a Joint Agency Response. A Joint Agency Response can be divided into three separate phases:
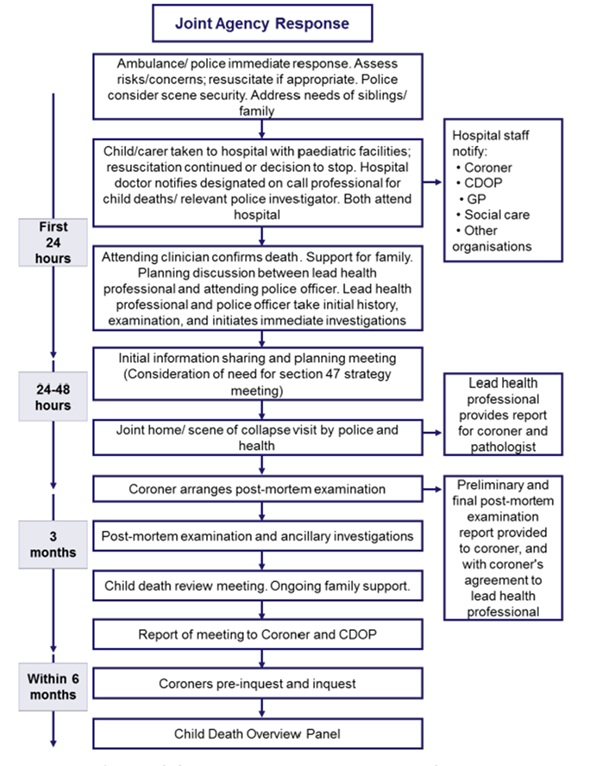
At each stage in the process, explicit consideration must be given as to whether child abuse / neglect may have been a contributory factor.
Immediate response (within a few hours)
Normally following an unexpected death, a child will be transferred by the ambulance service to Stoke Mandeville Hospital. The emergency providers attending the scene should assess the child and, unless it is clearly inappropriate, should attempt resuscitation and transfer the child and family to hospital. The child should never be taken straight to the mortuary unless directed by the police in consultation with the coroner. In such cases the police are responsible for notifying the consultant paediatrician on-call.
On arrival at hospital, a member of the nursing staff will be allocated to the family. On arrival at the A&E department the consultant paediatrician and/or senior doctor in A&E should be informed. Immediate responsibility for informing and providing appropriate care and support of the family rests with the on-call paediatric team. Resuscitation should continue as appropriate and any decision to stop will be made by an experienced medical practitioner with input from other members of the resuscitation team and in consultation with the family. As soon as practicable after arrival at a hospital, the child should be examined by the consultant paediatrician or delegated senior paediatrician on-call.
When the child is pronounced dead, the paediatric or A&E consultant or delegated senior clinician should inform the parents, having first reviewed all the available information. S/he/they should explain future police and coronial involvement, including the coroner’s authority to order a post-mortem examination. This may involve taking tissue blocks and slides to ascertain the cause of death.
Initial bereavement support will be provided by hospital staff. This is a difficult time for everyone. The time spent with the family may be brief, but actions will greatly influence how the family deals with the bereavement for a long time afterwards. Remember that families are in the first stages of grief. They may be shocked, numb, withdrawn, angry or hysterical. Every effort should be made to conduct discussions in a private and sympathetic environment away from interruptions.
Communication should be clear, sensitive and honest. Parents should be treated with compassion, respect and dignity.
Where parents do not understand and/or speak English well, an independent interpreter should be called – one can be arranged via switchboard. The interpreter should not normally be a family member. However, urgent information about the child could be sought from a family member whilst awaiting an interpreter to arrive.
Staff caring for families after a child’s death should be offered support through a formal debrief system and counselling via the Workplace Health Department, as appropriate.
Ongoing bereavement care is available from a range of agencies. Further details can be found in Appendix 2.
For lactating mothers please consider liaising with the medical team involved for the purposes of possible prescription to supress lactation.
Most of the medical and social history will be obtained during the initial discussion with the parents in the A&E Department. This is supplemented by information obtained at the home visit. All professionals should record history and background information given by parents/carers in as much detail as possible.
It is crucial that under no circumstances should professionals challenge or make comment on the history given by a parent/carer – if challenged or a comment is made parents/carers may form the impression that their account is not believed and may subsequently change their story. This could hinder any police investigation.
If there are other children, enquire about their whereabouts and who is caring for them. A surviving twin should automatically be offered admission for monitoring and investigation.
A Joint Agency Response meeting for children who normally reside within Bucks and who die in Bucks will be coordinated by the on-call paediatric team at Stoke Mandeville Hospital. These deaths should be notified to the on-call paediatrician by telephone. The consultant paediatrician on-call is responsible for instigating the Joint Agency Response and must ensure that police, social care and other appropriate agencies have been notified.
For children who reside in Buckinghamshire who have died at the John Radcliffe hospital in Oxford the paediatric team at Stoke Mandeville Hospital will coordinate the Joint Agency Response. These deaths should be notified in the first instance to the on-call paediatrician at Stoke Mandeville Hospital, who will then liaise with the Designated Doctor for Child Death Reviews (or in their absence the Named Doctor for Safeguarding).
For children who reside in Buckinghamshire who have died at a tertiary centre other than Oxford (e.g. GOSH, Birmingham etc), the initial response should be dealt with by the team within that centre. The paediatricians at Stoke Mandeville do not coordinate the investigation but may be called upon to attend meetings (e.g. case discussion/case review meetings) at the tertiary centre. They may also be called upon to submit a “Reporting form B” about the child to the Bucks CDOP.
For children dying within Buckinghamshire who normally reside elsewhere, the paediatric team will coordinate a Joint Agency Response as for a Buckinghamshire child, submitting information to the child’s local CDOP as appropriate. The exception to this would be a child from Oxfordshire. These cases should be notified to the SUDIC Paediatrician at the John Radcliffe or to the CDOP administrator for Oxfordshire (both available via the John Radcliffe Switchboard).
If there is any uncertainty about whether a Joint Agency Response is required, or who should convene one, it is imperative that it be discussed with the SUDIC paediatrician as a matter of urgency. If the SUDIC paediatrician is on leave then this should be discussed with the Named Doctor for Child Protection.
Early contact and discussion between key agencies is essential. Discussion should focus on whether the death may have been caused by abuse or neglect. In such cases the safety of siblings must be considered. Consideration should be given to securing the scene where the child died. Discussion about the need for a home/scene visit should take place early on between the police officer and the on-call paediatrician, enabling the prompt recovery of evidence that otherwise could be lost. A home visit will almost always be required in deaths under the age of 2 years. Paediatricians do not currently participate in home visits. The photographs from home visits can be shared and discussed by the team during the Joint Agency Response meeting.
Contact with police and social work should be clearly documented in the notes. No professional should assume they have been contacted. Repeated calls are better than none at all. If the death is suspicious or significant concerns are raised at any stage about the possibility of abuse or neglect, a decision will be taken for the police to become the lead agency and take primacy in the investigation.
On receiving notification of an unexpected child death, a senior police officer will be designated as the Senior Investigating Officer (SIO). It is important to stress to the family that the involvement of the police is routine and does not assume suspicion. However, staff need to be aware that on occasions, in suspicious circumstances, the early arrest of the parents/carers may be essential to secure and preserve evidence as part of an investigation.
The home or scene visit
For all children less than 2 years of age who have died suddenly and unexpectedly, a home visit should be undertaken within 24 hours (usually the same day). For older children the need for a home visit should be discussed between the police and the paediatric team. The home visit is usually conducted by the police. The home visit provides an opportunity to take a more careful history, to inspect the death scene and to try and alleviate some of the family’s concerns.
The purposes of the home or scene visit are to:
Where the location of the death is different to the home address of the child, an additional visit to the home address may be arranged if deemed necessary. Consideration should be given as to which professionals should attend the visit. Normally this will be the senior investigating officer. Where possible a member of the primary care team, or some other professional known to the family may also attend. There may be situations where, for pragmatic reasons, or because of the nature of the death a joint visit is not possible or appropriate, or where the police need to visit the scene of death early to gather forensic evidence.
Ongoing Information Sharing
Further information will need to be gathered to support the investigation into the cause and circumstances of death. All practitioners play a role in this and must be prepared to share information with other members of the multi-agency team.
The senior investigating officer (SIO) and on-call paediatrician should agree who will take the lead for collating information and sharing this with the coroner. Information will be gathered through a process of history taking, which may require more than one interview with the parents.
As far as possible, repeated questioning by different professionals should be avoided and parents interviewed jointly by police and health staff where appropriate. Information should be gathered from the primary care team and all other professionals who may know the child or family, including The Midwife, Health Visitor, School Nurse, social care and education where appropriate. All relevant records should be retrieved and reviewed by a lead professional in each agency.
The Post-Mortem Examination
Generally, most post-mortem examinations will be performed at the John Radcliffe Hospital in Oxford. If any concerns have been raised about the possibility of neglect or abuse having contributed to the child’s death, or the pathologist becomes concerned about such a possibility during the post-mortem examination, the paediatric pathologist should be accompanied by a forensic pathologist and a joint post-mortem examination protocol should be followed with the attendance of a senior investigating police officer.
Prior to commencing the post-mortem examination, the pathologist should be given a full written briefing on the history and the physical findings at presentation, and the findings of the death scene investigation. The senior investigating officer will ensure child’s ‘red book’ is secured and shared with the pathologist.
Any photographs or video recordings of the child or the scene should be made available to the pathologist. The pathologist should also be provided with a report and/or images from the radiographer for any radiological investigations. If required, skeletal surveys are performed at the time of the post-mortem examination.
The coroner should be provided with a copy of the history proforma. Where possible there should be an information sharing discussion between the consultant paediatrician and the pathologist before the post-mortem examination to identify outstanding issues and to ensure accurate understanding of information.
If the paediatrician has arranged any laboratory investigations before death, the pathologist and the coroner should be informed prior to the post-mortem examination, and the results made available as soon as possible.
Following the post-mortem examination, there should be a further discussion between the paediatrician, the pathologist, the senior investigating officer (SIO), a lead representative from children’s social care and the coroner’s officer to review any preliminary findings and decide on any further investigations required. If initial post-mortem examination findings are shared with the family, this MUST be done with the coroner’s consent.
The final report of the post-mortem examination should be sent to the coroner immediately once the final result is known. With the prior consent of the coroner, a copy of the post-mortem examination report will also be sent simultaneously to the responsible paediatrician. The post-mortem report will also be shared with Buckinghamshire CDOP (WTSC 23 p.149).
The Joint Agency Response (JAR) Meeting
The on-call Paediatrician or a deputy will convene a Joint Agency Response Meeting. This meeting will take place within 2 working days of an unexpected death. It must be convened prior to a post-mortem taking place so that information gathered at this meeting can be shared with the coroner to aid his investigation.
In cases where the process is interrupted by a weekend it may be necessary to hold this meeting early in the following week. This is in order that agencies which may hold information about the child (e.g. GP, Health Visitor, community midwife, ambulance crew, etc) will be able to attend. In these instances, it is critical that police, social work and the on-call paediatrician share information over the weekend period so that any information which comes to light over the weekend can be acted upon promptly. In other words, the JAR Meeting should not be viewed as the first opportunity to share information and if an agency becomes concerned it should share those concerns immediately.
The Joint Agency Response Meeting may include representation from:
The meeting should be minuted by one of the paediatric secretaries. A draft agenda for the meeting including specific areas to be covered in the discussion can be found as per the relevant health provider documentation ordinarily used.
The purposes of this meeting are:
If child protection concerns are identified when the information is shared, a Strategy Meeting will be convened by Children’s Social Care as per child protection procedures, and the Director of Children’s Social Care or equivalent will be notified.
Approved minutes will be shared with each of the attendees, the coroner’s office, the SUDC paediatrician and the Child Death Overview Panel as per Social Care CDOP Reporting Form B returns. They should be distributed within 1 week of the meeting for comments/amendment. The minutes should then be saved as part of the child’s medical record.
Parental consent is not required for this information to be passed to the designated paediatrician and CDOP. However it should only be shared with those who need to know governed by the Caldicott Principles, the Data Protection Act and Working Together.
Agency Report Form (Previously Form B)
Following the JAR meeting it is the responsibility of the on-call paediatrician to ensure that an Agency Report Form is submitted to Buckinghamshire CDOP and that any professionals who have not contributed to the JAR Meeting are identified. They should be invited to complete an independent agency report form on CDOP. This can be coordinated through the Buckinghamshire CDOP admin team. The Buckinghamshire CDOP admin team will send an invitation to fill out the reporting form via email. The reporting form should be completed online within 28 days of the child’s death.
DATIX and Serious Incidents
All unexpected deaths should be reported via internal agency reporting systems for managerial consideration. The lead handler for these incidents in BHT is the SUDC paediatrician. It is the responsibility of the consultant paediatrician to ensure that this happens.
The Healthcare Safety Investigations Branch
Healthcare Safety Investigations Branch (HSIB) carries out independent investigations into safety concerns within NHS funded care in England. It aims to be thorough, independent and impartial in its approach without apportioning blame or liability.
Separately, HSIB investigate NHS Serious Incident Investigation cases of
These investigations will continue to be characterized by a focus on learning and not attributing blame, and the involvement of the family is a key priority.
Co-ordination across investigations
It is easy for families to become lost in the parallel investigations following their child’s death. Effective co-ordination and good communication are vital to avoid additional distress to bereaved parents.
A “key worker” should be assigned to every bereaved family, to act as a single point of contact in relation to the child death review process.
In deaths where there is more than one investigation, NHS trusts should appoint a “case manager” to have oversight of procedures: ensuring that those involved are objective e.g. through engaging the Patient Advice and Liaison Service (PALS), have an understanding of statutory requirements, follow appropriate timescales, ensure parents have an opportunity to input into the process and establish how they would like to receive feedback. This is distinct from the key worker, who acts as an ongoing single point of contact for families.
The CDRM is a multi-professional meeting where all matters relating to an individual child’s death are discussed by the professionals directly involved in the care of that child during life and their investigation after death. It was previously known as a final case discussion meeting
The nature of this meeting will vary according to the circumstances of the child’s death and the practitioners involved.
| Circumstances of death | CDRM format |
| Sudden unexpected death | Final case discussion involving health, police and social care |
| Expected death in PICU | Morbidity and mortality meeting in PICU with input from local team if appropriate |
| Expected death in Neonatal Unit | Perinatal mortality (PMRT) review meeting |
| Expected death for child with life limiting illness | Morbidity and mortality meeting |
The CDRM should be:
It may be appropriate for the review to be quite brief or for the meeting to discuss one child or several children. In every case, the CDR Analysis Form C is drafted after all Form B’s are received and consolidated. Learning identified and actions points are confirmed by the Designated Dr for child death and discussed at the CDOP meeting.
In all cases, the aims of the CDRM are to:
It is the responsibility of the organisation responsible for the declaration of death to arrange the CDRM. The exception to this is when a Joint Agency Response has occurred, in which case responsibility defaults to the lead health professional.
Each child’s death requires unique consideration and where possible, should engage professionals across the pathway of care. The following professionals may be invited, depending on their ability to contribute meaningfully to a discussion on the circumstances of the child’s death:
NHS Trusts should note that, where practically possible, children’s deaths should be discussed at an individualized meeting, and that matters of morbidity should be considered separately. It is only through such a comprehensive approach that the contributory factors to death can be understood. (See case examples at Appendix 1 for further illustration). If certain professionals are unable to attend, they might be invited to submit a report to the meeting.
The CDRM should be chaired by the designated doctor for child death reviews, unless he/she/they was/were directly involved in the case. At the beginning of each meeting the Chair should inquire as to conflicts of interest among the attendees. In rare cases, it may be necessary to seek a chair external to the organisation; for example, when trust has broken down between the family and health care team in the organisation where death was declared. The designated doctor for child deaths might advise in such circumstances.
In general, children who die in hospital should be discussed within the department where the child died and considered an integral part of wider clinical governance processes.
Children who die in the community might be discussed at the local GP surgery, and children who die in a hospice discussed in that centre. However, the location of the meeting might also be informed by practical considerations relating to where most of the child’s treatment took place.
CDRMs require planning and co-ordination. Organisations should ensure that those responsible for reviewing child deaths have the proper resources to ensure that meetings are held in a timely and coordinated fashion.
The meeting should take place once investigations have concluded, and reports from agencies and professionals unable to attend the meeting have been received.
The meeting should take place as soon as is practicable, ideally within three months, although serious incident investigations and the length of time it takes to receive the final post-mortem report will often cause delay.
In order to best capture the views of those directly involved, it may be beneficial to start the process as soon as possible, prior to the formal CDRM.
The CDRM should occur before any coroner’s inquest, and before the CDOP meets.
The CDRM may proceed in the context of a criminal investigation, or prosecution, in consultation with the senior investigating police officer. The meeting cannot take place if the criminal investigation is directed at professionals involved in the care of the child, when prior group discussion might prejudice testimony in court.
The CDRM is a meeting for professionals. This allows full candour among those attending, and any difficult issues relating to the care of the child can be discussed without fear of misunderstanding. Parents should not attend this meeting. However, parents should be informed of the meeting by their key worker and have an opportunity to contribute information and questions through their key worker or another professional.
At the meeting’s conclusion, there should be a clear description of what follow-up meetings have already occurred with the parents, and who is responsible for reporting the meeting’s conclusions to the family. This would generally be the child’s paediatrician, or in the case of a neonatal death, obstetrician/neonatologist. In a coroner’s investigation, such liaison should take place in conjunction with the coroner’s officers.
Buckinghamshire CDOP review the deaths of all children normally resident within the relevant local authority area. The Panel ordinarily meets five times a year and has representation from health (primary and secondary care), the Integrated Care Board, police, education, social care, the local safeguarding partnership and public health.
CDOP’s should conduct an anonymised secondary review of each death where the identifying details of the child and treating professionals are redacted. This review should be informed by a standardised output, the draft Panel Analysis Form C, from the CDRM.
The functions of CDOP include:
Families have the right to have their child’s death reviewed to
Parents and carers should be informed about and involved in the review process
Appendix 2 includes contact details for national organisations offering bereavement support.
Professionals in all agencies have a duty to support bereaved parents. When there are issues with the quality of care healthcare organisations have a “duty of candour” to explain what has happened, to apologise as appropriate, and to identify lessons to reduce the likelihood of a repeat incident.
Whether the child’s death is sudden or follows a long illness, the requirement for the following roles is universal:
The ‘key worker’
All bereaved families should be given a single, named point of contact to whom they can turn for information on the child death review process, and who can signpost them to sources of support.
It is the responsibility of the organisation where the child was certified dead to identify a key worker for the family.
The role could be taken by a range of practitioners. For example:
| Circumstances of child death | Possible key worker |
| Sudden unexpected death | Paediatric matron or member of bereavement support team |
| Expected death in child with life limiting illness | Team leader of children’s community nursing team or hospice team |
| Child with long term condition e.g. oncology patient | Clinical nurse specialist |
| Death of baby in Neonatal Unit | Matron for NNU / bereavement lead for NNU |
| Child who dies in community, not known to hospital team e.g. a suicide | Coroner’s office, family liaison officer (police) |
Regardless of professional background this person should:
An appropriate consultant neonatologist or paediatrician should also be identified after every child’s death to support the family.
This is distinct from the key worker, and might either be the doctor that the family had most involvement with while the child was alive or the designated professional on-duty at the time of death. This individual should liaise closely with the family’s key worker and arrange:
Other professionals
At the time of a child’s death, other professionals may also provide vital support to the family; these include (but are not limited to) the GP, clinical psychologist, social worker, school, family support worker, midwife, health visitor or school nurse, palliative care team, chaplaincy and pastoral support team.
In all cases, it is the duty of the key worker to ensure that there is clarity regarding each professional’s role; that the family does not receive mixed messages; and that communication is clear.
It should be remembered that bereaved parents may be in state of extreme shock when their child has died. They may not be able to process or retain information and it is common that information needs to be repeated over time. Information pertaining to the statutory process to be followed should be available in an accessible format to all bereaved families or carers (When a Child Dies – A Guide for Parents and Carers.)
Providers should be familiar with its contents in order to ensure that bereaved families and carers receive the best support possible. Staff involved with the care of a child should also be offered appropriate support.
When their child dies, bereaved parents or carers should:
Children with life-limiting conditions sometimes die following prolonged illnesses. In these situations, “parallel planning” means planning for the end-of-life care, even while active treatment is still being pursued. It often involves a palliative care team. It may involve:
For detailed guidance relating to the planning and management of end-of-life care in children with life-limiting conditions see:
Appendix 2 includes contact details for national charities who offer bereavement support for families. Local NHS services and CDOP’s may also offer specific bereavement services. The key worker should be able direct families to the most appropriate support service.
Appendix 1 – Immediate decision making proforma (opens in Word)
Appendix 2 – Sources of family support (opens as a PDF)
Appendix 3 – Joint Agency Response Agenda (opens as a PDF)