RELATED INFORMATION
Working Together to Safeguard Children 2023, Chapter 6 (Department for Education)
CONTENTS
1. Preface
The death of any child is a tragedy. Every parent has a right to have such an event properly investigated. Many sudden child deaths are the result of natural causes. However, all child deaths need to be appropriately investigated to exclude homicide, to reassure the family and ensure that future children are protected, and to satisfy wider public concerns.
This guideline is provided to support multi-agency staff working within Buckinghamshire following the death of a child or young person. It aims to give an overview of the whole Child Death Review Process and to offer specific operational guidance on the management of child deaths.
A child is defined as anyone who has not yet reached their 18th birthday. ‘Children’ therefore means ‘children and young people’ throughout. The fact that a child has reached 16 years of age, is living independently or is in further education, is a member of the armed forces, is in hospital, in prison or in a Young Offenders’ Institution, does not change his or her status or entitlement to services or protection under the Children Act 1989.
This protocol does not apply to stillbirths, unless the stillbirth occurs within the community, without any medical interventions, and a doctor is not able to issue a death certificate.
This document provides the framework for a comprehensive and sensitive enquiry aimed at establishing the cause of, and factors contributing to, all deaths in all children under 18 years, with particular attention to the management of sudden, unexpected deaths. This guidance is not intended to be prescriptive, but endeavours to provide advice to practitioners who are confronted with these tragic circumstances.
Professionals need to strike a balance between the sensitivities of handling the bereaved parents and securing and preserving evidence, which may aid them in arriving at an understanding of why a child has died.
When dealing with an unexpected or unexplained child death, all agencies need to follow five common, equally important, principles:
- A sensitive, open-minded and balanced approach
- An inter-agency response
- Sharing of information
- An appropriate response to the circumstances
- Preservation of evidence.
2. Management of Child Deaths and Child Death Reviews (CDR)
2.1 Overview of the Child Death Review process
The purposes of the Child Death Review process are:
- To establish, where possible, cause(s) of death
- To identify any potential contributory factors
- To provide ongoing support to the family
- To learn lessons in order to reduce the risks of future child deaths.
There are two inter-related processes for reviewing child deaths:
- A local, multiagency agency review by an appropriate group of key professionals
- An overview of all child deaths (under 18 years) in the safeguarding partnership area(s).
Summary of Child Death Review process
(Click on the image to increase size)
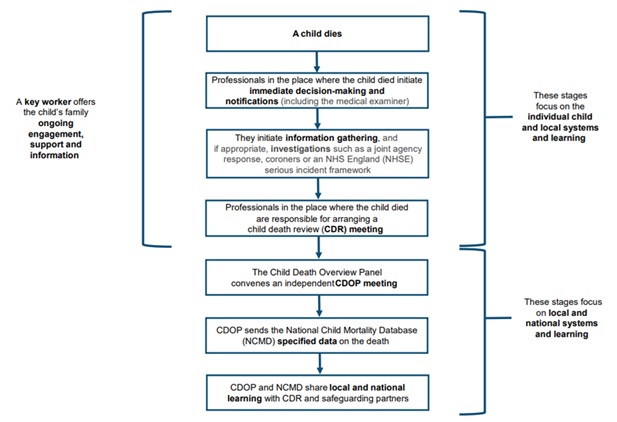
2.2 Immediate decision making and notifications
Several decisions need to be made by professionals in the hours immediately following the death of a child. These include:
- how best to support the family
- whether the death meets the criteria for a Joint Agency Response
- whether a death certificate can be issued
- whether a referral to the coroner is required
- whether the death meets the criteria for an NHS Patient Safety Incident Reporting Framework (PSIRF) investigation
A number of notifications should also be made: to the child’s GP and other professionals; to the Child Health Information System; and the relevant Child Death Review partners (as a minimum police and social care) and the Child Death Overview Panel (CDOP).
Investigation and information gathering
Following the notification of a child death, a number of investigations may then follow. These include:
- Coronial investigation
- Joint Agency Response
- NHS Patient Safety Incident Reporting Framework (PSIRF).
Post-mortem examinations may be required in some cases. Which investigations are necessary will vary depending on the circumstances of the individual case. They may run in parallel, and timeframes will vary greatly from case to case.
Child Death Review Meeting (CDRM)
Although investigations following the death of a child will vary, every child’s death should be discussed at a Child Death Review Meeting. This is the multi-professional meeting attended by professionals directly involved in the care of that child during life and those involved in the investigation after death.
The nature of this meeting will vary according to the circumstances of the child’s death and the practitioners involved.
Review of Child Deaths at a Child Death Overview Panel (CDOP)
Child Death Overview Panels (CDOP’s) are responsible for reviewing information on all child deaths. Information from the above investigations is fed into the CDOP for final review. In Buckinghamshire there are two CDOP’s. One operates in Milton Keynes and the other one is a joint Panel between Buckinghamshire and Oxfordshire (as per requirements for the minimum numbers of cases). The CDOP for Buckinghamshire contains representation from the Integrated Care Board (ICB), Children’s Social Care, Thames Valley Police, the Buckinghamshire Coroner’s Office, Public Health, South Central Ambulance Service, Midwifery and Education. In addition the Paediatric Liaison Nurse and Designated Doctor for Child Death Reviews in Buckinghamshire also attend.
Child death review processes have been mandatory since April 2008.
Support for the family
Supporting and engaging the family who have lost a child is of prime importance throughout the whole child death review process. Recognizing the complexity of the process, and the different emotional responses that bereavement can bring, families should be given a single, named point of contact, i.e. the “key worker”, for information on the processes following their child’s death, and who can signpost them to sources of support.
2.3 Immediate actions
Multiagency discussion and planning are required within the first few hours following notification of a child’s death. Necessary discussions may be face-to-face or by telephone and should engage the following professionals:
- The Medical Examiner
- Other professionals as appropriate; for example:
- the on-call paediatrician
- police
- duty social worker
Information about the circumstances of the child’s death and medical and social background should be sought to aid with the following:
- Identifying how best to support the family
- Issuing a Medical Cause of Death Certificate (MCCD). If this is not possible, consider whether the death should be referred to the coroner (see, Section 2.4 Issuing a MCCD referral to the coroner)
- Deciding whether a Joint Agency Response is required (see Section 3.2, Joint Agency Response)
- Identifying issues relating to health care or service delivery
- Determining actions to ensure the health and safety of others (e.g. family or community members, other patients and staff)
- In all deaths, these discussions should be recorded on a relevant proforma (see Appendix 1).
The outcome of these discussions should also be fed back to the family.
2.4 Issuing a MCCD referral to the coroner
- The cause of death for most children is known, and an MCCD can be issued shortly after death. See Medical certificate of cause of death (MCCD): guidance for medical practitioners (gov.uk).
- Two versions of the death certificate exist
- a neonatal certificate (up to 28 days)
- the standard certificate.
- In deaths of children with pre-existing complex medical conditions, correct wording of the death certificate may need to be discussed with the specialist team.
- If it is not possible to sign the MCCD then the case should be referred to the coroner.
- The Chief coroner has issued guidance on which deaths should be reported to the coroner (see Section 3.1 Coronial investigation). If there is any uncertainty over whether a referral is necessary, the attending doctor should contact the coroner’s office to discuss.
- Two versions of the death certificate exist
2.5 The Post-Mortem Examination
A post-mortem examination is sometimes required as part of a coronial investigation. If a coroner requires a post-mortem examination parental consent is not required and parents cannot refuse the examination.
In cases where a death certificate can be issued a hospital post-mortem examination (PM) may still provide important information as to why a child has died. It is therefore important to explore the issue with the family at the time of death, even in cases where the coroner does not require a PM.
2.6 Informing the Child Death Overview Panel
This should be completed electronically filling out a notification form within 24 hours of the death (or next working day). This is done via the Oxfordshire Buckinghamshire eCDOP website login using the “Submit Notification form A”:
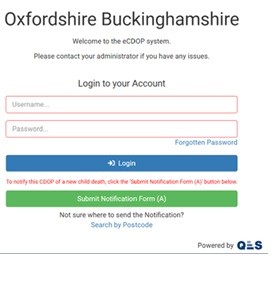
For all deaths essential information regarding demographics, circumstances of death and background medical history should be submitted to CDOP via the reporting form (previously Form B).
2.7 Other notifications
The following people should also be notified within 24 hours (or the next working day) of the child’s death:
- General Practitioner – inform the GP of the fact and circumstances of the death, so that the GP can support the family
- Other professionals, as appropriate – community midwives, health visitor, school nurse, hospital/community medical team.
3. Investigating and Information Gathering
The nature of the investigation(s) varies with individual circumstances. They may include:
- A Coronial Investigation
- A Joint Agency Response
- A NHS Patient Safety Incident Reporting Framework (PSIRF)
- A Local Child Safeguarding Practice Review (LCSPR)
For all deaths essential information regarding demographics, circumstances of death and background medical history should be submitted to CDOP via the Notification Reporting Form A process. Oxfordshire/Buckinghamshire eCDOP website log-in.
3.1 Coronial investigation
Informing the coroner
The coroner’s office must be informed of all ‘unexpected’ deaths via 01494 475505 (call Thames Valley Police on 101 out of hours). Once the death has been declared, the coroner assumes immediate responsibility for the body. Samples may be taken post-mortem as outlined in the BHT Policy.
Anyone can refer a death to the coroner for investigation. Reasons for referral are as follows:
- the cause of death is unknown
- the deceased was not seen by the certifying doctor either after death or within 14 days before death
- the death was violent or suspicious
- the death was unnatural
- the death may be due to an accident (whenever it occurred)
- the death may be due to self-neglect or neglect by others
- the death may be due to an abortion
- the death occurred during an operation or before recovery from the effects of an anaesthetic
- the death may be a suicide
- the death occurred during or shortly after detention in police or prison custody
- the death occurred while the deceased was subject to compulsory detention under the Mental Health Act or a Deprivation of Liberty Safeguards authorisation (DoLS)
- Deaths that may be lined to medical treatment, surgery or anaesthetic
- for any other concerning feature.
They may order a post-mortem (PM) examination, if necessary. Following the PM, the body of the child is usually promptly released back to their family for the death to be registered and funeral arrangements to be made. Release may however be later if organs or tissues have been taken for analysis, or if a second independent post-mortem examination is required.
Not all deaths reported to the coroner proceed to inquest although most unexplained deaths of children do. The inquest aims to determine the identity of the person that died and how, when and where they came by their death. The coroner will examine the evidence and, commonly without a jury, record the answers to the questions listed on a public document called the Record of Inquest. The details of the coroner’s findings are forwarded to the local registrar.
All agencies holding pertinent information are under a duty to disclose such information.
The family should be informed early on of the coroner’s involvement, and the need for and timing of a post-mortem examination, their right to be represented at the examination should they so wish, whether an investigation or inquest has been opened so that they may attend the inquest opening and the dates of any investigation reviews, pre-inquest reviews and the inquest itself.
Once the jurisdiction of the coroner is engaged, the coroner’s officer is the main point of contact with the family for matters relating to the coronial process.
3.2 Joint Agency Response (JAR)
All deceased children that meet the criteria for a JAR should be transferred to the nearest appropriate Emergency Department (ED) to enable the JAR to be triggered.
A Joint Agency Response should be triggered if a child’s death:
- is or could be due to external causes
- is sudden and there is no immediately apparent cause
- (including Sudden Unexplained Death in Infancy/Childhood);
- occurs in custody, or where the child was detained under the Mental Health Act
- suspicion of unnatural causes
- in the case of a stillbirth with no healthcare professional in attendance
In any of these circumstances, the on-call paediatrician at Stoke Mandeville Hospital, (pager 593), police investigator, and duty social worker should be contacted immediately to initiate the Joint Agency Response.
A Joint Agency Response should also be triggered if such children are brought to hospital near death, are successfully resuscitated, but are expected to die in the following days. This enables an accurate history of events to be taken and, if necessary, a ‘scene of collapse’ visit to occur. Appropriate clinical investigations should also be performed in such cases.
A lead health professional should be assigned. This will usually be the on-call paediatrician. This person will ensure that all health responses are implemented and be responsible for on-going liaison with the police and other agencies.
Flowchart setting out the sequence of events that should unfold in a Joint Agency Response. A Joint Agency Response can be divided into three separate phases:
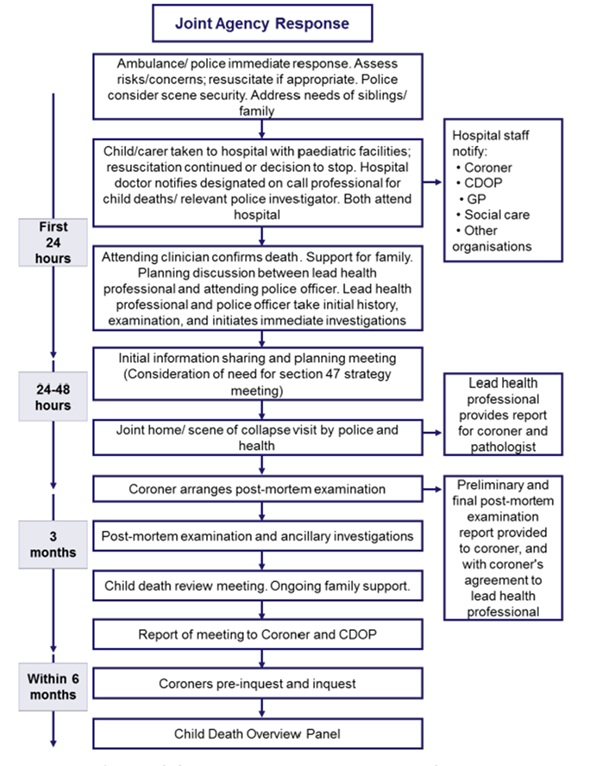
At each stage in the process, explicit consideration must be given as to whether child abuse / neglect may have been a contributory factor.
Immediate response (within a few hours)
-
- Caring for the Family
- Initial History taking
- Initial examination
- Initial laboratory investigations/samples
- Immediate Information sharing/planning
- Early Response (within a few days) NHS Patient Safety Incident Reporting Framework (PSIRF)
- Ongoing information gathering
- Home visit by police
- Initial Case Discussion Meeting
- Post-mortem examination
- Late Response
- Child Death Review Meeting (See Section 4)
Immediate response
Normally following an unexpected death, a child will be transferred by the ambulance service to Stoke Mandeville Hospital. The emergency providers attending the scene should assess the child and, unless it is clearly inappropriate, should attempt resuscitation and transfer the child and family to hospital. The child should never be taken straight to the mortuary unless directed by the police in consultation with the coroner. In such cases the police are responsible for notifying the consultant paediatrician on-call.
On arrival at hospital, a member of the nursing staff will be allocated to the family. On arrival at the A&E department the consultant paediatrician and/or senior doctor in A&E should be informed. Immediate responsibility for informing and providing appropriate care and support of the family rests with the on-call paediatric team. Resuscitation should continue as appropriate and any decision to stop will be made by an experienced medical practitioner with input from other members of the resuscitation team and in consultation with the family. As soon as practicable after arrival at a hospital, the child should be examined by the consultant paediatrician or delegated senior paediatrician on-call.
When the child is pronounced dead, the paediatric or A&E consultant or delegated senior clinician should inform the parents, having first reviewed all the available information. S/he/they should explain future police and coronial involvement, including the coroner’s authority to order a post-mortem examination. This may involve taking tissue blocks and slides to ascertain the cause of death.
Caring for the family
Initial bereavement support will be provided by hospital staff. This is a difficult time for everyone. The time spent with the family may be brief, but actions will greatly influence how the family deals with the bereavement for a long time afterwards. Remember that families are in the first stages of grief. They may be shocked, numb, withdrawn, angry or hysterical. Every effort should be made to conduct discussions in a private and sympathetic environment away from interruptions.
Communication should be clear, sensitive and honest. Parents should be treated with compassion, respect and dignity.
Where parents do not understand and/or speak English well, an independent interpreter should be called – one can be arranged via switchboard. The interpreter should not normally be a family member. However, urgent information about the child could be sought from a family member whilst awaiting an interpreter to arrive.
Staff caring for families after a child’s death should be offered support through a formal debrief system and counselling via the Workplace Health Department, as appropriate.
Ongoing bereavement care is available from a range of agencies. Further details can be found in Appendix 2.
For lactating mothers please consider liaising with the medical team involved for the purposes of possible prescription to supress lactation.
Initial history taking
Most of the medical and social history will be obtained during the initial discussion with the parents in the A&E Department. This is supplemented by information obtained at the home visit. All professionals should record history and background information given by parents/carers in as much detail as possible.
It is crucial that under no circumstances should professionals challenge or make comment on the history given by a parent/carer – if challenged or a comment is made parents/carers may form the impression that their account is not believed and may subsequently change their story. This could hinder any police investigation.
If there are other children, enquire about their whereabouts and who is caring for them. A surviving twin should automatically be offered admission for monitoring and investigation.
Immediate information sharing / planning
A Joint Agency Response meeting for children who normally reside within Bucks and who die in Bucks will be coordinated by the on-call paediatric team at Stoke Mandeville Hospital. These deaths should be notified to the on-call paediatrician by telephone. The consultant paediatrician on-call is responsible for instigating the Joint Agency Response and must ensure that police, social care and other appropriate agencies have been notified.
For children who reside in Buckinghamshire who have died at the John Radcliffe hospital in Oxford the paediatric team at Stoke Mandeville Hospital will coordinate the Joint Agency Response. These deaths should be notified in the first instance to the on-call paediatrician at Stoke Mandeville Hospital, who will then liaise with the Designated Doctor for Child Death Reviews (or in their absence the Named Doctor for Safeguarding).
For children who reside in Buckinghamshire who have died at a tertiary centre other than Oxford (e.g. GOSH, Birmingham etc), the initial response should be dealt with by the team within that centre. The paediatricians at Stoke Mandeville do not coordinate the investigation but may be called upon to attend meetings (e.g. case discussion/case review meetings) at the tertiary centre. They may also be called upon to submit a “Reporting form B” about the child to the Bucks CDOP.
For children dying within Buckinghamshire who normally reside elsewhere, the paediatric team will coordinate a Joint Agency Response as for a Buckinghamshire child, submitting information to the child’s local CDOP as appropriate. The exception to this would be a child from Oxfordshire. These cases should be notified to the SUDIC Paediatrician at the John Radcliffe or to the CDOP administrator for Oxfordshire (both available via the John Radcliffe Switchboard).
If there is any uncertainty about whether a Joint Agency Response is required, or who should convene one, it is imperative that it be discussed with the SUDIC paediatrician as a matter of urgency. If the SUDIC paediatrician is on leave then this should be discussed with the Named Doctor for Child Protection.
Early contact and discussion between key agencies is essential. Discussion should focus on whether the death may have been caused by abuse or neglect. In such cases the safety of siblings must be considered. Consideration should be given to securing the scene where the child died. Discussion about the need for a home/scene visit should take place early on between the police officer and the on-call paediatrician, enabling the prompt recovery of evidence that otherwise could be lost. A home visit will almost always be required in deaths under the age of 2 years. Paediatricians do not currently participate in home visits. The photographs from home visits can be shared and discussed by the team during the Joint Agency Response meeting.
Contact with police and social work should be clearly documented in the notes. No professional should assume they have been contacted. Repeated calls are better than none at all. If the death is suspicious or significant concerns are raised at any stage about the possibility of abuse or neglect, a decision will be taken for the police to become the lead agency and take primacy in the investigation.
On receiving notification of an unexpected child death, a senior police officer will be designated as the Senior Investigating Officer (SIO). It is important to stress to the family that the involvement of the police is routine and does not assume suspicion. However, staff need to be aware that on occasions, in suspicious circumstances, the early arrest of the parents/carers may be essential to secure and preserve evidence as part of an investigation.
Early response (within a few days)
The home or scene visit
For all children less than 2 years of age who have died suddenly and unexpectedly, a home visit should be undertaken within 24 hours (usually the same day). For older children the need for a home visit should be discussed between the police and the paediatric team. The home visit is usually conducted by the police. The home visit provides an opportunity to take a more careful history, to inspect the death scene and to try and alleviate some of the family’s concerns.
The purposes of the home or scene visit are to:
- Review the history taken in ED
- Evaluate the environment where the child died
- Support the family
- Update the family on the investigation. The discussion with parents about the details of the post-mortem examination should be done in conjunction with coroner’s officers.
Where the location of the death is different to the home address of the child, an additional visit to the home address may be arranged if deemed necessary. Consideration should be given as to which professionals should attend the visit. Normally this will be the senior investigating officer. Where possible a member of the primary care team, or some other professional known to the family may also attend. There may be situations where, for pragmatic reasons, or because of the nature of the death a joint visit is not possible or appropriate, or where the police need to visit the scene of death early to gather forensic evidence.
Ongoing Information Sharing
Further information will need to be gathered to support the investigation into the cause and circumstances of death. All practitioners play a role in this and must be prepared to share information with other members of the multi-agency team.
The senior investigating officer (SIO) and on-call paediatrician should agree who will take the lead for collating information and sharing this with the coroner. Information will be gathered through a process of history taking, which may require more than one interview with the parents.
As far as possible, repeated questioning by different professionals should be avoided and parents interviewed jointly by police and health staff where appropriate. Information should be gathered from the primary care team and all other professionals who may know the child or family, including The Midwife, Health Visitor, School Nurse, social care and education where appropriate. All relevant records should be retrieved and reviewed by a lead professional in each agency.
The Post-Mortem Examination
Generally, most post-mortem examinations will be performed at the John Radcliffe Hospital in Oxford. If any concerns have been raised about the possibility of neglect or abuse having contributed to the child’s death, or the pathologist becomes concerned about such a possibility during the post-mortem examination, the paediatric pathologist should be accompanied by a forensic pathologist and a joint post-mortem examination protocol should be followed with the attendance of a senior investigating police officer.
Prior to commencing the post-mortem examination, the pathologist should be given a full written briefing on the history and the physical findings at presentation, and the findings of the death scene investigation. The senior investigating officer will ensure child’s ‘red book’ is secured and shared with the pathologist.
Any photographs or video recordings of the child or the scene should be made available to the pathologist. The pathologist should also be provided with a report and/or images from the radiographer for any radiological investigations. If required, skeletal surveys are performed at the time of the post-mortem examination.
The coroner should be provided with a copy of the history proforma. Where possible there should be an information sharing discussion between the consultant paediatrician and the pathologist before the post-mortem examination to identify outstanding issues and to ensure accurate understanding of information.
If the paediatrician has arranged any laboratory investigations before death, the pathologist and the coroner should be informed prior to the post-mortem examination, and the results made available as soon as possible.
Following the post-mortem examination, there should be a further discussion between the paediatrician, the pathologist, the senior investigating officer (SIO), a lead representative from children’s social care and the coroner’s officer to review any preliminary findings and decide on any further investigations required. If initial post-mortem examination findings are shared with the family, this MUST be done with the coroner’s consent.
The final report of the post-mortem examination should be sent to the coroner immediately once the final result is known. With the prior consent of the coroner, a copy of the post-mortem examination report will also be sent simultaneously to the responsible paediatrician. The post-mortem report will also be shared with Buckinghamshire CDOP (WTSC 23 p.149).
The Joint Agency Response (JAR) Meeting
The on-call Paediatrician or a deputy will convene a Joint Agency Response Meeting. This meeting will take place within 2 working days of an unexpected death. It must be convened prior to a post-mortem taking place so that information gathered at this meeting can be shared with the coroner to aid his investigation.
In cases where the process is interrupted by a weekend it may be necessary to hold this meeting early in the following week. This is in order that agencies which may hold information about the child (e.g. GP, Health Visitor, community midwife, ambulance crew, etc) will be able to attend. In these instances, it is critical that police, social work and the on-call paediatrician share information over the weekend period so that any information which comes to light over the weekend can be acted upon promptly. In other words, the JAR Meeting should not be viewed as the first opportunity to share information and if an agency becomes concerned it should share those concerns immediately.
The Joint Agency Response Meeting may include representation from:
- Health
- The on-call Paediatrician/SUDC Paediatrician
- Senior members of the children’s nursing team
- Ambulance service/A&E staff/Intensive care/Anaesthetists
- The named health visitor, children’s community nurse or school nurse
- The community midwife
- The general practitioner
- Children’s/Adult (for parents) Mental Health teams
- Social Work – The children’s social care team manager or appropriate deputy
- Police – The Senior Investigating Officer or an appropriate deputy
- Other contributors
- coroner’s officer
- Education (where the child was attending school or nursery)
- The named professionals for Child Protection
- Mental health professionals (CPN or consultant psychiatrist)
- Any other agency known to the child/family e.g. drug/alcohol services.
The meeting should be minuted by one of the paediatric secretaries. A draft agenda for the meeting including specific areas to be covered in the discussion can be found as per the relevant health provider documentation ordinarily used.
The purposes of this meeting are:
- Information Sharing and Analysis
- Each agency will share information regarding circumstances of the child’s death and any background information they hold
- Consider any evidence of child abuse, neglect or poor parental care/supervision.
- To collate all relevant information to share with the pathologist.
- To identify factors which may have contributed to the child’s death
- Investigation Planning
- To determine which professional/agency will lead the multi-agency investigation.
- To plan and determine the process of the investigation. Each of the following questions must be asked and their answers recorded.
- Is the death suspicious, requiring a police investigation?
- Does the death constitute a serious untoward incident?
- Is consideration of a Local Child Safeguarding Practice Review required?
- Management Planning
- To ensure a coordinated bereavement care plan for the family. This should include nominating a professional to share the results of the post- mortem examination.
- To enable consideration of any child safeguarding risks to siblings/any other children living in the household and to consider the potential need for child protection procedures.
- To discuss any need for action in respect of other children in the wider household or family (e.g. health overview).
If child protection concerns are identified when the information is shared, a Strategy Meeting will be convened by Children’s Social Care as per child protection procedures, and the Director of Children’s Social Care or equivalent will be notified.
Approved minutes will be shared with each of the attendees, the coroner’s office, the SUDC paediatrician and the Child Death Overview Panel as per Social Care CDOP Reporting Form B returns. They should be distributed within 1 week of the meeting for comments/amendment. The minutes should then be saved as part of the child’s medical record.
Parental consent is not required for this information to be passed to the designated paediatrician and CDOP. However it should only be shared with those who need to know governed by the Caldicott Principles, the Data Protection Act and Working Together.
Agency Report Form (Previously Form B)
Following the JAR meeting it is the responsibility of the on-call paediatrician to ensure that an Agency Report Form is submitted to Buckinghamshire CDOP and that any professionals who have not contributed to the JAR Meeting are identified. They should be invited to complete an independent agency report form on CDOP. This can be coordinated through the Buckinghamshire CDOP admin team. The Buckinghamshire CDOP admin team will send an invitation to fill out the reporting form via email. The reporting form should be completed online within 28 days of the child’s death.
DATIX and Serious Incidents
All unexpected deaths should be reported via internal agency reporting systems for managerial consideration. The lead handler for these incidents in BHT is the SUDC paediatrician. It is the responsibility of the consultant paediatrician to ensure that this happens.
The Healthcare Safety Investigations Branch
Healthcare Safety Investigations Branch (HSIB) carries out independent investigations into safety concerns within NHS funded care in England. It aims to be thorough, independent and impartial in its approach without apportioning blame or liability.
Separately, HSIB investigate NHS Serious Incident Investigation cases of
- intrapartum stillbirth
- early neonatal deaths
- severe brain injuries from 37 weeks gestation
These investigations will continue to be characterized by a focus on learning and not attributing blame, and the involvement of the family is a key priority.
Co-ordination across investigations
It is easy for families to become lost in the parallel investigations following their child’s death. Effective co-ordination and good communication are vital to avoid additional distress to bereaved parents.
A “key worker” should be assigned to every bereaved family, to act as a single point of contact in relation to the child death review process.
In deaths where there is more than one investigation, NHS trusts should appoint a “case manager” to have oversight of procedures: ensuring that those involved are objective e.g. through engaging the Patient Advice and Liaison Service (PALS), have an understanding of statutory requirements, follow appropriate timescales, ensure parents have an opportunity to input into the process and establish how they would like to receive feedback. This is distinct from the key worker, who acts as an ongoing single point of contact for families.
4. The Child Death Review Meeting
4.1 Introduction
The CDRM is a multi-professional meeting where all matters relating to an individual child’s death are discussed by the professionals directly involved in the care of that child during life and their investigation after death. It was previously known as a final case discussion meeting
The nature of this meeting will vary according to the circumstances of the child’s death and the practitioners involved.
| Circumstances of death | CDRM format |
| Sudden unexpected death | Final case discussion involving health, police and social care |
| Expected death in PICU | Morbidity and mortality meeting in PICU with input from local team if appropriate |
| Expected death in Neonatal Unit | Perinatal mortality (PMRT) review meeting |
| Expected death for child with life limiting illness | Morbidity and mortality meeting |
The CDRM should be:
- flexible and proportionate
- focused on local learning
- undertaken for all Deaths (expected and unexpected)
It may be appropriate for the review to be quite brief or for the meeting to discuss one child or several children. In every case, the CDR Analysis Form C is drafted after all Form B’s are received and consolidated. Learning identified and actions points are confirmed by the Designated Dr for child death and discussed at the CDOP meeting.
4.2 Aims
In all cases, the aims of the CDRM are to:
- review the background history, treatment, and outcomes of investigations, to determine, as far as is possible, the likely cause of death
- ascertain contributory and modifiable factors in the following areas
- service delivery
- child
- social and physical environment
- describe learning arising from the death and associated actions
- review the support provided to the family
- ensure that the family are provided with
- the outcomes of any investigation into their child’s death
- an explanation of why their child died along with any learning from the review meeting. If the family’s first language is not English this may require a face-to- face meeting with a translator.
- ensure that CDOP and, where appropriate, the coroner is informed of the outcomes of any investigation into the child’s death
- review the support provided to staff involved in the care of the child.
4.3 Attendees and chair
It is the responsibility of the organisation responsible for the declaration of death to arrange the CDRM. The exception to this is when a Joint Agency Response has occurred, in which case responsibility defaults to the lead health professional.
Each child’s death requires unique consideration and where possible, should engage professionals across the pathway of care. The following professionals may be invited, depending on their ability to contribute meaningfully to a discussion on the circumstances of the child’s death:
- hospital or community healthcare staff involved with the child at the end of his/her life, and those known to the family prior to this event
- pathologist, if a post-mortem examination has taken place
- other professional peers from relevant hospital departments and community services
- patient safety team if a serious incident investigation has taken place
- coroner’s officer, if the case has been referred to the coroner
- senior investigating police officer, if there is a Joint Agency Response; or
- other practitioners for example social work, ambulance and fire services, primary care clinicians, school nurse, head teacher, representatives from voluntary organisations.
NHS Trusts should note that, where practically possible, children’s deaths should be discussed at an individualized meeting, and that matters of morbidity should be considered separately. It is only through such a comprehensive approach that the contributory factors to death can be understood. (See case examples at Appendix 1 for further illustration). If certain professionals are unable to attend, they might be invited to submit a report to the meeting.
The CDRM should be chaired by the designated doctor for child death reviews, unless he/she/they was/were directly involved in the case. At the beginning of each meeting the Chair should inquire as to conflicts of interest among the attendees. In rare cases, it may be necessary to seek a chair external to the organisation; for example, when trust has broken down between the family and health care team in the organisation where death was declared. The designated doctor for child deaths might advise in such circumstances.
4.4 Location and timing
In general, children who die in hospital should be discussed within the department where the child died and considered an integral part of wider clinical governance processes.
Children who die in the community might be discussed at the local GP surgery, and children who die in a hospice discussed in that centre. However, the location of the meeting might also be informed by practical considerations relating to where most of the child’s treatment took place.
CDRMs require planning and co-ordination. Organisations should ensure that those responsible for reviewing child deaths have the proper resources to ensure that meetings are held in a timely and coordinated fashion.
The meeting should take place once investigations have concluded, and reports from agencies and professionals unable to attend the meeting have been received.
The meeting should take place as soon as is practicable, ideally within three months, although serious incident investigations and the length of time it takes to receive the final post-mortem report will often cause delay.
In order to best capture the views of those directly involved, it may be beneficial to start the process as soon as possible, prior to the formal CDRM.
The CDRM should occur before any coroner’s inquest, and before the CDOP meets.
The CDRM may proceed in the context of a criminal investigation, or prosecution, in consultation with the senior investigating police officer. The meeting cannot take place if the criminal investigation is directed at professionals involved in the care of the child, when prior group discussion might prejudice testimony in court.
4.5 Family engagement
The CDRM is a meeting for professionals. This allows full candour among those attending, and any difficult issues relating to the care of the child can be discussed without fear of misunderstanding. Parents should not attend this meeting. However, parents should be informed of the meeting by their key worker and have an opportunity to contribute information and questions through their key worker or another professional.
At the meeting’s conclusion, there should be a clear description of what follow-up meetings have already occurred with the parents, and who is responsible for reporting the meeting’s conclusions to the family. This would generally be the child’s paediatrician, or in the case of a neonatal death, obstetrician/neonatologist. In a coroner’s investigation, such liaison should take place in conjunction with the coroner’s officers.
5. Child Death Overview Panel
5.1 Introduction
Buckinghamshire CDOP review the deaths of all children normally resident within the relevant local authority area. The Panel ordinarily meets five times a year and has representation from health (primary and secondary care), the Integrated Care Board, police, education, social care, the local safeguarding partnership and public health.
CDOP’s should conduct an anonymised secondary review of each death where the identifying details of the child and treating professionals are redacted. This review should be informed by a standardised output, the draft Panel Analysis Form C, from the CDRM.
5.2 Panel responsibilities
The functions of CDOP include:
- collation of information about each child death
- analysis of this information to
- confirm or clarify the cause of death
- determine any contributory factors
- identify learning arising that may prevent future child deaths
- to make recommendations to all relevant organisations which may prevent future child deaths
- to notify the local Safeguarding Partners in cases involving abuse or neglect
- to provide data to the National Child Mortality Database
- to produce an annual report for CDR partners outlining
- patterns and trends in child deaths
- lessons learnt and actions taken
- effectiveness of the wider child death review process; and
- to contribute to local, regional and national initiatives to improve child death reviews.
6. Family Engagement and Bereavement Support
Families have the right to have their child’s death reviewed to
- identify the cause of death
- learn lessons to prevent further children’s deaths
Parents and carers should be informed about and involved in the review process
Appendix 2 includes contact details for national organisations offering bereavement support.
Professionals in all agencies have a duty to support bereaved parents. When there are issues with the quality of care healthcare organisations have a “duty of candour” to explain what has happened, to apologise as appropriate, and to identify lessons to reduce the likelihood of a repeat incident.
Whether the child’s death is sudden or follows a long illness, the requirement for the following roles is universal:
- A key worker
- A medical lead
6.1 The team around the family
The ‘key worker’
All bereaved families should be given a single, named point of contact to whom they can turn for information on the child death review process, and who can signpost them to sources of support.
It is the responsibility of the organisation where the child was certified dead to identify a key worker for the family.
The role could be taken by a range of practitioners. For example:
| Circumstances of child death | Possible key worker |
| Sudden unexpected death | Paediatric matron or member of bereavement support team |
| Expected death in child with life limiting illness | Team leader of children’s community nursing team or hospice team |
| Child with long term condition e.g. oncology patient | Clinical nurse specialist |
| Death of baby in Neonatal Unit | Matron for NNU / bereavement lead for NNU |
| Child who dies in community, not known to hospital team e.g. a suicide | Coroner’s office, family liaison officer (police) |
Regardless of professional background this person should:
- be readily accessible point of contact for the family after the death
- help co-ordinate meetings between the family and professionals as required
- be able to provide information on the child death review process and the course of any investigations pertaining to the child
- liaise as required with the coroner’s officer and police family liaison officer
- represent the ‘voice’ of the parents at professional meetings, ensure that their questions are effectively addressed, and to provide feedback to the family afterwards; and
- signpost to expert bereavement support if required.
An appropriate consultant neonatologist or paediatrician should also be identified after every child’s death to support the family.
This is distinct from the key worker, and might either be the doctor that the family had most involvement with while the child was alive or the designated professional on-duty at the time of death. This individual should liaise closely with the family’s key worker and arrange:
- follow-up meetings at locations and times convenient to the family; and
- clinical expertise (via other professionals if necessary) to be able to:
- answer questions relating to the medical, nursing or midwifery care of the child
- explain the findings, where relevant, of the post-mortem examination and/or other investigations and
- report back the outcome from the CDRM.
Other professionals
At the time of a child’s death, other professionals may also provide vital support to the family; these include (but are not limited to) the GP, clinical psychologist, social worker, school, family support worker, midwife, health visitor or school nurse, palliative care team, chaplaincy and pastoral support team.
In all cases, it is the duty of the key worker to ensure that there is clarity regarding each professional’s role; that the family does not receive mixed messages; and that communication is clear.
6.2 What can bereaved families expect when their child dies?
It should be remembered that bereaved parents may be in state of extreme shock when their child has died. They may not be able to process or retain information and it is common that information needs to be repeated over time. Information pertaining to the statutory process to be followed should be available in an accessible format to all bereaved families or carers (When a Child Dies – A Guide for Parents and Carers.)
Providers should be familiar with its contents in order to ensure that bereaved families and carers receive the best support possible. Staff involved with the care of a child should also be offered appropriate support.
When their child dies, bereaved parents or carers should:
- have the opportunity to spend time with the child’s body in a quiet and private environment
- have the opportunity to make memories including taking photographs, hand and footprints and a lock of hair
- expect a member of staff to remain with them, to provide comfort, and to ensure their basic needs are met. In cases where there are suspicious circumstances it will be necessary to have a staff member with the body of the child when the parents are present.
- be given the contact details of their key worker and the identity of their medical lead, be informed who will be contacting them and when they will be contacted after they leave the hospital or hospice (and what to do should they have any questions in the meantime)
- know how to make arrangements to view their child’s body
- be given information on death registration and the coronial process (if applicable)
- understand why a post-mortem examination may be indicated and, if so, where it is taking place, and when the results might be expected. In the event of a coroner’s case this responsibility falls to the coroner’s officer
- be supported to understand the child death review process and how they are able to contribute to it
- be given practical advice in respect to organising the child’s funeral
- have the key worker accompany them to meetings to provide practical and emotional support
- be able to access expert bereavement support if required (see Appendix 2).
6.3 Planning prior to death for life-limiting conditions
Children with life-limiting conditions sometimes die following prolonged illnesses. In these situations, “parallel planning” means planning for the end-of-life care, even while active treatment is still being pursued. It often involves a palliative care team. It may involve:
- identifying a ‘team around the family’
- writing an advance care plan
- giving thought to cultural and religious requirements
For detailed guidance relating to the planning and management of end-of-life care in children with life-limiting conditions see:
- NICE guidance 61; end of life care for infants, children and young people with life-limiting conditions: planning and management
- Together for Short Lives: core care pathway for children with life-limiting conditions
- Together for Short Lives: perinatal pathway for babies with palliative care needs.
6.4 When a child dies in the emergency department (ED)
- When children die or are certified dead in the emergency department (ED) there will usually be a Joint Agency Response (see Section 3.2, Joint Agency Response). In such circumstances, the same expectations apply relating to identifying a ‘team around the family’.
- Responsibility for ensuring that appropriate care is provided to the family falls to the organisation in which the child is certified dead. Detailed guidance relating to support for the family in such situations is provided in the SUDI/C Guidelines.
6.5 When a child dies and a Patient Safety Incident Response Framework (PSIRF) is instigated
- Where concerns about service delivery have been raised a PSIRF investigation may be required. Parents can provide vital insight into the circumstances of the death and quality of care received.
- In such cases, a “case manager” will support the key worker in having oversight of the various processes, tracking timelines, and ensuring commitments to the family are met.
6.6 Support for parents, families and carers
Appendix 2 includes contact details for national charities who offer bereavement support for families. Local NHS services and CDOP’s may also offer specific bereavement services. The key worker should be able direct families to the most appropriate support service.
Appendices
Appendix 1 – Immediate decision making proforma (opens in Word)
Appendix 2 – Sources of family support (opens as a PDF)
Appendix 3 – Joint Agency Response Agenda (opens as a PDF)